
Abstract
Objective
While narcotics remain the backbone of perioperative analgesia, the adjunctive role of other analgesics, including non-steroidal anti-inflammatory drugs (NSAIDs), is being recognized increasingly. This meta-analysis sought to determine whether adjunctive NSAIDs improve postoperative analgesia and reduce cumulative narcotic requirements.
Methods
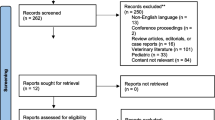
A comprehensive search was undertaken to identify all randomized trials, in cardiothoracic patients, of NSAIDs plus narcotics vs narcotics without NSAIDs. Medline, Cochrane Library, EMBASE, and abstract databases were searched up to September 2005. The primary outcome was visual analogue scale (VAS) pain score. Secondary outcomes included 24-hr cumulative morphine-equivalents, rescue medications required, mortality, myocardial infarction, atrial fibrillation, stroke, renal failure, hospital readmissions, and in-hospital costs.
Results
Twenty randomized trials involving 1,065 patients were included. A significant reduction in 24-hr VAS pain score was found in patients receiving NSAIDs [weighted mean difference (WMD) -0.91 points, 95% confidence interval (CI) -1.48 to -0.34 points]. In addition, patients required significantly less morphine-equivalents in the first 24 hr (WMD -7.67 mg, 95% CI -8.97 to -6.38 mg). No significant difference was found with respect to mortality [odds ratio (OR) 0.19, 95% CI 0.01 to 4.22], myocardial infarction (OR 0.71, 95% CI 0.09 to 5.71), renal dysfunction (OR 0.95, 95% CI 0.37 to 2.46), or gastrointestinal bleeding (OR 0.96, 95% CI 0.13 to 7.09).
Conclusion
In patients less than 70 yr of age undergoing cardiothoracic surgery, the adjunctive use of NSAIDs with narcotic analgesia reduces 24-hr VAS pain score and narcotic requirements.
Résumé
Objectif
Les narcotiques demeurent le pivot de ľanalgésie périopératoire, mais le rôle complémentaire ďautres analgésiques, dont les anti-inflammatoires non stéroidiens (AINS), est de plus en plus reconnu. La présente méta-analyse veut déterminer si les AINS ďappoint améliorent ľanalgésie postopératoire et réduisent les besoins cumulatifs de narcotiques.
Méthode
Nous avons recensé toutes les études randomisées sur des narcotiques, complétés ou non par des AINS, réalisées auprs de patients de cardiochirurgie thoracique. Les bases Medline, Cochrane Library, EMBASE et les résumés parus jusqu’à septembre 2005 ont été explorés. Le principal paramtre recherché était le score de douleur à ľéchelle visuelle analogique (EVA). Les paramtres secondaires étaient la consommation cumulative, sur 24 h, ďanalgésiques en équivalents-morphine, les besoins de médicaments ďappoint, la mortalité, la présence ďinfarctus du myocarde, la fibrillation auriculaire, ľaccident vasculaire, ľinsuffisance rénale, la réadmission hospitalire et le coût de ľhospitalisation.
Résultats
Vingt études randomisées regroupant 1 065 patients ont été retenues. Une réduction significative des scores de douleur, sur 24 h, a été trouvée chez ceux qui recevaient des AINS [différence moyenne pondérée (DMP) -0,91 points, intervalle de confiance de 95 % (IC) -1,48 à -0,34 points]. De plus, les patients ont demandé sensiblement moins ďéquivalents-morphine au cours des 24 premires heures (DMP -7,67 mg, IC de 95 % -8,97 à -6,38 mg). Il n’y avait aucune différence significative quant à la mortalité [risque relatif (RR) de 0,19, IC de 95 % 0,01 à 4,22], à ľinfarctus du myocarde (RR 0,71, IC de 95 % 0,09 à 5,71), à ľinsuffisance rénale (RR 0,5, IC de 95 % 0,37 à 2,46) ou au saignement gastrointestinal (RR 0,96, IC de 95 % 0,13 à 7,09).
Conclusion
Chez les patients de moins de 70 ans qui subissent une opération cardiothoracique, ľusage ďAINS ďappoint avec ľanalgésie aux narcotiques réduit la douleur et les besoins de narcotiques sur 24 h.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Stenseth R, Bjella L, Berg EM, Christensen O, Levang OW, Gisvold SE. Effects of thoracic epidural analgesia on pulmonary function after coronary artery bypass surgery. Eur J Cardiothorac Surg1 1996; 10: 859–65; discussion 866.
Reinhart K, Foehring U, Kersting T, et al. Effects of thoracic epidural anesthesia on systemic hemodynamic function and systemic oxygen supply-demand relationship. Anesth Analg 1989; 69: 360–9.
Pastor MC, Sanchez MJ, Casas MA, Mateu J, Bataller ML. Thoracic epidural analgesia in coronary artery bypass graft surgery: seven years’ experience. J Cardiothorac Vasc Anesth 2003; 17: 154–9.
Chaney MA, Nikolov MP, Blakeman BP, Bakhos M. Intrathecal morphine for coronary artery bypass graft procedure and early extubation revisited. J Cardiothorac Vasc Anesth 1999; 13: 574–8.
Fitzpatrick GJ, Moriarty DC. Intrathecal morphine in the management of pain following cardiac surgery. A comparison with morphine i.v. Br J Anaesth 1988; 60: 639–44.
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Metaanalyses. Lancet 1999; 354: 1896–900.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996; 17: 1–12.
McEvoy GK. AHFS Drug Information, Bethesda, MD: American Society of Health-System Pharmacists; 2005.
Repchinsky C. Compendium of Pharmaceuticals and Specialties. The Canadian Drug Reference for Health Professionals. Ottawa: Canadian Pharmacists Association; Ottawa, Ontario, 2005.
Thomson L. Micromedex Healthcare Series, Greenwood Village, Colorado: Micromedex; 2004.
Strassels SA, Mcnicol E, Suleman R. Postoperative pain management: a practical review, part 1. Am J Health Syst Pharm 2005; 62: 1904–16.
Altman DG. Confidence intervals for the number needed to treat. BMJ 1998; 317: 1309–12.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple,graphical test. BMJ 1997; 315: 629–34.
Lin JC, Szwerc MF, Magovern JA. Non steroidal antiinflammatory drug-based pain control for minimally invasive direct coronary artery bypass surgery. Heart Surg Forum 1999; 2: 169–71.
Burke JP, Pestotnik SL, Classen DC, Lloyd JF. Evaluation of the financial impact of ketorolac tromethamine therapy in hospitalized patients. Clin Ther 1996; 18: 197–211.
McCrory CR, Diviney DD, Moriarty JM, Luke DA, Fitzgerald DJ. Spinal prostaglandin formation and pain perception following thoracotomy; a role for cyclooxy-genase-2. Anesthesiology 2001; 95: A797 (abstract).
Murphy DF, Medley C. Preoperative indomethacin for pain relief after thoracotomy: comparison with postoperative indomethacin. Br J Anaesth 1993; 70: 298–300.
Doyle E, Bowler GM. Pre-emptive effect of multimodal analgesia in thoracic surgery. Br J Anaesth 1998; 80: 147–51.
Mogensen T, Vegger P, Jonsson T, Matzke AE, Lund C, Kehlet H. Systemic piroxicam as an adjunct to combined epidural bupivacaine and morphine for postoperative pain relief--a double-blind study. Anesth Analg 1992; 74: 366–70.
McCrory C, Diviney D, Moriarty J, Luke D, Fitzgerald D. Comparison between repeat bolus intrathecal morphine and an epidurally delivered bupivacaine and fentanyl combination in the management of post-tho-racotomy pain with or without cyclooxygenase inhibition. J Cardiothorac Vasc Anesth 2002; 16: 607–11.
Immer FF, Immer-Bansi AS, Trachsel N, et al. Pain treatment with a COX-2 inhibitor after coronary artery bypass operation: a randomized trial. Ann Thorac Surg 2003; 75: 490–5.
Ott E, Nussmeier NA, Duke PC, et al. Multicenter Study of Perioperative Ischemia (McSPI) Research Group; Ischemia Research and Education Foundation (IREF) Investigators. Efficacy and safety of the cyclooxygenase 2 inhibitors parecoxib and valdecoxib in patients undergoing coronary artery bypass surgery. J Thorac Cardiovasc Surg 2003; 125: 1481–92.
Nussmeier NA, Whelton AA, Brown MT, et al. Complications of the COX-2 inhibitors parecoxib and valdecoxib after cardiac surgery. N Engl J Med 2005; 352: 1081–91.
Barilaro C, Rossi M, Martinelli L, Guarneri S, Cimino A, Schiavello R. [Control of postoperative pain in heart surgery. Comparison of analgesics]. Minerva Anestesiol 2001; 67: 171–9.
Bigler D, Moller J, Kamp-Jensen M, Berthelsen P, Hjortso NC, Kehlet H. Effect of piroxicam in addition to continuous thoracic epidural bupivacaine and morphine on postoperative pain and lung function after thoracotomy. Acta Anaesthesiol Scand 1992; 36: 647–50.
Carretta A, Zannini P, Chiesa G, Altese R, Melloni G, Grossi A. Efficacy of ketorolac tromethamine and extrapleural intercostal nerve block on post-thoracotomy pain. A prospective, randomized study. Int Surg 1996; 81: 224–8.
Fayaz KM, Abel R, Pugh S, Hall JE, Mecklenburgh JS. Opioid sparing and side effect profile of three different analgesic techniques for cardiac surgery. Eur J Anaesthesiol 2003; 20: A6 (abstract).
Gust R, Pecher S, Gust A, Hoffmann V, Bohrer H, Martin E. Effect of patient-controlled analgesia on pulmonary complications after coronary artery bypass grafting. Crit Care Med 1999; 27: 2218–23.
Hynninen MS, Cheng DC, Hossain I, et al. Non-steroi-dal anti-inflammatory drugs in treatment of postoperative pain after cardiac surgery. Can J Anesth 2000; 47: 1182–7.
Jones RM, Cashman JN, Foster JM, Wedley JR, Adams AP. Comparison of infusions of morphine and lysine acetyl salicylate for the relief of pain following thoracic surgery. Br J Anaesth 1985; 57: 259–63.
Kavanagh BP, Katz J, Sandler AN, et al. Multimodal analgesia before thoracic surgery does not reduce postoperative pain. Br J Anaesth 1994; 73: 184–9.
Keenan DJ, Cave K, Langdon L, Lea RE. Comparative trial of rectal indomethacin and cryoanalgesia for control of early postthoracotomy pain. Br Med J (Clin Res Ed) 1983; 287: 1335–7.
Kulik A, Ruel M, Bourke ME, et al. Postoperative naproxen after coronary artery bypass surgery: a double-blind randomized controlled trial. Eur J Cardiothorac Surg 2004; 26: 694–700.
Merry AF, Wardall GJ, Cameron RJ, Peskett MJ, Wild CJ. Prospective, controlled, double-blind study of i.v. tenoxicam for analgesia after thoracotomy. Br J Anaesth 1992; 69: 92–4.
Pavy T, Medley C, Murphy DF. Effect of indomethacin on pain relief after thoracotomy. Br J Anaesth 1990; 65: 624–7.
Perttunen K, Kalso E, Heinonen J, Salo J. IV diclofenac in post-thoracotomy pain. Br J Anaesth 1992; 68: 474–80.
Perttunen K, Nilsson E, Kalso E. I.v. diclofenac and ketorolac for pain after thoracoscopic surgery. Br J Anaesth 1999; 82: 221–7.
Power I, Bowler GM, Pugh GC, Chambers WA. Ketorolac as a component of balanced analgesia after thoracotomy. Br J Anaesth 1994; 72: 224–6.
Rapanos T, Murphy P, Szalai JP, Burlacoff L, LamMcCulloch J, Kay J. Rectal indomethacin reduces post operative pain and morphine use after cardiac surgery. Can J Anesth 1999; 46: 725–30.
Rhodes M, Conacher I, Morritt G, Hilton C. Nonsteroidal antiinflammatory drugs for postthoracotomy pain. A prospective controlled trial after lateral thoracotomy. J Thorac Cardiovasc Surg 1992; 103: 17–20.
Richardson J, Sabanathan S, Mearns AJ, Evans CS, Bembridge J, Fairbrass M. Efficacy of pre-emptive analgesia and continuous extrapleural intercostal nerve block on post-thoracotomy pain and pulmonary mechanics. J Cardiovasc Surg (Torino) 1994; 35: 219–28.
Singh H, Bossard RF, White PF, Yeatts RW. Effects of ketorolac versus bupivacaine coadministration during patient-controlled hydromorphone epidural analgesia after thoracotomy procedures. Anesth Analg 1997; 84: 564–9.
Stouten EM, Armbruster S, Houmes RJ, Prakash O, Erdmann W, Lachmann B. Comparison of ketorolac and morphine for postoperative pain after major surgery. Acta Anaesthesiol Scand 1992; 36: 716–21.
Beattie WS, Badner NH, Choi P. Epidural analgesia reduces postoperative myocardial infarction: a metaanalysis. Anesth Analg 2001; 93: 853–8.
Conacher ID. Post-thoracotomy analgesia. Anesthesiol Clin North America 2001; 19: 611–25.
Marret E, Flahault A, Samama CM, Bonnet F. Effects of postoperative, nonsteroidal, antiinflammatory drugs on bleeding risk after tonsillectomy: meta-analysis of randomized, controlled trials. Anesthesiology 2003; 98: 1497–502.
Moiniche S, Romsing J, Dahl JB, Tramer MR. Nonsteroidal antiinflammatory drugs and the risk of operative site bleeding after tonsillectomy: a quantitative systematic review. Anesth Analg 2003; 96: 68–77.
Solomon DH, Glynn RJ, Bohn R, Levin R, Avorn J. The hidden cost of nonselective nonsteroidal antiinflammatory drugs in older patients. J Rheumatol 2003; 30: 792–8.
Ofman JJ, MacLean CH, Straus WL, et al. A metaanalysis of severe upper gastrointestinal complications of nonsteroidal antiinflammatory drugs. J Rheumatol 2002; 29: 804–12.
Lee A, Cooper MC, Craig JC, Knight JF, Keneally JP. Effects of nonsteroidal anti-inflammatory drugs on postoperative renal function in adults with normal renal function. Cochrane Database Syst Rev 2004: CD002765.
Patrono C, Ciabattoni G, Patrignani P, et al. Clinical pharmacology of platelet cyclooxygenase inhibition. Circulation 1985; 72: 1177–84.
Patel TN, Goldberg KC. Use of aspirin and ibuprofen compared with aspirin alone and the risk of myocardial infarction. Arch Intern Med 2004; 164: 852–6.
Fornaro G, Rossi P, Mantica PG, et al. Indobufen in the prevention of thromboembolic complications in patients with heart disease. A randomized, placebocontrolled, double-blind study. Circulation 1993; 87: 162–4.
Brochier ML. Evaluation of flurbiprofen for prevention of reinfarction and reocclusion after successful thrombolysis or angioplasty in acute myocardial infarction. The Flurbiprofen French Trial. Eur Heart J 1993; 14: 951–7.
Sanchez-Fidalgo S, Martin-Lacave I, Illanes M, Motilva V. Angiogenesis, cell proliferation and apoptosis in gastric ulcer healing. Effect of a selective cox-2 inhibitor. Eur J Pharmacol 2004; 505: 187–94.
Cahill RA, Sheehan KM, Scanlon RW, Murray FE, Kay EW, Redmond HP. Effects of a selective cyclo-oxygenase 2 inhibitor on colonic anastomotic and skin woundintegrity. Br J Surg 2004; 91: 1613–8.
Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR. The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998; 23: 834–8.
Mamdani M, Juurlink DN, Lee DS, et al. Cyclo-oxy-genase-2 inhibitors versus non-selective non-steroidal anti-inflammatory drugs and congestive heart failure outcomes in elderly patients: a population-based cohort study. Lancet 2004; 363: 1751–6.
Wright JM. The double-edged sword of COX-2 selective NSAIDs. CMAJ 2002; 167: 1131–7.
Dieppe PA, Ebrahim S, Martin RM, Juni P. Lessons from the withdrawal of rofecoxib. BMJ 2004; 329: 867–8.
Jüni P, Nartey L, Reichenbach S, Sterchi R, Dieppe PA, Egger M. Risk of cardiovascular events and rofecoxib: cumulative meta-analysis. Lancet 2004; 364: 1–9.
Reuben SS, Connelly NR. Postoperative analgesic effects of celecoxib or rofecoxib after spinal fusion surgery. Anesth Analg 2000; 91: 1221–5.
Reuben SS, Bhopatkar S, Maciolek H, Joshi W, Sklar J. The preemptive analgesic effect of rofecoxib after ambulatory arthroscopic knee surgery. Anesth Analg 2002; 94: 55–9.
Camu F, Beecher T, Recker DP, Verburg KM. Valdecoxib, a COX-2-specific inhibitor, is an efficacious, opioid-sparing analgesic in patients undergoing hip arthroplasty. Am J Ther 2002; 9: 43–51.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976; 16: 31–41.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Bainbridge, D., Cheng, D.C., Martin, J.E. et al. NSAID-analgesia, pain control and morbidity in cardiothoracic surgery. Can J Anesth 53, 46–59 (2006). https://doi.org/10.1007/BF03021527
Issue Date:
DOI: https://doi.org/10.1007/BF03021527