
Abstract
Purpose: The objectives of this study were to determine: 1) if anesthesiologists had experienced a medication error and 2) to identify causal factors. The perceived value of a Canadian reporting agency for medication errors and improved standards for labels on drug ampoules was also investigated.
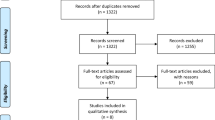
Methods: A self-reporting survey was mailed to members of the Canadian Anesthesiologists’ Society (n=2,266). Respondents provided free-text descriptions of medication errors and answered fixed response questions.
Results: Surveys from 687 anesthesiologists (30% response rate) revealed that 85% of the participants had experienced at least one drug error or “near miss”. Although most errors (1,038) were of minor consequence (98%), four deaths were reported. The commonest error involved the administration of muscle relaxants instead of a reversal agent. “Syringe swaps” (70.4%) and the misidentification of the label (46.8%) were common contributing factors. Anesthesiologists (97.9%) reported that they read the ampoule label “most of the time” although the label colour was an important secondary cue. Approximately half of the participants would report the error if a reporting program existed and 84% agreed that improved standards for drug labels would reduce the incidence of error.
Conclusions: Most anesthesiologist experienced at least one drug error. The commonest error was a “syringe swap” that involved a muscle relaxant. Most errors were of minor consequence, however, serious morbidity and mortality resulted from clearly preventable events. These results support the development of improved standards for drug labels and the establishment of a Canadian reporting program for medication errors.
Résumé
Objectif: 1) Découvrir si les anesthésiologistes ont vécu l’expérience d’une erreur de médication et 2) en déterminer les facteurs de causalité. Aussi, on a étudié la valeur perçue d’une agence de notification canadienne des erreurs de médication et de normes strictes des étiquettes d’ampules de médicaments.
Méthode: Une enquête d’autodéclaration a été postée aux membres de la Société canadienne des anesthésiologistes (n=2,266). Les répondants ont fourni des descriptions en textes libres des erreurs de médication et ont répondu aux questions à réponses fixes.
Résultats: Les réponses reçues de 687 anesthésiologistes (taux de réponse de 30 %) ont révélé que 85 % des participants avaient fait au moins une erreur de médicament ou l’avait évitée de justesse. Même si la plupart des erreurs (1,038) n’ont eu que des conséquences mineures (98 %), quatre décès ont été rapportés. L’erreur la plus fréquente concernait l’administration de myorelaxants à la place de décurarisants. “L’échange de seringue” (70,4 %) et la mauvaise identification de l’étiquette (46,8 %) étaient souvent des causes d’erreur. Certains (97,9 %) ont dit lire l’étiquette sur l’ampoule “la plupart du temps” nême si la couleur de l’étiquette était un important signal secondaire. La moitié des participants environ auraient mentionné l’erreur si un programme de notification avait existé et 84 % croyaient que des normes plus strictes d’étiquetage des médicaments pouvaient réduire l’incidence d’erreur.
Conclusion: La plupart des anesthésiologistes ont expérimenté au moins une erreur de médicament. L’erreur la plus fréquente a été “l’échange de seringue” pour un myorelaxant. Même si, en général, les conséquences sont mineures, une morbidité et une mortalité préoccupantes ont découlé d’incidents qu’on aurait pu certainement prévenir. Ces résultats incitent la mise au point de normes plus strictes pour l’étiquetage des médicaments et l’établissement d’un programme canadien de notification des erreurs de médication.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med 1991; 324: 377–84.
Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. JAMA 1995; 274: 29–34.
Schneider PJ, Gift MG, Lee Y-P, Rothermich EA, Sill BE. Cost of medication-related problems at a university hospital. Am J Health Syst Pharm 1995; 52: 2415–8.
Chopra V, Bovill JG, Spierdijk J, Koornneef F, Reported significant observations during anaesthesia: a prospective analysis over an 18-month period. Br J Anaesth 1992; 68: 13–7.
Short TG, O’Regan A, Lew J, Oh TE. Critical incident reporting in an anaesthetic department quality assurance programme. Anaesthesia 1992; 47: 3–7.
Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology 1984; 60: 34–42.
Currie M, Mackay P, Morgan C, et al. The “wrong drug” problem in anaesthesia: an analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 596–601.
Tessler MJ, White I, Naugler-Colville M, Biehl DR Inadvertent epidural administration of potassium chloride. A case report. Can J Anaesth 1988; 35: 631–3.
Symington MJ, Murthy BV, Milligan KR Epidural mexilitine (Letter). Anaesthesia 1993; 48: 925.
Ziser A, Sorenson EJ, Bluestein LS, Ronan KP. Epidural injection of aztreonam (Letter). Can J Anaesth 1994; 41: 553.
Groudine SB. Unexpected results: consider a medication error (Letter). Anesth Analg 1992; 75: 1073–4.
Orser BA, Oxorn DC An anaesthetic drug error: minimizing the risk. Can J Anaesth 1994; 41: 120–4.
Williamson JA, Webb RK, Sellen A, Runciman WB, Van der Walt JH. Human failure: an analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 678–83.
Albert M. Physician, Heal Thyself. Scientific America, May 2000: 32–3.
Merry AF, Peck DJ. Anaesthetists, errors in drug administration and the law. N Z Med J 1995; 108: 185–7.
Kohn LT, Corrigan JM, Donaldson MS. To Err is Human: Building a Safer Health System. Washington: National Academy Press, 1999.
Orser B. Reducing medication errors. CMAJ 2000; 162: 1150–1.
Chen R, Orser BA. Medication labels: for whose benefit? (Letter) Can J Anaesth 1996; 43: 194–5.
Cullen DJ, Sweitzer BJ, Bates DW, Burdick E, Edmondson A, Leape LL. Preventable adverse drug events in hospitalized patients: a comparative study of intensive care and general care units. Crit Care Med 1997; 25: 1289–97.
National Patient Safety Foundation. Diverse Groups Come Together to Improve Health Care Safety Through the National Patient Safety Foundation [Web page]. 1997 Available atwww.ama-assn.org/med-sci/npsf.
Orser BA Medication safety in anesthetic practice: first do no harm. Can J Anesth 2000; (In press).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Orser, B.A., Chen, R.J.B. & Yee, D.A. Medication errors in anesthetic practice: a survey of 687 practitioners. Can J Anaesth 48, 139–146 (2001). https://doi.org/10.1007/BF03019726
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03019726