
Abstract
Purpose
Upper respiratory infections (URI) presage perioperative respiratory complications, but thresholds to cancel surgery vary widely. We hypothesized that autonomically-mediated complications seen during emergence from anesthesia would be predicted by capnometry and reduced with preoperative bronchodilator administration.
Methods
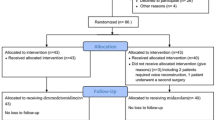
Afebrile outpatient tertiary-care children (age two months to 18 yr,n = 109) without lung disease or findings, having non-cavitary, non-airway surgery for under three hours, were randomized to bronchodilator premedication vs placebo and had preoperative capnometry. After halothane via mask, laryngeal mask airway, or endotracheal tube, and regional anesthesia as appropriate, patients recovered breathing room air while cough, wheeze, stridor, laryngospasm, and cumulative desaturations were recorded for 15 min.
Results
In this specific population, there was no association between adverse events and either URl within six weeks (n = 76) or URl within seven days (n = 21). Neither albuterol nor ipratropium premedication decreased adverse events. Endotracheal intubation was associated with increased emergence desaturations and placebo nebulized saline increased emergence coughing. Neither anesthesiologists nor preoperative capnometry predicted adverse events.
Conclusions
Adverse events were neither predicted nor prevented. In afebrile outpatient ASA l and ll children with no lung disease or findings, having non-cavitary, non-airway surgery for under three hours, there was no association between either recent URl or active URl and desaturation, wheeze, cough, stridor, or laryngospasm causing desaturation (allP > 0.05). In this highly selected population of afebrile patients, the results suggest that anesthesiologists may proceed with surgery using specific criteria in the presence of a URl.
Résumé
Objectif
Les infections des voies respiratoires supérieures (lRS) présagent des compiications respiratoires périopératoires, mais les valeurs seuils qui pourraient faire annuler l’opération chirurgicale varient beaucoup. Notre hypothèse était que ies complications d’origine autonome pendant le réveil postanesthésique, pourraient être prédites par ia capnométrie et réduites par l’administration préopéra-toire de bronchodilatateur.
Méthode
Des enfants afébriies admis à l’unité externe de soins tertiaires, (deux mois à 18 ans, n = 109), sans infection pulmonaire connue ou constatée, devant subir une opération de moins de trois heures ne touchant ni une cavité ni les voies aériennes, ont été répartis de façon aléatoire pour recevoir une prémédication bronchodilatatrice ou un placebo, et ont été soumis à une capnométrie préopératoire. Après l’administration d’halothane par masque, la mise en place d’un masque laryngé, ou d’un tube endotrachéal, et l’anesthésie régionale quand c’était indiqué, les patients ont respiré spontanément l’air ambiant. Toux, respiration siffiante, stridor, laryngospasme et désaturation cumulative ont été enregistrés pendant 15 min.
Résultats
Dans cette popuiation spécifique, aucun lien n’a été noté entre ies événements indésirabies et, soit une lRS dans les six dernières semaines (n = 76) ou les sept derniers jours (n = 21). La prémédication avec albutérol ou ipratropium n’a pas réduit les événements indésirables. L’intubation endotrachéaie a été associée à une désaturation accrue au réveil et la solution saline en aérosol a augmenté la
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Olsson GL. Bronchospasm during anaesthesia. A computer-aided incidence study of 136929 patients. Acta Anaesthesiol Scand 1987; 31: 244–52.
Cohen MM, Cameron CB. Should you cancel the operation when a child has an upper respiratory tract infection? Anesth Analg 1991; 72: 282–8.
Tait AR, Knight PR. Intraoperative respiratory complications in patients with upper respiratory tract infections. Can J Anaesth 1987; 34: 300–3.
McGill WA, Coveler LA, Epstein BS. Subacute upper respiratory infection in small children. Anesth Analg 1979; 58: 331–3.
DeSoto H, Patel RI, Soliman IE, Hannallah RS. Changes in oxygen saturation following general anesthesia in children with upper respiratory infection signs and symptoms undergoing otolaryngological procedures. Anesthesiology 1988; 68: 276–9.
Levy L, Pandit UA, Randel GI, Lewis IH, Tait AR. Upper respiratory tract infections and general anaesthesia in children. Peri-operative complications and oxygen saturation. Anaesthesia 1992; 47: 678–82.
Rolf N, Cote CJ. Frequency and severity of desaturation events during general anesthesia in children with and without upper respiratory infections. J Clin Anesth 1992; 4: 200–3.
Schreiner MS, O’Hara I, Markakis DA, Politis GD. Do children who experience laryngospasm have an increased risk of upper respiratory tract infection? Anesthesiology 1996; 85: 475–80.
Kinouchi K, Tanigami H, Tashiro C, Nishimura M, Fukumitsu K, Takauchi Y. Duration of apnea in anesthetized infants and children required for desaturation of hemoglobin to 95%. The influence of upper respiratory infection. Anesthesiology 1992;77: 1105–7.
Tait AR, Reynolds PI, Gutstein HB. Factors that influence an anesthesiologist’s decision to cancel elective surgery for the child with an upper respiratory tract infection. J Clin Anesth 1995; 7: 491–9.
Tait AR, Voepel-Lewis T, Munro HM, Gutstein HB, Reynolds PI. Cancellation of pédiatric outpatient surgery: economic and emotional implications for patients and their families. J Clin Anesth 1997; 9: 213–9.
Monto AS, Ullman BM. Acute respiratory illness in an American community. The Tecumseh study. JAMA 1974; 227: 164–9.
Empey DW, Laitinen LA, Jacobs L, Gold WM, Nadel JA. Mechanisms of bronchial hyperreactivity in normal subjects after upper respiratory tract infection. Am Rev Respir Dis 1976; 113: 131–9.
Picken JJ, Niewoehner DE, Chester EH. Prolonged effects of viral infections of the upper respiratory tract upon small airways. Am J Med 1972; 52: 738–46.
Kil HK, Rooke GA, Ryan-Dykes MA, Bishop MJ. Effect of prophylactic bronchodilator treatment on lung resistance after tracheal intubation. Anesthesiology 1994; 81:43–8.
Olsson GL, Hallen B. Laryngospasm during anaesthesia. A computer-aided incidence study in 136929 patients. Acta Anaesthesiol Scand 1984; 28: 567–75.
Yon B, Peslin R, Duvivier C, Vu VD, Grilliat JP. Expiratory capnography in asthma: evaluation of various shape indices. Eur Respir J 1994; 7: 318–23.
Teculescu D, Aubry C, Chau N, Locuty J, Pham QT, Manciaux M. Respiratory symptoms or signs on the day of the study alter pulmonary function in teenagers. Int J Epidemiol 1988; 17: 209–16.
Tait AR, Knight PR. The effects of general anesthesia on upper respiratory tract infections in children. Anesthesiology 1987; 67: 930–5.
Chan CS, Brown IG, Kelly CA, Dent AG, Zimmerman PV. Bronchodilator responses to nebulised ipratropium and salbutamol singly and in combination in chronic bronchitis. Br J Clin Pharmacol 1984; 17: 103–5.
Okanlami OA, Fryer AD, Hirshman C. Interaction of nondepolarizing muscle relaxants with M2 and M3 muscarinic receptors in guinea pig lung and heart. Anesthesiology 1996; 84: 155–61.
Hutton N, Wilson MH, Mellits ED, et al. Effectiveness of an antihistamine-decongestant combination for young children with the common cold: a randomized, controlled clinical trial. J Pediatr 1991; 118: 125–30.
Lewis RA, Lewis MN, Tattersfield AE. Asthma induced by suggestion: is it due to airway cooling? Am Rev Respir Dis 1984; 129: 691–5.
Schoeffel RE, Anderson SD, Altounyan RE. Bronchial hyperreactivity in response to inhalation of ultrasonically nebulised solutions of distilled water and saline. Br Med J (Clin Res Ed) 1981; 283: 1285–7.
van Noord JA, Smeets JJ, Maesen FP. A comparison of the onset of action of salbutamol and formoterol in reversing methacholine-induced bronchoconstriction. Respir Med 1998; 92: 1346–51.
Parnis SJ, Barker DS, Van Der Walt JH. Clinical predictors of anaesthetic complications in children with respiratory tract infections. Paediatr Anaesth 2001; 11: 29–40.
Tait AR, Malviya S, Voepel-Lewis T, Munro HM, Siewert M, Pandit UA. Risk factors for perioperative adverse respiratory events in children with upper respiratory tract infections. Anesthesiology 2001; 95: 299–306.
Tait AR, Pandit UA, Voepel-Lewis T, Munro HM, Malviya S. Use of the laryngeal mask airway in children with upper respiratory tract infections: a comparison with endotracheal intubation. Anesth Analg 1998; 86: 706–11.
Fryer AD, Jacoby DB. Parainfluenza virus infection damages inhibitory M2 muscarinic receptors on pulmonary parasympathetic nerves in the guinea-pig. Br J Pharmacol 1991; 102: 267–71.
Schuh S, Parkin P, Rajan A, et al. Highversus lowdose, frequently administered, nebulized albuterol in children with severe, acute asthma. Pediatrics 1989; 83:513–8.
Ream RS, Schreiner MS, Neff JD, et al. Volumetric capnography in children. Influence of growth on the alveolar plateau slope. Anesthesiology 1995; 82: 64–73.
Roy WL, Lerman J. Laryngospasm in paediatric anaesthesia. Can J Anaesth 1988; 35: 93–8.
Chripko D, Bevan JC, Archer DP, Bherer N. Decreases in arterial oxygen saturation in paediatric outpatients during transfer to the postanaesthetic recovery room. Can J Anaesth 1989; 36: 128–32.
Mizrahi T. Managing medical mistakes: ideology, insularity and accountability among internists-in-training. Soc Sci Med 1984; 19: 135–46.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was carried out at Johns Hopkins Hospital, Baltimore, MD and Children’s Hospital and Regional Medical Centre, Seattle, WA, USA.
Rights and permissions
About this article
Cite this article
Elwood, T., Morris, W., Martin, L.D. et al. Bronchodilator premedication does not decrease respiratory adverse events in pediatric general anesthesia. Can J Anaesth 50, 277–284 (2003). https://doi.org/10.1007/BF03017798
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017798