
Abstract
Purpose
Rotator cuff repair may result in severe postoperative pain. We compared a continuous intra-articular infusion to a continuous interscalene block with ropivacaine for patients undergoing outpatient rotator cuff repair.
Methods
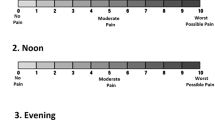
Seventeen patients were randomized to one of two groups: 1) interscalene block with 0.5% ropivacaine (40 mL) followed by a postoperative intra-articular infusion or; 2) interscalene block with 0.5% ropivacaine (40 mL) followed by a postoperative continuous interscalene infusion. Infusions were 0.2% ropivacaine at 10 mL·hr−1 for both groups. Infusions were maintained for 48 hr. Patients were discharged on the day of surgery. Verbal analogue pain scores (VAS) and postoperative oxycodone consumption were measured for 48 hr.
Results
Eight patients (47%; four in each group) had side effects or logistical problems complicating care. The mean VAS scores at rest and with movement in the postanesthesia care unit and at 12 hr, 24 hr, and 48 hr were not different (P > 0.1). Inadequate analgesia was reported in 50–75% of all study patients. Time until first oxycodone use was similar beiween groups 829 min ± 432 (interscalene) and 999 min ± 823 (intra-articular;P = 0.6). Total oxycodone consumption was also similar 49 mg ± 48 and 59 mg ± 51 (P = 0.7), respectively.
Conclusions
This study demonstrates the difficulties of ambulatory interscalene and intra-articular infusion for rotator cuff surgery. The high VAS scores and need for additional medical care suggest that intra-articular administration may not be reasonable for this magnitude of surgery. Further refinement of the perineural local anesthetic infusion is necessary to consistently provide analgesia after ambulatory rotator cuff surgery.
Résumé
Objectif
La réparation de la coiffe des rotateurs peut provoquer des douleurs postopératoires sévères. Nous avons comparé une perfusion intra-articulaire continue à un bloc interscalène continu avec de la ropivacaïne chez des patients devant subir la réparation de la coiffe des rotateurs en chirurgie ambulatoire.
Méthode
Dix-sept patients ont été répartis au hasard en deux groupes: 1) bloc interscalène avec de la ropivacaïne à 0,5 % (40 mL) suivi d’une perfusion intra-articulaire postopératoire ou 2) bloc interscalène avec de la ropivacaine à 0,5 % (40 mL) suivi d’une perfusion postopératoire interscalène continue. Les perfusions comportaient de la ropivacaine à 0,2 % administrée selon 10 mL · hr−1 dans les deux groupes. Elles ont été maintenues pendant 48 h. Les patients ont reçu leur congé le jour de l’intervention. Les scores verbaux de l’échelle visuelle analogique (EVA) et la consommation d’oxycodone postopératoire ont été notés pendant 48 h.
Résultats
Huit patients (47 %; quatre dans chaque groupe) ont été traités pour des effets secondaires ou des complications de problèmes logistiques. Les scores moyens à l’EVA enregistrés au repos et en mouvement n’ont pas été différents après l’anesthésie ou 12, 24 et 48 h plus tard (P > 0,1). Une analgésie incomplète a été rapportée chez 50–75 % de tous les patients de l’étude. Le temps écoulé avant la première demande d’oxycodone a été similaire dans les deux groupes: 829 min ± 432 (interscalène) et 999 min ± 823 (intra-articulaire; P = 0,6). La consommation totale d’oxycodone aussi a été semblable: 49 mg ± 48 et 59 mg±51 (P = 0,7).
Conclusion
L’étude démontre les difficultés d’une perfusion ambulatoire interscalène ou intraarticulaire en chirurgie de la coiffe des rotateurs. Les scores élevés de l’EVA et les besoins de soins supplémentaires supposent que l’administration intra-articulaire ne soit pas appropriée à l’importance de l’intervention chirurgicale. Il faut raffiner la perfusion périneurale d’anesthésique local afin de fournir une analgésie constante après l’opération ambulatoire de la coiffe des rotateurs.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Winnie AP. Interscalene brachial plexus block. Anesth Anaig 1970; 49: 455–66.
Klein SM, Grant SA, Greengrass RA, et al. Interscalene brachial plexus block with a continuous catheter insertion system and a disposable infusion pump. Anesth Analg 2000; 91: 1473–8.
Klein SM, Nielsen KC, Martin A, et al. Interscalene brachial plexus block with continuous intraarticular infusion of ropivacaine. Anesth Analg 2001; 93: 601–5.
Grant SA, Nielsen KC, Greengrass RA, Steele SM, Klein SM. Continuous peripheral nerve block for ambulatory surgery. Reg Anesth Pain Med 2001; 26: 209–14.
Tuominen M, Haasio J, Hekali R, Rosenberg PH. Continuous interscalene brachial plexus block: clinical efficacy, technical problems and bupivacaine plasma concentrations. Acta Anaesthesiol Scand 1989; 33: 84–8.
Singelyn FJ, Seguy S, Gouverneur JM. Interscalene brachial plexus analgesia after open shoulder surgery: continuous versus patient-controlled infusion. Anesth Analg 1999; 89: 1216–20.
Borgeat A, Tewes E, Biasca N, Gerber C. Patient-controlled interscalene analgesia with ropivacaine after major shoulder surgery: PCIA vs PCA. Br J Anaesth 1998; 81: 603–5.
Rawal N, Axelsson K, Hylander J, et al. Postoperative patient-controlled local anesthetic administration at home. Anesth Analg 1998; 86: 86–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Sponsorship: Departmental. Pumps were supplied by Sorrensen Medical, West Jordan, UT, USA.
Rights and permissions
About this article
Cite this article
Klein, S.M., Steele, S.M., Nielsen, K.C. et al. The difficulties of ambulatory interscalene and intra-articular infusions for rotator cuff surgery: a preliminary report. Can J Anaesth 50, 265–269 (2003). https://doi.org/10.1007/BF03017796
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017796