
Abstract
Purpose
The current bedside “gold standard” for cardiac output (CO) monitoring is thermodilution using a pulmonary artery catheter (PAC) but there is a number of risks associated with its use. The primary objective of this review was to evaluate the utility of esophageal Doppler (ED) as a minimally invasive monitor of CO.
Source
Medline literature search from 1966 to 2001 with citation review for studies comparing ED to PAC thermodilution for CO in perioperative and critically ill patients.
Principal findings
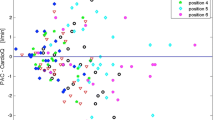
Twenty-five publications were identifed comparing ED and PAC measurement of CO in a broad range of patients. There was a good overall correlation between CO determined by ED and thermodilution (n = 18 studies, median R = 0.89, range 0.52 to 0.98) and minimal bias (n = 13, median −0.01, range 1.38 to 2 L·min−1). The precision of ED was only fair overall as assessed by limits of agreement. The ED technique was found to be responsive in detecting changes in thermodilution CO and was reliable demonstrating both low intra- and inter-observer variation. ED was reportedly easy to insert after minimal training and was safe, with no significant complications identified.
Conclusion
ED is a practical, reliable, and valid device for measuring CO in perioperative and critically ill patients. Further studies with larger numbers of patients are needed to determine if the limited precision observed is inherent to the technique, the diagnoses of patients studied, or the small sample sizes.
Résumé
Objectif
La thermodilution avec un cathéter artériel pulmonaire (CAP) représente la référence actuelle en monitorage de chevet du débit cardiaque (DC), mais elle comporte certains risques. L’objectif principal de la présente revue était d’évaluer l’utilité du Doppler œsophagien (DO) comme moniteur du DC à effraction minimale.
Source
Nous avons procédé à une recherche dans Medline, pour la période de 1966 à 2001, et à une revue des citations pour les études comparant l’usage périopératoire du DO et de la thermodilution avec CAP pour le DC chez des patients gravement malades.
Constatations principales
Vingt-cinq articles traitaient de la comparaison des mesures du DC avec DO et CAP chez une grande diversité de patients. Une bonne corrélation globale a été notée entre le DC déterminé par le DO et la thermodilution (n = 18 études, R médian = 0,89, étendue de 0,52 à 0,98) et biais minimal (n = 13, médiane −0,01, étendue de 1,38 à 2 L·min−1). La précision du DO n’a été que bonne dans l’ensemble comme l’ont montré les limites de la concordance. La technique du DO a été trouvée efficace, car elle détecte les modifications du DC noté par thermodilution, et fiable, puisqu’elle peut démontrer une faible variation intra-observateur et interobservateur. Les articles révèlent que le DO est facile à insérer, ne requérant qu’une formation minimale, et sans risque, ne présentant pas de complications significatives connues.
Conclusion
Le DO est un appareil de mesure périopératoire du DC pratique, fiable et valide pour des patients gravement malades. D’autres études auprès d’un plus grand nombre de patients demeurent nécessaires pour déterminer si la précision limitée qui a été observée est inhérente à la technique, aux diagnostics des patients étudiés ou aux échantillonnages de faible effectif.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Pulmonary Artery Catheter Consensus Conference Participants. Pulmonary artery catheter consensus conference: consensus statement. Crit Care Med 1997; 25: 910–24.
Swan HJC, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D. Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. N Engl J Med 1970; 283: 447–51.
Connors AF Jr, Speroff T, Dawson NV, et al. The effectiveness of right heart catheterization in the initial care of critically ill patients. JAMA 1996; 276: 889–97.
Zion MM, Balkin J, Rosenmann D, et al. Use of pulmonary artery catheters in patients with acute myocardial infarction. Analysis of experience in 5,841 patients in the SPRINT registry. Chest 1990; 98: 1331–5.
Sandham JD, Hull RD, Brant R, and the Canadian Critical Care Clinical Trials Group Rationale. A randomized controlled trial of pulmonary artery catheter use in 1994 high-risk geriatric surgical patients. Am J Respir Crit Care Med 2001; 163: A16 (abstract).
Singer M. Cardiac output in 1998. Heart 1998; 79: 425–8.
Newman DG, Callister R. The non-invasive assessment of stroke volume and cardiac output by impedance cardiography: a review. Aviat Space Environ Med 1999; 70: 780–9.
Troianos CA, Porembka DT. Assessment of left ventricular function and hemodynamics with transesophageal echocardiography. Crit Care Clin 1996; 12: 253–72.
Side C, Gosling R. Non-surgical assessment of cardiac function. Nature 1971; 232: 335–6.
Daigle RE, Miller CW, Histand MB, McLeod FD, Hokanson DE. Nontraumatic aortic blood flow sensing by use of using an ultrasonic esophageal probe. J Appl Physiol 1975; 38: 1153–60.
Huntsman LL, Stewart DK, Barnes SR, Franklin SB, Colocousis JS, Hessel EA. Noninvasive Doppler determination of cardiac output in man. Clinical validation. Circulation 1983; 67: 593–602.
Boulnois JG, Pechoux T. Non-invasive cardiac output monitoring by aortic blood flow measurement with the Dynemo 3000. J Clin Monit 2000; 16: 127–40.
Perrino AC Jr, Fleming J, LaMantia KR. Transesophageal Doppler cardiac output monitoring: performance during aortic reconstructive surgery. Anesth Analg 1991; 73: 705–10.
Penny JA, Anthony J, Shennan AH, de Swiet M, Singer M. A comparison of hemodynamic data derived by pulmonary artery flotation catheter and the esophageal Doppler monitor in preeclampsia. Am J Obstet Gynecol 2000; 183: 658–61.
Lavandier B, Muchada R, Cathignol D. The importance of measuring the diameter of the aorta in peroperative blood flow monitoring. V International Symposium on Biomedical Engineering 1994, Santiago: Spain, 1994: 258–9 (abstract).
Bernardin G, Tiger F, Fouché R, Mattéi M. Continuous noninvasive measurement of aortic blood flow in critically ill patients with a new esophageal echo-Doppler system. J Crit Care 1998; 13: 177–83.
Singer M. Esophageal Doppler monitoring of aortic blood flow: beat-by-beat cardiac output monitoring. Int Anesth Clin 1993: 99–125.
Histand MB, Wells MK, Reeves JT, Sodal IE, Adamson HP, Wilson JT. Ultrasonic pulsed Doppler transesophageal measurement of aortic haemodynamics in humans. Ultrasonics 1979; 17: 215–8.
Rodriguez RM, Berumen KA. Cardiac output measurement with an esophageal Doppler in critically ill emergency department patients. J Emerg Med 2000; 18: 159–64.
Klein G, Emmerich M, Maisch O, Dummler R. Clinical evaluation of non-invasive monitoring aortic blood flow (ABF) by a transesophageal echo-Doppler device. Anesthesiology 1998; 89: A446 (abstract).
Lefrant J-Y, Bruelle P, Aya AGM, et al. Training is required to improve the reliability of esophageal Doppler to measure cardiac output in critically ill patients. Intensive Care Med 1998; 24: 347–52.
Freund PR. Transesophageal Doppler scanning versus thermodilution during general anesthesia. An initial comparison of cardiac output techniques. Am J Surg 1987; 153: 490–4.
Stetz CW, Miller RG, Kelly GE, Raffin TA. Reliability of the thermodilution method in the determination of cardiac output in clinical practice. Am Rev Respir Dis 1982; 126: 1001–4.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986: 307–10.
Altman D. Practical Statistics for Medical Research. London, UK: Chapman & Hall, 1991.
Baillard C, Cohen Y, Fosse JP, Karoubi P, Hoang P, Cupa M. Haemodynamic measurements (continuous cardiac output and systemic vascular resistance) in critically ill patients: transesophageal Doppler versus continuous thermodilution. Anaesth Intensive Care 1999; 27: 33–7.
Cuschieri J, Rivers E, Caruso J, et al. A comparison of transesophageal Doppler, thermodilution and Fick cardiac output measurements in critically ill patients. Crit Care Med 1998; 26(suppl): A62 (abstract).
DiCorte CJ, Latham P, Greilich PE, Cooley MV, Grayburn PA, Jessen ME. Esophageal Doppler monitor determinations of cardiac output and preload during cardiac operations. Ann Thorac Surg 2000; 69: 1782–6.
Krishnamurthy B, McMurray TJ, McClean E. The perioperative use of the oesophageal Doppler monitor in patients undergoing coronary artery revascularization. Anaesthesia 1997; 52: 624–9.
Kumar A, Minagoe S, Thangathurai D, et al. Noninvasive measurement of cardiac output during surgery using a new continuous-wave Doppler esophageal probe. Am J Cardiol 1989; 64: 793–8.
Madan AK, UyBarreta VV, Aliabadi-Wahle S, et al. Esophageal Doppler ultrasound monitor versus pulmonary artery catheter in the hemodynamic management of critically ill surgical patients. J Trauma 1999; 46: 607–11.
Mark JB, Steinbrook RA, Gugino LD, et al. Continuous noninvasive monitoring of cardiac output with esophageal Doppler ultrasound during cardiac surgery. Anesth Analg 1986; 65: 1013–20.
Perrino AC Jr, Fleming J, LaMantia KR. Transesophageal Doppler ultrasonography: evidence for improved cardiac output monitoring. Anesth Analg 1990; 71: 651–7.
Schmid ER, Spahn DR, Tornic M. Reliability of a new generation transesophageal Doppler device for cardiac output monitoring. Anesth Analg 1993; 77: 971–9.
Siegel LC, Shafer SL, Martinez GM, Ream AK, Scott JC. Simultaneous measurements of cardiac output by thermodilution, esophageal Doppler, and electrical impedance in anesthetized patients. J Cardiothorac Anesth 1988; 2: 590–5.
Singer M, Clarke J, Bennett ED. Continuous hemodynamic monitoring by esophageal Doppler. Crit Care Med 1989; 17: 447–52.
Spahn DR, Schmid ER, Tornic M, et al. Noninvasive versus invasive assessment of cardiac output after cardiac surgery: clinical validation. J Cardiothorac Vasc Anesth 1990; 4: 46–59.
Stein MS, Barratt SMcG, Purcell GJ. Intraoperative assessment of the Lawrence 3000 Doppler cardiac output monitor. Anaesth Intensive Care 1991; 19: 251–5.
Valtier B, Cholley BP, Belot J-P, de la Coussaye J-E, Mateo J, Payen DM. Noninvasive monitoring of cardiac output in critically ill patients using transesophageal Doppler. Am J Respir Crit Care Med 1998; 158: 77–83.
Wagner G, Kalckhoff A, Emmerich M, Westhof FB, Klein G. Noninvasive monitoring cardiac output (CO) during off-pump coronary artery bypass grafting (OP-CABG). New York Post Graduate Assembly. New York: 1999: 115 (abstract).
Cariou A, Monchi M, Joly L-M, et al. Noninvasive cardiac output monitoring by aortic blood flow determination: evaluation of the Sometec Dynemo-3000 system. Crit Care Med 1998; 26: 2066–72.
Muchada R, Cathignol D, Lavandier B, Lamazou J, Haro D. Aortic blood flow measurement. Am J Noninvas Cardiol 1988; 2: 24–31.
Lavandier B, Cathignol D, Muchada R, Xuan BB, Motin J. Noninvasive aortic blood flow measurement using an intraesophageal probe. Ultrasound Med Biol 1985; 11:451–60.
Lefrant JY, Aya G, de la Coussaye JE, et al. Comparison of cardiac output measured by esophageal Doppler vs thermodilution. Intensive Care Med 1992; 18(suppl 2): S177 (abstract).
Raper R, Sibbald WJ. Misled by the wedge? The SwanGanz catheter and left ventricular preload. Chest 1986; 89: 427–34.
Calvin JE, Driedger AA, Sibbald WJ. Does the pulmonary capillary wedge pressure predict left ventricular preload in critically ill patients? Crit Care Med 1981; 9: 437–43.
Singer M, Bennett ED. Noninvasive optimization of left ventricular filling using esophageal Doppler. Crit Care Med 1991; 19: 1132–7.
Mythen MG, Webb AR. Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Arch Surg 1995; 130: 423–9.
Sinclair S, James S, Singer M. Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. BMJ 1997; 315: 909–12.
Author information
Authors and Affiliations
Corresponding author
Additional information
Dr. Laupland was supported by the 2000 Bayer Healthcare/Canadian Institutes of Health Research/Canadian Infectious Diseases Society Research Fellowship and a clinical fellowship award from the Alberta Heritage Foundation for Medical Research.
Rights and permissions
About this article
Cite this article
Laupland, K.B., Bands, C.J. Utility of esophageal Doppler as a minimally invasive hemodynamic monitor: a review. Can J Anesth 49, 393–401 (2002). https://doi.org/10.1007/BF03017329
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017329