
Abstract
Purpose
In a previous study we noticed that P6 acupressure ecreased postoperative nausea and vomiting (PONV) more markedly after discharge. As motion sickness susceptibility is increased by, for example, opioids we hypothesized that P6 acupressure decreased PONV by decreasing motion sickness susceptibility. We studied time to nausea by a laboratory motion challenge in a group of volunteers, during P6 and placebo acupressure.
Methods
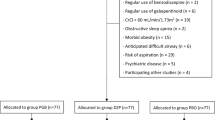
60 women with high and low susceptibilities for motion sickness participated in a randomized and double-blind study with an active P6 acupressure, placebo acupressure, and a control group (n = 20 in each group). The risk score for PONV was over 50%. The motion challenge was by eccentric rotation in a chair, blindfolded and with chin to chest movements of the head. The challenge was stopped when women reported moderate nausea. Symptoms were recorded.
Results
Mean time to moderate nausea was longer in the P6 acupressure group compared to the control group. P6 acupressure = 352 (259-445), mean (95% confidence interval) in seconds, control = 151 (121-181) and placebo acupressure = 280 (161-340); (P = 0.006). No difference was found between P6 and placebo acupressure or placebo acupressure and control groups. Previous severity of motion sickness did not influence time to nausea (P = 0.107). The cumulative number of symptoms differed between the three groups (P < 0.05). Fewer symptoms were reported in the P6 acupressure compared to the control group P < 0.009. Overall, P6 acupressure was only marginally more effective than placebo acupressure on the forearms.
Conclusion
In females with a history of motion sickness P6 acupressure increased tolerance to experimental nauseogenic stimuli, and reduced the total number of symptoms reported.
Résumé
Objectif
Nous avions expérimenté déjà que ľacupression en P6 diminuait davantage les nausées et les vomissements postopératoires (NVPO) après ľhospitalisation. Comme la susceptibilité au mal des transports est augmentée par les opioides, entre autres, nous avons pensé que ľacupression en P6 diminuerait les NVPO en réduisant la susceptibilité au mal des transports. Nous avons mesuré le temps écoulé avant les premières nausées lors de ďune épreuve de mouvement chez des volontaires pendant ľapplication ďacupression en P6 ou ďun placebo.
Méthode
Notre essai randomisé et à double insu a réuni 60 femmes, peu ou très sujettes au mal des transports, réparties en trois groupes: avec acupression active en P6, acupression placebo, ou groupe témoin (n = 20 dans chaque groupe). Ľévaluation des risques de NVPO était de plus de 50 %. Ľépreuve de mouvement consistait en une rotation excentrique dans une chaise, les yeux bandés, et en des mouvements de la tête vers la poitrine. Ľépreuve était arrêtée quand les femmes avaient des nausées modérées. Les symptômes étaient notés.
Résultats
Le temps moyen écoulé avant ľapparition de nausées modérées a été plus long dans le groupe avec acupression en P6 comparé au groupe témoin. Acupression en P6 = 352 (259-445), moyenne (intervalle de confiance de 95 %) en secondes, groupe témoin = 151 (121-181) et acupression placebo = 280 (161-340) ; (P = 0,006). Aucune différence n’a été trouvée entre les groupes ďacupression en P6 et placebo ou entre les groupes placebo et témoin. La sévérité du mal des transports préalable n’a pas eu ďinfluence sur le temps écoulé avant les nausées (P = 0,107). Ľensemble des symptômes diffère entre les trois groupes (P < 0,05). Moins de symptômes ont été rapportés chez les patientes soumises à ľacupression en P6 comparées aux témoins P < 0,009. Sur ľensemble, ľacupression en P6 n’a été que marginalement plus efficace que le placebo appliqué sur les avant-bras.
Conclusion
Chez des femmes qui présentent des antécédents de mal des transports, ľacupression en P6 augmente la tolérance aux stimuli nauséogènes expérimentaux et réduit en nombre la fréquence des symptômes.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Kamath B, Curran J, Hawkey C, et al. Anaesthesia, movement and emesis. Br J Anaesth 1990; 64: 728–30.
Apfel CC, Läärä E, Koivuranta M, Creim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting. Conclusions from cross-validations between two centers. Anesthesiology 1999; 91: 693–700.
Bertolucci LE, Didario B. Efficacy of a portable acustimulation device in controlling seasickness. Aviat Space Environ Med 1995; 66: 1155–8.
Alkaissi A, Stålnert M, Kalman S. Effect and placebo effect of acupressure (P6) on nausea and vomiting after outpatient gynaecological surgery. Acta Anaesthesiol Scand 1999; 43: 270–4.
Alkaissi A, Evertsson K, Johnsson VA, Ofenbartl L, Kalman S. P6 acupressure may relieve nausea and vomiting after gynecological surgery: an effectiveness study in 410 women. Can J Anesth 2002; 49: 1034–9.
Cowings PS, Toscano WB. Autogenic-feedback training exercise is superior to promethazine for control of motion sickness symptoms. J Clin Pharmacol 2000; 40: 1154–65.
Hoffer ME, Gottshall K, Kopke RD, et al. Vestibular testing abnormalities in individuals with motion sickness. Otol Neurotol 2003; 24: 633–6.
A Barefoot Doctor’s Manual (The American Translation of The Official Chines Paramedical Manual). Philadelphia: Running Press; 1990.
Johnson WH, Stubbs RA, Kelk GF, Franks WR. Stimulus required to produce motion sickness. 1. Preliminary report dealing with importance of head movements. J Aviat Med1951; 22: 3 65–74.
Bruce DG, Golding JF, Hockenhull N, Pethybridge RJ. Acupressure and motion sickness. Aviat Space Environ Med 1990; 61: 361–5.
Ödkvist L. Clinical and instrumental investigational otolith function. Adv Otorhinolaryngol 2001; 58: 68–76.
Warwick-Evans LA, Masters IJ, Redstone SB. A doubleblind placebo controlled evaluation of acupressure in the treatment of motion sickness. Aviat Space Environ Med 1991; 62: 776–8.
Tramèr MR, Moore RA, Reynolds DJ, McQuay HJ. A quantitative systematic review of ondansetron in treatment of established postoperative nausea and vomiting. BMJ 1997; 314: 1088–92.
Beijing College of Traditional Chinese Medicine,et al. Essentials of Chinese Acupuncture. Beijing: Beijing Foreign Language Press; 1980.
Clement-Jones V, McLoughlin L, Tomlin S, Besser GM, Rees LH, Wen HL. Increased ß-endorphin but not metenkephalin levels in human cerebrospinal fluid after acupuncture for recurrent pain. Lancet 1980; 2: 946–8.
Yang LG, Jawan B, Chen CN, Ho RT, Chang KA.Lee JH. Comparison of P6 acupoint injection with 50% glucose in water and intravenous droperidol for prevention of vomiting after gynecological laparoscopy. Acta Anaesthesiol Scand 1993; 37: 192–4.
NIH Consensus Conference. Acupuncture: NIH consensus development panel on acupuncture. JAMA 1998; 280: 1518–24.
Roberts AH, Kewman DG, Mercier L, Hovell M. The power of nonspecific effects in healing: implications for psychosocial and biological treatments. Clin Psych Review 1993; 13: 375–91.
Linde K, Vickers A, Hondras M, et al. Systematic reviews of complementary therapies — an annotated bibliography. Part 1: acupuncture. BMC Complementary and Alternative Mecicine 2001; 1: 3.
Ray CA, Hume KM. Neck afferents and muscle sympathetic activity in humans: implications for the vestibulosympathetic reflex. J Appl Physiol 1998; 84: 450–3.
Jokerst MD, Gatto M, Fazio R, Gianaros PJ, Stern RM, Koch KL. Effects of gender of subjects and experimenter on susceptibility to motion sickness. Aviat Space Environ Med 1999; 70: 962–5.
Cheung B, Hofer K. Lack of gender difference in motion sickness induced by vestibular Coriolis crosscoupling. J Vestib Res 2002-2003; 12: 191–200.
Parker DE,Paker KL. Adaptation to the simulated stimulus rearrangement of weightlessness In: Cramption GH (Ed.). Motion and Space Sickness. Boca Raton, FL: CRC Press; 1990: 247–61.
Wood CD. Antimotion sickness and antiemetic drugs. Drugs 1979; 17: 471–9.
Uijtdehaage SH, Stern RM, Koch KL. Effects of eating on vection-induced motion sickness, cardiac vagal tone, and gastric myoelectric activity. Psychophysiology 1992; 29: 193–201.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Alkaissi, A., Ledin, T., Odkvist, L.M. et al. P6 acupressure increases tolerance to nauseogenic motion stimulation in women at high risk for PONV. Can J Anesth 52, 703–709 (2005). https://doi.org/10.1007/BF03016557
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016557