
Abstract
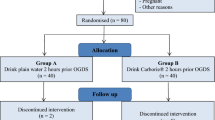
One hundred unpremedicated daycare patients were randomly assigned to one of four groups. Between two and three hours preoperatively all patients received either oral ranitidine 150 mg, or placebo, with bromosulphthalein (BSP) 50 mg in JO ml water, immediately followed by either ISO ml water or no further fluid.
The residual gastric volume (RGV) in the two placebo groups was significantly lower in patients given 150 ml water (20.6 ± 14.1 ml) than in those who continued fasting (29,9 ± 18.2 ml) (p <0.05). The RGV was further significantly decreased in the two ranitidine groups (10.0 ± 8.8, 9.7 ± 10.5ml) compared with the two placebo groups (20.6 ± 14.1, 29.9 ± 18.9 ml) (p <0.01).
Mean pH values were significantly higher in the two ranitidine groups (6.71 ± 0.99; 6.31 ± 1.81) than in the two placebo groups (2.05 ± 1.41; 1.72 ± 0.33) but were not significantly different in the fluid versus non-fluid groups. In patients who ingested 150 ml water there was no correlation between the premedication interval and either RGV or pH values. The extremely low percentage of the original BSP ( <0.9 per cent) in the gastric fluid of these patients demonstrated that gastric emptying of the ingested water was virtually complete prior to surgery.
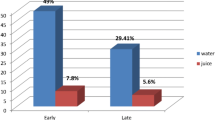
The combination of RGV of 25 ml or more with pH less than 2.5 was present in 56 per cent of patients who had only a sip of water with placebo, in 28 per cent of those who received 150 ml water with placebo, and in only two per cent of those patients who received ranitidine.
Résumé
Cent patients externes ont été randomisés en quatre groupes. Entre la première et la troisième heure pré-op, tous les patients ont reçu avec de la bromosulphthalein (BSP) (50 mg dans 10 ml ďeau) soit de la ranitidine 150 mg soit du placebo. Ceci fut suivi immédiatement soit par ľingestion de 150ml ďeau soit par aucune ingestion de liquide.
Le volume gastrique résiduel (RGV) dans les deux groupes placebo étaient significativement plus bas chez les patients ayant reçu 150ml ďeau (20.6 i 14.1ml) que ceux qui sont restés a jeun (29.9 ±18.2ml)(p < 0.05). Le RGV était encore plus significativement diminué dans les deux groupes ranitidine (10.0 ±8.8, 9.7 ± 10.5 ml) comparativement aux deux groupes placebo (20.6 ± 14.1, 29.9 í 8.9) (p < 0.01).
Les valeurs moyennes du pH étaient significativement plus élevées dans les groupes ranitidine (6.71 ± 0.99; 6.31 ± 1.81) que dans les deux groupes placebo mais n’étaient pas significativement différentes dans les deux groupes fluides versus groupe à jeun. Pour les patients ayant pris 150 ml ďeau il n’y avait aucune corrélation entre ľintervalle de la prémédication et soit la RGV ou les valeurs du pH. Le pourcentage extr êmement bas du BSP original (<0.9pour cent) dans le liquide gastrique de ces patients a démontré que la vidange gastrique de ľeau ingérée était presque complète avant la chirurgie.
La combinaison de RGV de 25 ml ou plus avec un pH inférieur à 2.5 était présente dans 56 pour cent des patients qui ont pris une simple gorgée ďeau avec le placebo, 20 pour cent chez ceux qui ont reçu 150 ml ďeau avec le placebo, et seulement deux pour cent chez ceux qui ont reçu la ranitidine.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Snow J On chloroform and other anaesthetics.London: Churchill, 1858:74-5.
Lister J On Anaesthetics, Part III. In: Holmes’ System of Surgery, Vol III, 3rd ed. London 1883. (Reprinted in: The Collected Papers of Joseph Lister. Birmingham: The Classics of Medicine Library, 1979: 171–2.)
Buxton W Anaesthetics: their uses and administration. London: Lewis, 1920: 24–5.
Boyle HEG, Hewer CL Practical anaesthetics. Third edition. London: Frowde, Hodder and Stoughton, 1923: 9.
Hunt JN Some properties of an elementary osmoreceptor mechanism. J. Physiol 1956; 132: 267–8.
Horowitz M, Pounder DJ Is the stomach a useful forensic clock? Aust NZ J Med 1985; 15: 273–6.
Moore JD, Christien PE, Coleman RE Gastric emptying of various meal weight and composition in man, Evaluation by dual liquid- and solid-phase method. Dig Dis Sci 1981; 26: 16–22.
Guidelines for the basic standards of practice of anaesthesia. The Canadian Anaesthetists’ Society Inc., Toronto, Ontario. 1981: p. 6.
Atkinson RS, Rushman GB, Lee JA A synopsis of anaesthesia. 9th ed. Bristol: Wright 1982: 96.
Gregory 1C Anaesthesia and the gasto-intestinal tract. In:Churchill-Davidson HC, ed. A Practice of Anaesthesia. 9th ed. Chicago: Year Book Medical Publishers, 1984: 939–53.
Orkin FK Selection. In:BV Wetchler, ed. Anesthesia for Ambulatory Surgery. Philadelphia: Lippincott, 1985: 106.
Prior FM A manual of anaesthesia for the small hospital. New Delhi: Emmanuel Hospital Association 1974: 58–9.
Sutherland T, Davies JM, Stock J The price and value of preoperative outpatient fasting -effects on gastric contents and outpatient morbidity. Can Anaesth Soc J 1985; 32: S100.
Ong BY, Palahniuk RJ, dimming M Gastric volume and pH in outpatients. Can Anaesth Soc J 1978; 25: 36–9.
Miller M, Wishart HY, Nimmo WS Gastric contents at induction of anaesthesia. Is a four hour fast necessary? Br J Anaesth 1983; 55: 1185–8.
Morison DH, Dunn GL, Fargas-Babjak AM, Moudgil CC, Smedstad K, Woo J A double-blind comparison of cimetidine and ranitidine as prophylaxis against gastric aspiration syndrome. Anesth Analg 1982; 61: 988–92.
Manchikanti L, Colliver JA, Marrero TC, Roush JR Assessment of age-related acid aspiration risk factors in pediatric, adult, and geriatric patients. Anesth Analg 1985; 64: 11–7.
Solanki DR, Suresh M, Ethridge HC The effects of intravenous cimetidine and metoclopramide on gastric volume pH. Anesth Analg 1984; 63: 599–602.
Guyton AC Textbook of Medical Physiology, 7th ed. Philadelphia: WB Saunders 1986: 774–8.
Durrant JM, Strunin L Comparative trial of the effect of ranitidine and cimetidine on gastric secretion in fasting patients at induction of anaesthesia. Can Anaesth Soc J 1982; 29: 446–50.
Hjortso E, Mondorf T Does oral premedication increase the risk of gastric aspiration? Acta Anaesthesiol Scand 1982; 26: 505–6.
Gregory RA Some factors influencing the passage of fluid through intestinal loops in dogs. J Physiol 1950; 111: 119–37.
Bloom DS, Jacobson ED, Grossman Ml Validation of dilution indicators in the stomach. Gastroenterology 1967; 52: 205–10.
Adelhoj B, Petring OU, Hagelsten JO Inaccuracy of peranesthetic gastric intubation for emptying liquid stomach contents. Acta Anaesthesiol Scand 1986; 30: 41–3.
Roberts RB, Shirley MA Reducing the risk of acid aspiration during cesarean section. Anesth Analg 1974; 58: 859–68.
Sutherland AD, Stock JG, Davies JM Effects of preoperative fasting on morbidity and gastric contents in patients undergoing day-stay surgery. Br J Anaesth 1986; 58: 876–8.
Wald A, Vanthiel DH, Hoechstetter L etal. Effect of pregnancy on gastrointestinal transit. Dig Dis Sci 1982; 27: 1015–8.
Cohen S The sluggish gallbladder of pregnancy. N Engl J Med 1980; 302: 397–8.
Fisher RS, Roberts GS, Grabowski CJ, Cohen S Inhibition of lower esophageal sphincter circular muscle by female sex hormones. Am J Physiol 1978; 234: E234–7.
Braverman DZ, Johnson ML, Kern F Effects of pregnancy and contraceptive steroids on gallbladder function. N Engl J Med 1980; 302: 362–4.
Maltby JR, Sutherland AD, Sale JP, Shaffer EA Preoperative oral fluids: is a five-hour fast justified prior to elective surgery? Anesth Analg 1986; 65: 112–6.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Sutherland, A.D., Maltby, J.R., Sale, J.P. et al. The effect of preoperative oral fluid and ranitidine on gastric fluid volume and pH. Can J Anesth 34, 117–121 (1987). https://doi.org/10.1007/BF03015327
Issue Date:
DOI: https://doi.org/10.1007/BF03015327