
Abstract
Purpose
To present a case of apparent interference of an ECG monitor by radiofrequency interference (RFI) and to provide a bnef review of RFI issues relevant to critical care medicine.
Clinical features
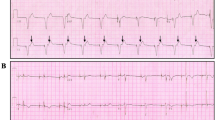
A 74-yr-old woman, with an implanted pacemaker, underwent major spinal surgery. In the post-anaesthesia care unit, the cardiac monitor demonstrated graphic evidence of pacemaker malfunction but there was no apparent effect on the patient. Investigation by the hospital’s biomedical personnel led to the conclusion that RFI was being interpreted by the monitor as abnormal pacemaker activity.
Conclusion
With the emergence of portable, battery-operated cominunication devices, there is an increased risk of RFI within hospitals. Antennas and repeaters are required to receive and boost the signal levels of these devices to improve signal quality. They are located throughout hospitals and may be situated near patient care areas. Patient monitors may receive these signals, misinterpret them as being patient-generated and output erroneous information. In the case described, the monitor was presented with RFI signals and interpreted them as pacemaker spikes, generating a tracing suggestive of pacemaker malfunction. Troubleshooting strategies and minimizing the potential impacts of RFI on patient monitors are discussed.
Résumé
Objectif
Présenter un cas d’interférence radiofréquentielle (IRF) apparue sur un moniteur ECG et passer brièvement en revue les problèmes de l’interférence radiofréquentielle en réanimation.
Éléments cliniques
Une femine de 74 ans porteuse d’un pacemaker implanté subissait une chirurgie rachidienne majeure. À l’unité des soins postanesthésiques, un enregistrement du moniteur cardiaque révélait un mauvais fonctionnement du pacemaker sans effet apparent sur la patiente. Un examen du personnel biomédical de l’hôpital permettait de conclure que l’IRF était interprétée comine une activité anormale du pacemaker.
Conclusion
L’apparition des instruments de cominunication portables alimentés par piles augmente le risque d’IRF à l’intérieur des hôpitaux. Dans le but d’améliorer la qualité des signaux, des antennes et des répéteurs sont utilisés pour recevoir et amplifier les signaux fournis par ces appareils. Ils sont localisés dans les hôpitaux et peuvent être situés près des secteurs de soins. Les moniteurs des patients peuvent capter ces signaux, les interpréter comine s’ils étaient générés par les patients et fournir ainsi de fausses informations. Dans le cas présent, le moniteur percevait des signaux d’IRF et les interprétait comine des pointes d’ECG, générant ainsi un tracé suggestif d’un dysfonctionnement de pacemaker. Les stratégies de détection et de correction destinées à minimiser les impacts potentiels de l’IRF sur les moniteurs font l’objet de la discussion.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
LaCava W, Pantiskas C, Morse W. Monitoring pacemaker patients. Journal of Clinical Engineering 1994; 19: 39–47.
Emergency Care Research Institute. Evaluation criteria, test methods, and results. ECRI Health Devices 1991; 20: 100–6.
Emergency Care Research Institute. Pacemaker pseudomalfunction. ECRI Health Devices 1988; 17: 356–7.
Mond HG, Sloman JG. The malfunctioning pacemaker system. Part I. PACE 1981; 4: 49–60.
Mond HG, Sloman JG. The malfunctioning pacemaker system. Part II. PACE 1981; 4: 168–81.
Bourke ME. The patient with a pacemaker or related device. Can J Anaesth 1996; 43: R24–32.
Levine PA, Balady GJ, Lazar HL, Beiott PH, Roberts AJ. Electrocautery and pacemakers: management of the paced patient subject to electrocautery. Ann Thorac Surg 1986; 41: 313–7.
Aldrete JA, Brown C, Daily J, Buerke V. Pacemaker malfunction due to microcurrent injection from a bioimpedance noninvasive cardiac output monitor. J Clin Monit 1995; 11: 131–3.
Emergency Care Research Institute. Guidance Article: Cellular telephones and radio transmitters — interference with clinical equipment. ECRI Health Devices 1993; 22: 416–20.
Naegeli B, Osswald S, Deola M, Burkart F. Intermittent pacemaker dysfunction caused by digital mobile telephones. J Am Coll Cardiol 1996; 27: 1471–7.
Imich W. Mobile telephones and pacemakers (Editorial). PACE 1996; 19: 1407–9.
Barbara V, Bartolini P, Donato A, Militello C. Electromagnetic interference of analog cellular telephones with pacemakers. PACE 1996; 19: 1410–8.
Hayes DL, Carrillo RG, Findlay GK, Embrey M. State of the science: pacemaker and defibrillator interference from wireless cominunication devices. PACE 1996; 19: 1419–30.
Imich W, Batz L, Müller R, Tobisch R. Electromagnetic interference of pacemakers by mobile phones. PACE 1996; 19: 1431–46.
Nowak B, Rosocha S, Zellerhoff C, et al. Is there a risk for interaction between mobile phones and single lead VDD pacemakers? PACE 1996; 19: 1447–50.
Sparks PB, Mond HG, Joyner KH, Wood MP. The safety of digital mobile cellular telephones with minute ventilation rate adaptive pacemakers. PACE 1996; 19: 1451–5.
Wilke A, Grimin W, Funck R, Maisch B. Influence of D-Net (European GSM-Standard) cellular phones on pacemaker function in 50 patients with permanent pacemakers. PACE 1996; 19: 1456–8.
Loscaizo J, Antman E. Artificial cardiac pacemakers: current concepts. J Crit Care 1986; 1: 174–88.
Andersen C, Madsen GM. Rate-responsive pacemakers and anaesthesia. Anaesthesia 1990; 45: 472–6.
Association for the Advancement of Medical Instrumentation. Cardiac monitors, heart rate meters, and alarms. AAMI EC13 1992; 1–44.
Gordon MS. Electromagnetic. The medical safety issue of the 1990s? Biomedical Technology Management 1995; July/August: 20–7.
Geddes LA. Technical Note: observations of intermittent electromagnetic interference on impedance respiration monitors. Journal of Clinical Engineering 1995; 20: 151–5.
Murdoch DK, Moran JF, Stafford M, King L, Loeb HS, Scanlon PJ. Pacemaker malfunction: fact or artifact? Heart and Lung 1986; 15: 150–4.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cleland, M.J., Crosby, E.T. Electrocardiographic “pacemaker pseudospikes” and radio frequency interference. Can J Anaesth 44, 751–756 (1997). https://doi.org/10.1007/BF03013391
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013391