
Abstract
Purpose
Respiratory acidosis during carbon dioxide (CO2) insufflation has been suggested as a cause of spontaneous abortion and preterm labour following laparoscopic cholecystectomy during pregnancy. Capnography may not be adequate as a guide to adjust pulmonary ventilation during laparoscopic surgery and hence arterial carbon dioxide (PaCO2) monitoring has been recommended. We report the feasibility and benefits of transcutaneous carbon dioxide monitoring (PtcCO2) as an approach to optimise ventilation during laparoscopic surgery in pregnancy.
Method
A healthy parturient received general anaesthesia for laparoscopic cholecystectomy. Pulmonary ventilation was adjusted to maintain end-tidal carbon dioxide (conventional PETCO2) at 32 mmHg during CO2 insufflation. A PtcCO2 monitor was used to trend PaCO2 throughout the procedure. Mechanical ventilation was interrupted every five minutes to obtain an end-tidal PCO2 value at large tidal volume (squeeze PETCO2).
Results
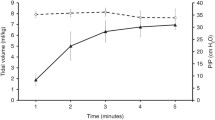
The PtcCO2 increased from 39 mmHg before induction to 45 mmHg after CO2 insufflation. This corresponds to an estimated maximum PaCO2 of 39–40 mmHg during insufflation. The PtcCO2 gradually returned to pre-induction baseline values one hour after the termination of CO3 insufflation. Squeeze PETCO2 values approximated PtcCO2 more closely than did conventional PETCO2 values (P < 0.01).
Conclusion
Continuous PtcCO2 measurements as well as squeeze PetCO2 may be of clinical value in trending and preventing hypercarbia during laparoscopic surgery.
Résumé
Objectif
L’acidose respiratoire durant l’insufflation au CO2 a été proposée comme cause d’avortement spontané et de travail prématuré à la suite de cholécystectomie laparoscopique durant la grossesse. La capnométrie peut ne pas être un guide adéquat pour ajuster la ventilation durant la chirurgie laparoscopique et de ce fait le monitoring du CO2 artériel a été recommandé. Cette étude rapporte la faisabilité et les bénéfices du monitorage du CO2 par voie transcutanée (PtcCO2) comme mesure d’optimalisation de la ventilation durant la chirurgie laparoscopique pendant la grossesse.
Méthode
Une parturiente en bonne santé a subi une cholécystectomie par laparoscopie sous anesthésie générale. La PCO2 en fin d’expiration (PETCO2 conventionnelle) a été maintenue à 32 mmHg durant l’insufflation de CO2 en ajustant la ventilation pulmonaire. Un moniteur de PCO2 transcutanée a été utilisé pour établir la tendance durant la procédure. A toutes les cinq minutes, la ventilation mécanique était interrompue pour mesurer la PCO2 de fin d’expiration suite à un volume courant élevé (“Squeeze” PETCO2).
Résultats
La PtcCO2 était de 39 mmHg avant l’induction et a augmenté à 45 mmHg après l’insufflation avec le CO2. Ceci correspond à une PaCO2 maximale estimée de 39–40 mmHg durant l’insufflation. La PtcCO2 a retrouvé progressivement les valeurs de base une heure après la fin de l’insufflation de CO2. La PETCO2 suite à un volume courant élevé a une meilleure corrélation avec la PtcCO2 que la PETCO2 normale (P < 0,01 ).
Conclusion
Les mesures de la PtcCO2 de même que celles de la PETCO2 suite à un volume courant élevé peuvent être cliniquement utiles durant la chirurgie laparoscopique pour établir la tendance et prévenir l’hypercarbie.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Lanza-fame RJ. Laparoscopic cholecystectomy during pregnancy. Surgery 1995; 118: 627–33.
Elerding SC. Laparoscopic cholecystectomy in pregnancy. Am J Surg 1993; 165: 625–7.
Steinbrook RA, Brooks DC, Datta S. Laparoscopic cholecystectomy during pregnancy. Review of anesthetic management, surgical considerations. Surg Endosc 1996; 10: 511–5.
Soper NJ, Hunter JG, Petrie RH. Laparoscopic cholecystectomy during pregnancy. Surg Endosc 1992; 6: 115–7.
Eichenberg BJ, Vanderlinden J, Miguel C, et al. Laparoscopic cholecystectomy in the third trimester of pregnancy. Am Surg 1996; 62: 874–7.
Curet MJ, Allen D, Josloff RK, et al. Laparoscopy during pregnancy. Arch Surg 1996; 131: 546–51.
Amos JD, Schorr SJ, Norman PF, et al. Laparoscopic surgery during pregnancy. Am J Surg 1996; 171: 435–7.
Reedy M, Galan H, Richards W, Kuehl T. Laparoscopy during pregnancy: a survey of the Society of Laparoendoscopic Surgeons. Am J Obstet Gynecol 1995; 172: A89.
Cruz AM, Southerland LC, Duke T, Townsend HGG, Ferguson JG, Crone L-AL. Intraabdominal carbon dioxide insufflation in the pregnant ewe. Uterine blood flow, intraamniotic pressure, and cardiopulmonary effects. Anesthesiology 1996; 85: 1395–102.
Hunter JG, Swanstrom L, Thornburg K. Carbon dioxide pneumoperitoneum induces fetal acidosis in a pregnant ewe model. Surg Endosc 1995; 9: 272–9.
Pucci RO, Seed RW. Case report of laparoscopic cholecystectomy in the third trimester of pregnancy. Am J Obstet Gynecol 1991; 165: 401–2.
Bhavani-Shankar K, Moseley H, Kumar AT, Delph Y. Capnometry and anaesthesia. Can J Anacsth 1992; 39: 617–32.
Severinghaus JW. Transcutaneous blood gas analysis. Respiratory Care 1983; 27: 152–9.
TCO2M® Transcutaneous CO2/O2 monitor. User’s Manual, model 860. Novametrix Medical Systems Inc. 1996: 18–9.
Hazinski TA, Severinghaus JW. Transcutancous analysis of arterial PCO2. Med Instrum 1982; 16: 150–3.
Eletr S, Jimison H, Ream AK, Dolan WM, Rosenthal MH. Cutaneous monitoring of systemic PCO2 on patients in the respiratory intensive care unit being weaned from the ventilator. Acta Anaesth Scand 1978; 68(Suppl): 123–7.
Epstein MF, Cohen AR, Feldman HA, Raemer DB. Estimation of PaCO2 by two noninvasive methods in the critically ill newborn infant. J Pediatr 1985; 106: 282–6.
Nunn JF. Carbon dioxide.In: Nunn JF (Ed.). Nunn’s Applied Respiratory Physiology, 4th ed. Cambridge: Butterworth-Heinemann Ltd., 1993: 245–6.
Reid CW, Martineau RJ, Miller DR, Hull KA, Baines J, Sullivan PJ. A comparison of transcutaneous, end-tidal and arterial measurements of carbon dioxide during general anaesthesia. Can J Anaesth 1992; 39: 31–6.
Drummond KJ, Fearnside MR, Chee A. Transcutaneous carbon dioxide measurement after craniotomy in spontaneously breathing patients. Neurosurgery 1997; 41: 361–7.
McEvedy BAB, McLeod ME, Mulera M, Kirpalani H, Lerman J. End-tidal, transcutaneous, and arterial PCO2 measurements in critically ill neonates: a comparative study. Anesthesiology 1988; 69: 112–6.
Bhavani Shankar K, Moseky H, Kumar T, Vemula V, Krishnan A. Arterial to end-tidal carbon dioxide tension difference during anaesthesia for tubal ligation. Anaesthesia 1987; 42: 482–6.
Shankar KB, Moseley H, Kumar Y, Vemula V. Arterial to end tidal carbon dioxide tension difference during Caesarean section anaesthesia. Anaesthesia 1986; 41: 698–702.
Fletcher R, Jonsim B, Cumming G, Brew J. The concept of deadspace with special reference to the single breath test for carbon dioxide. Br J Anaesth 1981; 53: 77–88.
Bhavani Shankar K, Kumar AY, Moseley, HSL, Ahyu-Hallsworth R. Terminology and current limitations of time capnography: A brief review. J Clin Monit 1995; 11: 175–82.
Newman W, Braid D, Wood C. Fetal acid-base status. 1. Relationship between maternal and fetal PCO2. Am J Obstet Gynecol 1967; 97: 43–51.
Harned HS Jr, Rowshan G, MacKinney LG, Sugioka K. Relationships of PO2, PCO2, and pH to onset of breadiing of the term lamb as studied by a flow-through cuvette electrode assembly. Pediatrics 1964; 33: 672–81.
Ivankovic AD, Elam JO, Huffman J. Effect of maternal hypercarbia on the newborn infant. Am J Obstet Gynccol 1970; 107: 939–45.
Walker AM, Oakes GK, Ehnnkranz R, Mchaughlin M, Chez RA. Effects of hypercarbia on uterine and umbilical circulations in conscious pregnant sheep. J Appl Physiol 1976; 41: 727–33.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bhavani-Shankar, K., Steinbrook, R.A., Mushlin, P.S. et al. Transcutaneous PCO2 monitoring during laparoscopic cholecystectomy in pregnancy. Can J Anaesth 45, 164–169 (1998). https://doi.org/10.1007/BF03013257
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013257