
Abstract
Purpose
Accurate haemodynamic assessment during surgical repair of scoliosis is crucial to the care of the patient. The purpose of this study was to compare transoesophageal echocardiography (TEE) with central venous pressure monitoring in patients with spinal deformities requiring surgery in the prone position.
Methods
Twelve paediatric patients undergoing corrective spinal surgery for scoliosis/kyphosis in the prone position were studied. Monitoring included TEE, intra-arterial and central venous pressure monitoring (CVP). Haemodynamic assessment was performed prior to and immediately after positioning the patient prone on the Relton-Hall table. Data consisted of mean arterial blood pressure (mBP), heart rate (HR), CVP, left ventricular end-systolic and end-diastolic diameters (LVESD and LVEDD respectively) and fractional shortening (FS). Right ventricular (RV) function and tricuspid regurgitation (TR) were assessed qualitatively. Analysis was performed using descriptive statistics, Student’s t test, sign rank, and correlation analysis.
Results
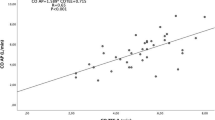
There was an increase in CVP (8.7 mmHg to 17.7 mmHg;P <.01), and decreases in LVEDD (37.1 mm to 33.2 mm;P <.05), and mean blood pressure (75.0 mmHg to 65.7 mmHg;P <.05) when patients were placed in the prone position. Fractional shortening, LVESD, and HR did not change from the supine to the prone position. Right ventricular systolic function and tricuspid regurgitation were unchanged.
Conclusion
These data indicate that the CVP is a misleading monitor of cardiac volume in patients with kyphosis/scoliosis in the prone position. This is consistent with previous studies. In this clinical situation, TEE may be a more useful monitoring tool to assess on-line ventricular size and function.
Résumé
Objectif
L’évaluation hémodynamique précise pendant la correction chirurgicale d’une scoliose est déterminante pour les soins donnés au patient. Le but de l’étude actuelle était de comparer l’échographie transoesophagienne (ETO) au monitorage de la pression veineuse centrale chez les patients souffrant de déformations rachidiennes nécessitant une chirurgie en décubitus ventral.
Méthodes
Douze patients pédiatriques devant subir, en décubitus ventral, une chirurgie de correction pour une scoliose ou une cyphose ont été étudiés. Le monitorage comprenait l’ETO, la mesure de la pression intra-artérielle et de la pression veineuse centrale (PVC). Lévaluation hémodynamique a été faite avant et immédiatement après l’installation du patient en décubitus ventral sur la table Relton-Hall. Les données comportaient la tension artérielle moyenne (TAm), la fréquence cardiaque (FC), la PVC, les diamètres ventriculaires gauches télosystolique et télodiastolique (DVGTS et DVGTD respectivement) et le raccourcissement fractionnaire (RF). La fonction du ventricule droit (VD) et la régurgitation tricuspidienne (RT) ont été évaluées qualitativement. L’analyse a été réalisée à partir de statistiques descriptives, du test t de Student, du test de rang et de l’analyse de corrélation.
Résultats
Il y a eu un accroissement de la PVC (de 8,7 mmHg à 17,7 mmHg;P <,0l), et une diminution du DVGTD (de 37,1 mm à 33,2 mm;P < 0,05) et de la tension artérielle moyenne (de 75,0 mmHg à 65,7 mmHg;P < 0,05) quand les patients ont été placés en décubitus ventral. Le raccourcissement fractionnaire, le DVGTS et la FC n’ont pas été modifiés lors du changement de position, de la position couchée au décubitus ventral. La fonction systolique du ventricule droit et la régurgitation tricuspidienne n’ont pas changé.
Conclusion
Ces résultats indiquent que la PVC n’est pas un moniteur fiable du volume cardiaque chez les patient souffrant de cyphose ou de scoliose, placés en décubitus ventral. Cela correspond aux études antérieures. Dans cette situation clinique, l’ETO peut être un outil de surveillance plus utile pour une évaluation en ligne de la taille et de la fonction ventriculaires.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Salem MR, Klowden AJ. Anesthesia for orthopaedic surgery.In: Gregory GA (Ed.). Pediatric Anesthesia, 3rd ed. New York: Churchill Livingstone Inc., 1994: 607–56.
Dykes MHM, Fuller JE, Goldstein LA. Sudden cessation of cardiac output during spinal fusion. Anesth Analg 1970; 49: 596–9.
Bagshaw ONT, Jardine A. Cardiopulmonary complications during anaesthesia and surgery for severe thoracic lordoscoliosis. Anaesthesia 1995; 50: 890–2.
Rhine EJ, Ménard EA. Anesthesia considerations for spinal instrumentation in pédiatric patient.In: Lui ACP, Crosby ET (Eds.). Problems in Anesthesia. Anesthesia and Musculoskeletal Disorders, Vol 5. Philadelphia: JB Lippincott Company, 1991: 67–79.
Harpole DH, Clements FM, Quill T, Wolfe WG, Jones RH, McCann RL. Right and left ventricular performance during and after abdominal aortic aneurysm repair. Ann Surg 1989; 209: 356–62.
Hansen RM, Viquerat CE, Matthay MA, et al. Poor correlation between pulmonary arterial wedge pressure and left ventricular end-diastolic volume after coronary artery bypass graft surgery. Anesthesiology 1986; 64: 764–70.
Kalman PG, Wellwood MR, Weisel RD, et al. Cardiac dysfunction during abdominal aortic operation: the limitations of pulmonary wedge pressures. J Vasc Surg 1986; 3: 773–81.
Douglas PS, Edmunds LH, St. John Sutton M, Geer R, Harken AH, Reichek N. Unreliability of hemodynamic indexes of left ventricular size during cardiac surgery. Ann Thorac Surg 1987; 44: 31–4.
Thys DM, Hillel Z, Goldman ME, Mindich BP, Kaplan JA. A comparison of hemodynamic indices derived by invasive monitoring and two-dimensional echocardiography. Anesthesiology 1987; 67; 630–4.
Roizen MF, Beaupre PN, Alpert RA et al. Monitoring with two-dimensional transesophageal echocardiography. Comparison of myocardial function in patients undergoing supraceliac, suprarenal-infraceliac, or infrarenal aortic occlusion. J Vasc Surg 1984; 1: 300–5.
Relton JES, Hall JE. An operation frame for spinal fusion. A new apparatus designed to reduce haemorrhage during operation. J Bone Joint Surg Br 1967; 49: 327–32.
Mason SJ, Fortuin NJ. The use of echocardiography for quantitative evaluation of left ventricular function. Prog Cardiovasc Dis 1978; 21: 119–32.
Nolan K. Anesthesia concerns for scoliosis surgery.In: Lui ACP, Crosby ET (Eds.). Problems in Anesthesia. Anesthesia and Musculoskeletal Disorders, Vol 5. Philadelphia: JB Lippincott Company, 1991: 52–65.
Shneerson JM, Sutton GC, Zorab PA. Causes of death, right ventricular hypertrophy, and congenital heart disease in scoliosis. Clin Orthop 1978; 35: 52–7.
Kafer ER. Respiratory and cardiovascular functions in scoliosis and the principles of anesthetic management. Anesthesiology 1980; 52; 339–45.
Primiano FP Jr, Nussbaum E, Hirschfeld SS, et al. Early echocardiographic and pulmonary function findings in idiopathic scoliosis. J Ped Orthop 1983; 3: 475–81.
Relton JES, Conn AW. Anaesthesia for the surgical correction of scoliosis by the Harrington method in children. Can Anaesth Soc J 1963; 10: 608–15.
Wadsworth R, Anderton JM, Vohra A. The effect of four different surgical prone positions on cardiovascular parameters in healthy volunteers. Anaesthesia 1996; 51: 819–22.
Yokoyama M, Ueda W, Hirakawa M, Yamamoto H. Hemodynamic effect of the prone position during anesthesia. Acta Anaesthesiol Scand 1991; 35: 741–4.
Lange RA, Katz J, McBride W, Moore DM Jr, Hillis LD. Effects of supine and lateral positions on cardiac output and intracardiac pressures. Am J Cardiol 1988; 62: 330–3.
Reich DL, Konstadt SN, Nejat M, Abrams HP, Bucek J. Intraoperative transeophageal echocardiography for the detection of cardiac preload changes induced by transfusion and phlebotomy in pediatric patients. Anesthesiology 1993; 79: 10–5.
Cheung AT, Savino JS, Weiss SJ, Aukburg SJ, Berlin JA. Echocardiographic and hemodynamic indexes of left ventricular preload in patients with normal and abnormal ventricular function. Anesthesiology 1994; 81: 376–87.
Swenson JD, Harkin C, Pace NL, Astle K, Bailey P. Transesophageal echocardiography: an objective tool in defining maximum ventricular response to intravenous fluid therapy. Anesth Analg 1996; 83: 1149–53.
Pagel PS, Grossman W, Haering JM, Warltier DC. Left ventricular diastolic function in the normal and diseased heart. Perspectives for the anesthesiologist (first of two parts). Anesthesiology 1993; 79: 836–54.
Mueller X, Stauffer JC, Jaussi A, Goy JJ, Kappenberger L. Subjective visual echocardiographic estimate of left ventricular ejection fraction as an alternative to conventional echocardiographic methods: comparison with contrast angiography. Clin Cardiol 1991; 14: 898–907.
Rajacich N, Burchard KW, Hasan FM, Singh AK. Central venous pressure and pulmonary capillary wedge pressure as estimates of left atrial pressure: effects of positive end-expiratory pressure and catheter tip malposition. Crit Care Med 1989; 17: 7–11.
Nunn JF. The pulmonary circulation.In: Nunn JF (Ed.). Applied Respiratory Physiology, 3rd ed. London: Butterworths, 1987: 117–39.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Soliman, D.E., Maslow, A.D., Bokesch, P.M. et al. Transoesophageal echocardiography during scoliosis repair: comparison with CVP monitoring. Can J Anaesth 45, 925–932 (1998). https://doi.org/10.1007/BF03012298
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012298