
Abstract
Purpose
To describe the perioperative assessment and anaesthetic management for surgical separation of three sets of conjoined twins with complex cardiac anomalies threatened with arterial desaturation and haemodynamic instability.
Clinical features
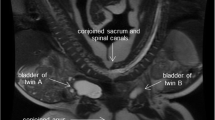
Three sets of conjoined twins, one omphaloischiopagus, one omphalopagus, and one thoraco-omphalopagus, were considered for separation during the perinatal or infantile period. Preoperative functional evaluation including continuous pulse oximetry, capnography, and cardiac electrophysiological studies were considered to be as important as anatomical evaluation of the cardiac anomalies and cross-circulation by angiography in assessing the feasibility of surgical separation. Ipsilateral infusion of prostaglandin E1 and phenylephrine were applied to the cyanotic and healthy twins respectively, to restore arterial oxygenation intraoperatively and to avoid profound hypoxaemia.
Conclusion
Surgical separation and anaesthesia should be well planned and rehearsed before clinical deterioration of the weaker twin. Aggressive pharmacological intervention and understanding of the cross-circulation pathophysiology is necessary to manage critical situations during surgical separation and in the postoperative period.
Résumé
Objectif
Décrire l’évaluation périopératoire et la gestion anesthésique de la séparation chirurgicale de trois couples de jumeaux siamois porteurs d’anomalies cardiaques complexes susceptibles de désaturation artérielle et d’instabilité hémodynamique.
Éléments cliniques
Trois couples de jumeaux siamois, dont un omphaloischiopage, un omphalopage et un thoraco-omphalopage étaient programmés pour une séparation pendant la période périnatale ou infantile. L’évaluation fonctionnelle préopératoire dont l’oxygmétrie de pouls continue, la capnographie, et les épreuves électrophysiologiques cardiaques étaient considérées comme aussi importantes que l’évaluation anatomique des anomalies cardiaques et l’étude de la circulation croisée par angiographie pour décider de la faisabilité d’une séparation chirurgicale. Une perfusion homolatérale de protaglandine E1 et de phényléphrine ont été administrées respectivement au jumeau cyanotique et au jumeau sain pour restaurer l’oxygénation artérielle pendant l’intervention et pour éviter l’hypoxémie profonde.
Conclusion
La séparation chirurgicale et l’anesthésie doivent être bien planifiées et répétées avant la détérioration du jumeau faible. Une intervention pharmacologique agressive et une connaissance de la physiopathologie de la circulation croisée sont essentielles pour la gestion des situations critiques pendant l’intervention pour séparation ainsi qu’à la période postopératoire.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Hoyle RM. Surgical separation of conjoined twins. Surg Gynecol Obstet 1990; 170: 549–62.
Chao C-C, Susetio L, Luu K-W, Kwan W-F. Anaesthetic management for successful separation of tripus ischiopagal conjoined male twins. Can J Anaesth 1980; 27: 565–70.
Harper RG, Kenigsberg K, Sia CG, Horn D, Stern D, Bongiovi V. Xiphopagus conjoined twins: a 300-year review of the obstetric, morphopathologic, neonatal, and surgical parameters. Am J Obstet Gynecol 1980; 137: 617–29.
Diaz JH, Furman EB. Perioperative management of conjoined twins. Anesthesiology 1987; 67: 965–73.
Aird I. The conjoined twins of Kano. BMJ 1954; 1: 831–7.
Rejjal A-LR, Nazer HM, Abu-Osba YK, Rifai A, Ahmed S. Conjoined twins: medical, surgical, and ethical challenges. Aust NZ J Surg 1992; 62: 287–91.
Block EC, Karis JH. Cardiopagus in neonatal thoracopagus twins: anesthetic management. Anesth Analg 1980; 59: 304–7.
Antonelli D, Shmilovitz L, Dharan M. Conjoined hearts. British Heart Journal 1986; 56: 486–8.
Wong KC, OhmuraA, Roberts TH, Webster LR, Cook GL. Anesthetic management for separation of craniopagus twins. Anesth Analg 1980; 59: 883–6.
Nichols BL, Blattner RJ, Rudolph AJ. General clinical management of thoracopagus twins. Birth Defects 1967; 3: 38–51.
Marin-Padilla M, Chin AJ, Marin-Padilla TM. Cardiovascular abnormalities in thoracopagus twins. Teratology 1981; 23: 101–13.
Patel R, Fox K, Dawson J, Taylor JFN, Graham GR. Cardiovascular anomalies in thoracopagus twins and the importance of preoperative cardiac evaluation. British Heart Journal 1977; 39: 1254–8.
O’Neill JA Jr,Holcomb GW III,Schnauffer L, et al. Surgical experience with thirteen conjoined twins. Ann Surg 1988; 208: 299–312.
Campbell GD, Brown SW, Anderson M, Anderson PG. Separation of conjoined twins. Aust NZ J Surg 1990; 60: 59–61.
Neutze JM, Starling MB, Elliott RB, Barratt-Boyes BG. Palliation of cyanotic congenital heart disease in infancy with E-type prostaglandins. Circulation 1977; 55: 238–41.
Pitlick P, French JW, Maze A, Kimble KJ, Ariagno RL, Reitz BA. Long-term low-dose prostaglandin E1 administration. J Pediatr 1980; 96: 318–20.
Coceani F, Olley PM, Lock JE. Prostaglandins, ductus arteriosus, pulmonary circulation: current concepts and clinical potential. Eur J Clin Pharmacol 1981; 18: 75–81.
Chen T-L, Lee Y-T, Wang M-J, Lee J-M, Lee Y-C, Chu S-H. Endothelin-1 concentrations and optimisation of arterial oxygénation and venous admixture by selective pulmonary artery infusion of prostaglandin E1 during thoracotomy. Anaesthesia 1996; 51: 422–6.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Chen, T.L., Lin, C.J., Lai, H.S. et al. Anaesthetic managements for conjoined twins with complex cardiac anomalies. Can J Anaesth 43, 1161–1167 (1996). https://doi.org/10.1007/BF03011846
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011846