
Abstract
Purpose
This study was designed to describe the early recovery characteristics, as well as the speed of onset of neuromuscular block, after a combination of mivacurium and vecuronium.
Methods
In this controlled, randomized study, 30 consenting ASA I–III patients were assigned to three treatment groups. The “2M2V” group received twice the dose necessary to cause 95% depression of the evoked twitch response (2 × ED95) of mivacurium (0.15 mg · kg−1) plus 2 × ED95 of vecuronium (0.1 mg · kg−1); the “2V” group received 2 × ED95 of vecuronium; and the “4V” group received 4 × ED95 of vecuronium. Evoked neuromuscular responses of the adductor pollicis were assessed with an adductor pollicis force transducer. The time until maximum block and times to 10% and 25% recovery (T10 and T25) in each group were expressed as mean ± standard deviation and compared using ANOVA.
Results
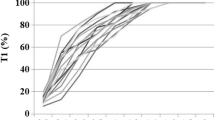
Onset of block in the 2M2V group was 27% faster than in the 2V group (2.0 ± 0.6 vs. 2.7 ± 0.8 min respectively, P < 0.05) and was similar to the 4V group (1.95 ± 0.3 min, P = NS). The times until 10% recovery were similar in the 2M2V and 4V groups (59.9 ± 12 vs 68.2 ± 25 min, P = NS) and were slower than in the 2V group (37.2 ± 9 min, P < 0.05). Between T10 and T25, recovery after 2M2V resembled that after 2V (6.7 ± 3 vs 5.7 ± 1 min, P = NS) and was faster than after 4V (10.9 ± 7 min, P<0.05).
Conclusions
When 2 × ED95 of mivacurium is added to 2 × ED95 of an intermediate or long-acting relaxant, recovery after T10 will proceed as if one had administered the longeracting agent alone.
Résumé
Objectif
Décrire les caractéristiques de la curarisation initiale et de la décurarisation après l’administration du mivacurium associé au vécuronium.
Méthodes
Au cours de cette étude contrôlée aléatoire, 30 adultes consentants ASA I–III ont été répartis en trois groupes. Le groupe 2M2V a reçu deux fois la dose (2 × ED95) de mivacurium (0,15 mg · kg−1) nécessaire pour causer une dépression de 95% de la réponse au twitch plus 2 × ED95 de vécuronium (0,1 mg · kg−1), le groupe 2V a reçu 2 × ED95 de vécuronium, et le groupe 4V, 4 × ED95 de vécuronium. Les réponses évoquées au niveau de l’adducteur du pouce ont été évaluées à l’aide d’un transducteur. Les temps nécessaires à une curarisation maximale et à 10% et 25% de décurarisation (T10 et T25) dans chaque groupe ont été exprimés en moyenne ± écart-type et comparés avec ANOVA.
Résultats
Le début de la curarisation dans le groupe 2M2V a été de 27% plus rapide que dans le groupe 2V (respectivement 2,0 ± 0,6 vs 2,7 ± 0,8 min, P < 0,05) et identique au groupe 4V (1,95 ± 0,3 min, P = NS). Le temps nécessaire à 10% de décurarisation a été identique dans les groupes 2M2V et 4V (59 ± 0,3 vs 68 ± 25 min, P = NS) et était plus prolongé que dans le groupe 2V (37,2 ± 0 min, P < 0,05). La décurarisation entre T10 et T25 était identique après 2M2V et 2V (6,7 vs 5,7 ± 1 min, P = NS) et était plus rapide après 4V (10,9 ± 7 min, P < 0,05).
Conclusion
Quand le mivacurium 2 × ED95 est ajouté à ≥ 2 × ED95 d’un relaxant intermédiaire ou de longue durée, la décurarisation après T10 a les mêmes caractéristiques qu’un agent de longue durée administré seul.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Savarese JJ, Ali HH, Basta SJ, et al. The cardiovascular effects of mivacurium chloride (BW B1090U) in patients receiving nitrous oxide-opiate-barbiturate anesthesia. Anesthesiology 1989; 70: 386–94.
Jalkanen L, Meretoja OA, Taivainen T, Brandom BW, Dayal B. Synergism between atracurium and mivacurium compared with that between vecuronium and mivacurium. Anesth Analg 1994; 79: 998–1002.
Naguib M. Neuromuscular effects of rocuronium bromide and mivacurium chloride administered alone and in combination. Anesthesiology 1994; 81: 388–95.
Savarese JJ, Ali HH, Basta SJ, et al. The clinical neuromuscular pharmacology of mivacurium chloride (BW B 1090U). A short-acting nondepolarizing ester neuromuscular blocking drug. Anesthesiology 1988; 68: 723–32.
Cook DR, Stiller RL, Weakly JN, Chakravorti S, Brandom BW, Welch RM. In vitro metabolism of mivacurium chloride (BW B1090U) and succinylcholine. Anesth Analg 1989; 68: 452–6.
Cook DR, Freeman JA, Lai AA, et al. Pharmacokinetics of mivacurium in normal patients and in those with hepatic or renal failure. Br J Anaesth 1992; 69: 580–5.
Caldwell JE, Heier T, Kitts JB, Lynam DP, Fahey MR, Miller RD. Comparison of the neuromuscular block induced by mivacurium, suxamethonium or atracurium during nitrous oxide-fentanyl anaesthesia. Br J Anaesth 1989; 63: 393–9.
Kopman AF. Tactile evaluation of train-of-four count as an indicator of reliability of antagonism of vecuroniumor atracurium-induced neuromuscular blockade. Anesthesiology 1991; 75: 588–93.
Viby-Mogensen J. Clinical assessment of neuromuscular transmission. Br J Anaesth 1982; 54: 209–23.
Silverman DG, Bartkowski RR. Pharmacokinetics and pharmacodynamics of nondepolarizing relaxants: maintenance and recovery.In: Silverman DG. (Ed.). Neuromuscular Block in Perioperative and Intensive Care. Philadelphia: J.B. Lippincott, 1994: 95–103.
Choi WW, Mehta MP, Murray DJ, et al. Neuromuscular and cardiovascular effects of mivacurium chloride in surgical patients receiving nitrous oxide-narcotic or nitrous oxide-isoflurane anaesthesia. Can J Anaesth 1989; 36: 641–50.
Weber S, Brandom BW, Powers DM, et al. Mivacurium chloride (BW B1090U)-induced neuromuscular blockade during nitrous oxide-isoflurane and nitrous oxide-narcotic anesthesia in adult surgical patients. Anesth Analg 1988; 67: 495–9.
Beauvoir C, Peray P, Daures JP, Peschaud JL, D’Athis F. Pharmacodynamics of vecuronium in patients with and without renal failure: a meta-analysis. Can J Anaesth 1993; 40: 696–702.
Silverman DG, Mirakhur RK. Intermediate-acting relaxants of the 1980s.In: Silverman DG. (Ed.). Neuromuscular Block in Perioperative and Intensive Care. Philadelphia: J.B. Lippincott, 1994: 184–99.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Stout, R.G., Brull, S.J., Kelly, D. et al. Early neuromuscular recovery characteristics following administration of mivacurium plus vecuronium. Can J Anaesth 43, 358–361 (1996). https://doi.org/10.1007/BF03011714
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011714