
Summary
Changes in functional residual capacity and their relationship to alveolararterial oxygen difference were observed during the course of respiratory failure in twelve patients. The influence of recumbency and oxygen breathing on frc in normal subjects was also examined.
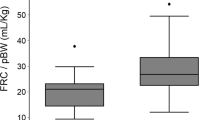
Low resting lung volumes and large alveolar-arterial oxygen differences were often observed at the time of admission in respiratory failure. The reduction in frc cannot be explained on the basis that these measurements were made in recumbent patients breathing a high concentration of oxygen in the inspired gas.
An increase in frc was often associated with an improvement in oxygenation, and it is inferred that in these patients correction of frc is associated with the opening up of previously non-ventilated alveoli, and that therapy designed with this objective is therefore justified. However, when extremely low resting lung volume is due to causes not reversible mechanically, such as diffuse pneumonia, large tidal volume ventilation determined on a body weight basis may not be indicated. Measurement of frc is not recommended for routine clinical management.
Résumé
Au cours de ľinsuffisance respiratoire survenue chez 12 malades, nous avons réussi à observer les modifications de la capacité résiduelle fonctionnelle et leur relation avec la différence en oxygène alvéolaire et artérielle. Nous avons également étudié chez des sujets normaux les effets du décubitus et de la ventilation à ľoxygène sur la capacité fonctionnelle résiduelle.
Au moment de ľadmission pour insuffisance respiratoire, nous avons noté des volumes pulmonaires restreints au repos et de grandes différences en oxygène alvéolaire et artérielle. La diminution de la capacité fonctionnelle résiduelle ne s’applique pas par le fait que ces mesures ont été faites sur des malades en décubitus et respirant une atmosphère à haute concentration en oxygène.
Une augmentation de la capacité fonctionnelle résiduelle a souvent été accompagnée ďune amélioration de ľoxygénation et ľon conclut que, chez ces malades, la correction de la capacité fonctionnelle résiduelle s’accompagne de ľouverture ďalvéoles non ventilées antérieurement et qu’ainsi, la thérapie préconisée dans ce but devient alors justifiée. Toutefois, lorsque de très petits volumes respiratoires au repos sont dus à des causes impossibles à vaincre mécaniquement, comme une pneumonie diffuse, il peut ne pas être indiqué de faire une ventilation à grand volume ďair courant calculée ďaprès le poids du malade. Nous ne recommandons pas le calcul de la capacité fonctionnelle résiduelle comme conduite clinique de routine.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Bendixen, H. H.;Hedley-Whyte, J.; &Laver, M. B. Impaired Oxygenation in Surgical Patients during General Anesthesia with Controlled Ventilation. New England J. Med.260: 991 (1963).
Hedley-Whyte, J.;Pontoppidan, H.; &Jocelyn Morris, M. The Response of Patient with Respiratory Failure and Cardio-pulmonary Disease to Different Levels of Constant Volume Ventilation. J. Clin. Invest.34: 1005 (1955).
Pontoppidan, H.;Hedley-Whyte, J.;Bendixen, H. H.;Laver, M. B.; &Radford, E. P. Jr. Ventilation and Oxygen Requirements during Prolonged Artificial Ventilation in Patients with Respiratory Failure. New England J. Med.273: 401 (1963).
Laver, M. B.;Morgan, J.;Bendixen, H. H.; &Radford, E. P. Jr. Lung Volume, Compliance and Arterial Oxygen Tensions during Controlled Ventilation. J. Appl. Physiol.19: 725 (1964).
Colgan, F. J.;Whang, T. B.; &Gillies, A. J. Atelectasis and Pneumothorax. Anesthesiology.29: 923 (1968).
Beecher, H. K. Effect of Laparotomy on Lung Volume: Demonstration of a New Type of Pulmonary Collapse. J. Clin. Invest.12: 651 (1933).
Huertado, A. &Fray, W. W. Studies of Total Pulmonary Capacity and Its Subdivisions: III. Changes with Body Posture. J. Clin. Invest.12: 825 (1933).
Whitfield, A. G. W.;Waterhouse, A. J. H.; &Arnott, W. The Total Lung Volume and Its Subdivisions: A Study in Physiological Norms. I. Basic Data. Brit. J. Social Med.4 (1950).
Lin, T. P. K. &Leift, V. C. Alterations in Lung Compliance and Functional Residual Capacity with Posture. J. Appl. Physiol.14: 164 (1959).
Déry, R.;Pelletier, J.;Jacques, A.;Clavet, M.; &Houde, J. Alveolar Collapse Induced by Denitrogenation. Canad. Anaesth. Soc. J.12: 531 (1965).
Meneely, G. R.;Ball, C. O. T.;Kory, R. C.;Galloway, J. J.;Merrill, J. M.;Mare, R. E.;Roehm, D. C.; &Kaltreider, N. L. A simplified Closed Circuit Helium Dilution Method for the Determination of the Residual Volume of the Lungs. Am. J. Med.29: 824 (1960).
Colgan, F. J. &Whang, T. B. A Method for Measuring the Functional Residual Capacity and Dynamic Lung Compliance during Oxygen and Halothane Inhalation. Anesthesiology.28: 559 (1967).
Laws, A. K. Effect of Induction of Anaesthesia and Muscle Paralysis on Functional Residual Capacity of the Lungs. Canad. Anaesth. Soc. J.15: 325 (1968).
Fairley, H. B. &Britt, B. A. The Adequacy of the Air-mix Control in Ventilators Operated from an Oxygen Source. C.M.A.J.90: 1394 (1964).
Dubois, A. B.;Turaids, T.;Mammar, R. E.; &Nebrega, F. T. Pulmonary Atelectasis in Subjects Breathing Oxygen at Sea Level and at Simulated Altitude. J. Appl. Physiol.21: 828 (1966).
McIntyre, R. W.;Laws, A. K.; &Ramachandran, P. R. Positive Expiratory Pressure Plateau: Improved Gas Exchange during Mechanical Ventilation. Canad. Anaesth. Soc. J.16: 477 (1969).
Finley, T. N. The Determination of Uneven Pulmonary Blood Flow from the Arterial Oxygen Tension during Nitrogen Washout. J. Clin. Invest.40: 1727 (1961).
Said, S. I. &Benergee, C. M. Venous Admixture to the Pulmonary Circulation in Human Subjects Breathing 100% Oxygen. J. Clin. Invest.42: 597 (1963).
Morgan, E. A. &Nahas, G. G. Study of Relationship of Arterial Oxygen Tension to Alveolar Oxygen Pressure in Man Utilizing a Polarometric Method for Whole Blood (abstract). Am. J. Physiol.163: 736 (1950).
Mead, J. Mechanics of Respiratory Structures.In: Ciba Foundation Symposium on Pulmonary Structure and Function. London: Churchill III (1962).
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ramachandran, P.R., Fairley, H.B. Changes in functional residual capacity during respiratory failure. Can. Anaesth. Soc. J. 17, 359–369 (1970). https://doi.org/10.1007/BF03004699
Issue Date:
DOI: https://doi.org/10.1007/BF03004699