
Abstract
Objectives
To examine the frequency of limiting (withdrawing and withholding) therapy in the intensive care unit (ICU), the grounds for limiting therapy, the people involved in the decisions, the way the decisions are implemented and the patient outcome.
Design
Prospective survey. Ethical approval was obtained.
Setting
ICUs in tertiary centres in London and Cape Town.
Patients
All patients who died or had life support limited.
Interventions
Data collection only.
Results
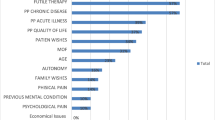
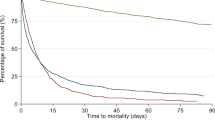
There were 65 deaths out of 945 ICU discharges in London and 45 deaths out of 354 ICU discharges in Cape Town. Therapy was limited in 81.5% and 86.7% respectively (p=0.6) of patients who died. The mean ages of patients whose therapy was limited were 60.2 years and 51.9 years (p=0.014) and mean APACHE II scores 18.5 and 22.6 (p=0.19) respectively. The most common reason for limiting therapy in both centres was multiple organ failure. Both medical and nursing staff were involved in most decisions, which were only implemented once wide consensus had been reached and the families had accepted the situation. Inotropes, ventilation, blood products, and antibiotics were most commonly withdrawn. The mean time from admission to the decision to limit therapy was 11.2 days in London and 9.6 days in Cape Twon. The times to outcome (death in all patients) were 13.2 h and 8.1 h respectively.
Conclusions
Withdrawal of therapy occurred commonly, most often because of multiple organ failure. Wide consensus was reached before a decision was made, and the time to death was generally short.
Article PDF
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
References
Smedira NG, Evans BH, Grais LS et al (1990) Withholding and withdrawal of life support from the critically ill. N Engl J Med 322:309–315
Zimmerman JE, Knaus WA, Sharpe SM et al (1986) The use and implications of do not resuscitate orders in intensive care units. JAMA 255:351–356
Daffurn K, Kerridge R, Hillman KM (1992) Active management of the dying patient. Med J Aust 157:701–704
Vincent JL (1990) European attitudes towards ethical problems in intensive care medicine: results of an ethical questionnaire. Intensive Care Med 16:256–264
Society of Critical Care Medicine ethics committee (1992) Attitudes of critical care medicine professionals concerning life-sustaining treatments. Crit Care Med 20: 320–326
Wood GG, Martin E (1995) Withholding and withdrawing life-sustaining therapy in a Canadian intensive care unit. Can J Anaesth 42:186–191
American Thoracic Society (1991) Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis 144:726–731
ACCP/SCCM consensus panel (1990) Ethical and moral guidelines for the initiation, continuation, and withdrawal of intensive care. Chest 97:949–961
Benatar SR, Abels C, Abratt R et al (1994) Statement on withholding and withdrawing life-sustaining therapy. S Afr Med J 84:254–256
Osborne ML (1992) Physician decisions regarding life support in the intensive care unit. Chest 101:217–224
Luce JM, Raffin TA (1988) Withholding and withdrawal of life support from critically ill patients. Chest 94:621–626
Fisher MM, Raper RF (1990) Withdrawing and withholding treatment in intensive care. Parts 1–3. Med J Aust 153:217–225
Wanzer SH, Federman DD, Adelstein SJ et al (1989) The physician's responsibility toward hopelessly ill, patients. A second look. N Engl J Med 320:844–849
Meisel A (1991) Legal myths about terminating life support. Arch Intern Med 151:1497–1502
Teres D (1993) Trends from the United States with end of life decisions in the intensive care unit. Intensive Care Med 19: 316–322
Task force on ethics of the Society of Critical Care Medicine (1990) Crit Care Med 18:1435–1439
Pallis C (1983) ABC of brain stem death. BMJ Press, London
Levy DE, Bates D, Caronna JJ et al (1981) Prognosis in nontraumatic coma. Ann Intern Med 94:293–301
Knaus WA, Draper EA, Wagner DP et al (1985) Prognosis in acute organ-system failure. Ann Surg 202:685–693
Faber-Langendoen K, Bartels DM (1992) Process of forgoing life-sustaining treatment in a university hospital: an empirical study. Crit Care Med 20:570–577
Orentlicher D (1992) The illusion of patient choice in end-of-life decisions. JAMA 267:2101–2104
Emmanuel LL, Barry MJ, Stoekle JD et al (1994) Advance directives for medical care: a case for greater use. N Engl J Med 324:889–895
Emanuel LL, Emanuel EJ, Stoeckle JD et al (1994) Advance directives. Stability of patients' treatment choices. Arch Intern Med 154:209–217
Block AJ (1993) Living wills are overrated. Chest 104:1645–1646
Murphy DJ, Burrows D, Santilli S et al (1994) Theinfluence of the probability of survival on patients' preferences regarding cardiopulmonary resuscitation. N Engl J Med 330:545–549
Christakis NA, Asch DA (1993) Biases in how physicians choose to withdraw life support. Lancet 342:642–646
Schneiderman LJ, Faber-Langendoen K, Jecker NS (1994) Beyond futility to an ethic of care. Am J Med 96:110–114
Dunstan GR (1985) Hard questions in intensive care. Anaesthesia 40:479–482
Koch KA, Rodeffer HD, Wears RL (1994) Changing patterns of terminal care management in an intensive care unit. Crit Care Med 22:233–243
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Turner, J.S., Michell, W.L., Morgan, C.J. et al. Limitation of life support: Frequency and practice in a London and a Cape Town intensive care unit. Intensive Care Med 22, 1020–1025 (1996). https://doi.org/10.1007/BF01699222
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01699222