
Abstract
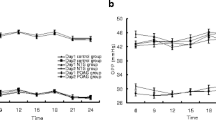
Using pneumotonometry combined with a Langham ocular blood-flow system, measurements of pulsatile ocular blood flow (POBF) were performed in eight ocular normotensive patients with implanted cardiac pacemakers, with the subjects assuming both the erect and the supine postures. Sequential measurements of POBF were made at pre-set values of heart rate over the physiological range between 60 and 120 beats/min at intervals of 10 beats/min. With patients in the supine position, measurements of cardiac output and stroke volume indices were also recorded by impedance cardiography. The mean pulse amplitude of the intraocular pressure (the ocular pulse) decreased as heart rate increased, and this change was statistically significant in both postures according to repeated-measures analysis of variance (erect: f=18.7, P < 0.0001; supine: f=18.8, P<0.0001). As measured in supine patients following an increase in heart rate, the pulse amplitude decreased in parallel with a decline in stroke volume index (f=18.8, P<0.0001). Up to a level of 90 beats/min, the mean POBF increased with heart rate, but it declined above this rate in both erect and supine postures. At all heart rates, intraocular pressure was higher when subjects were supine than when they stood erect (f=4.3, P<0.001). At lower heart rates of 70 and 80 beats/min, ocular pulse volume and POBF were significantly lower in supine patients than in erect subjects (70 beats/min: t=3.89, P<0.01 vs; t=3.87, P<0.01; 80 beats/min: t=2.85, P< 0.05 vs ; t = 2.87, P< 0.05). We conclude that when the heart rate is under normal physiological drive, the decline in POBF that accompanies the act of lying down is determined both by the change in posture itself and by the fall in heart rate that is associated with it. These observations suggest a possible disadvantage inherent in the use of anti-glaucoma drugs that inter alia induce bradycardia.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Berne RM, Levy MN (eds) (1988) Physiology, 2nd edn. Mosby, St. Louis, pp 472–485
Bernstein DP (1986) Continuous noninvasive real-time monitoring of stroke volume and cardiac output by thoracic electrical bioimpedance. Crit Care Med 14:898–901
Bernstein DP (1986) A new stroke volume equation or thoracic electrical bioimpedance: theory and rationale. Crit Care Med 14:904–909
Bray JJ, Cragg PA, Macknight ADC, Mills RG, Taylor DW (eds) (1989) Lecture notes in human physiology, 2nd edn. Blackwell, Oxford, pp 456–460
Canning CR, Restori M (1988) Doppler ultrasound studies of the ophthalmic artery. Eye 2:92–95
Riva CE, Grunwald JE, Petrig BL, Sinclair SH (1985) Blood velocity and volumetric flow rate in human retinal vessels. Invest Ophthalmol Vis Sci 26:1124–1132
Rosenqvist M, Botvinick EH, Abbott JA, O'Connell W, Cockrell J, Griffin JC (1989) The importance of abnormal pattern of ventricular depolarization, a comparison between atrial, AV-sequential and ventricular pacing. Pace 12:509–515
Roy MS, Harrison KS, Harvey E, Mitchell T (1989) Ocular blood flow in dogs using radiolabelled microspheres. Int J Radiat Appl Instrum [B] 16:81–84
Shepherd JT, Vanhoutte PM (1979) The human cardiovascular system. Facts and concepts. Raven Press, New York, pp 158–161
Sowton E, Siddon A (1976) Cardiac pacemakers. Thomas, Springfield
Trew DR, Smith SE (1991) Postural studies in pulsatile ocular blood flow: 1. Ocular hypertension and normotension. Br J Ophthalmol 75:66–70
Trew DR, Smith SE (1991) Postural studies in pulsatile ocular blood flow: 2. Chronic open angle glaucoma. Br J Ophthalmol 75:71–75
Author information
Authors and Affiliations
Additional information
Offprint requests to: D.R. Trew
Rights and permissions
About this article
Cite this article
Trew, D.R., James, C.B., Thomas, S.H.L. et al. Factors influencing the ocular pulse — the heart rate. Graefe's Arch Clin Exp Ophthalmol 229, 553–556 (1991). https://doi.org/10.1007/BF00203321
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00203321