
Abstract
Background
Bronchiectasis is an important cause of morbidity and mortality all over the world. Determining the frequency of actual occurrence is particularly misleading and difficult to determine, especially in patients with multiple respiratory disorders, because it can be a result of any primary pulmonary disease. The objective of this study was to evaluate the effect of readmission with acute exacerbation of bronchiectasis (AEB) on the admissions later on, need of long-term O2 and mechanical ventilation, and mortality.
Patients and methods
This is an observational cohort and prospective study. It was conducted on patients admitted with AEB who achieved modified O’Donnell criteria, and their high-resolution computed tomography showed bronchiectasis on admission at Aleppo University Hospital between September 2017 and January 2019. They were divided into three groups by age. Patients with bronchial asthma, chronic obstructive pulmonary disease, and cystic fibrosis were excluded.
Results
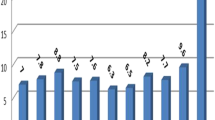
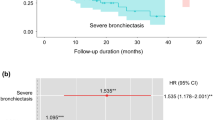
The study included 90 patients (57 males and 33 females) with a mean age of 52.93 ±20.437 years. AEB showed a peak of incidence in the age group 41–65 years. Dyspnea is the most common symptom in exacerbations (88.23%) followed by hemoptysis (80.88%). Wheezing had the least frequency on admission (60.29%). Median survival age was 14±0.214 months. We collected information on 136 exacerbations in 90 patients. A total of 31 (34.44%) patients had at least one readmission and 19 (21%) patients died within 12 months of admission to the hospital. Age, smoking, and need of long-term O2 were statistically significant between the two groups of study (P=0.013, <0.0001, and 0.04, respectively). Sex, radiological changes, mortality, and mechanical ventilation have no significance.
Conclusion
AEB is a common reason for hospitalization, and it correlates with age, smoking, readmission, and need of long-term O2 treatment.
Article PDF
Similar content being viewed by others

References
McShane PJ, Naureckas ET, Tino G, Strek ME. Non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med 2013; 188:647–656.
Bird K, Memon J. Bronchiectasis. InStatPearls [Internet] 2017 Nov 12. StatPearls Publishing Bronchiectasis.
Gupta A, Verma UP, Verma AK, Choudhary SC, Sharma S, Singh N, Sharma D. Periodontal diseases: a covert focus of inflammation in pulmonary diseases. Indian J Respir Care 2019; 8:8.
Amorim A, Gamboa F, Sucena M, Cunha K, Anciães M, Lopes S, et al. Recommendations for aetiological diagnosis of bronchiectasis. Rev Portug Pneumol 2016; 22:222–235.
Cantin L, Bankier AA, Eisenberg RL. Bronchiectasis. Am J Roentgenol 2009; 193:W158–W171.
Deslauriers J. Surgical treatment of bronchiectasis. Adv Therapy Thorac Surg 2005; 2:266.
Morrissey BM, Evans SJ. Severe bronchiectasis. Clin Rev Allergy Immunol 2003; 25:233–247.
Eastham KM, Fall AJ, Mitchell L, Spencer DA. The need to redefine non-cystic fibrosis bronchiectasis in childhood. Thorax 2004; 59:324–327.
Roberts ME, Lowndes L, Milne DG, Wong CA. Socioeconomic deprivation, readmissions, mortality and acute exacerbations of bronchiectasis. Intern Med J 2012; 42:e129–e136.
Seitz AE, Olivier KN, Adjemian J, Holland SM, Prevots DR. Trends in bronchiectasis among medicare beneficiaries in the United States, 2000 to 2007. Chest 2012; 142:432–439.
Quint JK, Millett ER, Joshi M, Navaratnam V, Thomas SL, Hurst JR, et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: a population-based cohort study. Eur Respir J 2016; 47:186–193.
O’Donnell AE, Barker AF, Ilowite JS, Fick RB, rhDNase Study Group. Treatment of idiopathic bronchiectasis with aerosolized recombinant human DNase I. Chest 1998; 113:1329–1334.
Goeminne PC, Nawrot TS, Ruttens D, Seys S, Dupont LJ. Mortality in non-cystic fibrosis bronchiectasis: a prospective cohort analysis. Respir Med 2014; 108:287–296.
Machado BC, Jacques PS, Penteado LP, Dalcin PD. Prognostic factors in adult patients with non-cystic fibrosis bronchiectasis. Lung 2018; 196:691–697.
Sadigov A. Factors associated with hospitalization and mortality in noncystic fibrosis bronchiectasis exacerbations: one-year follow-up study. Chest 2018; 154:4.
Zaibi H, Missaoui L, Dhahri B, Fezai N, Azzebi S, Baccar MA, et al. Acute exacerbation in patients with bronchiectasis: what prognostic factors?
Hamdi B, Moussa I, Berraies A, Touil A, Ammar J, Hamzaoui A. Exacerbations of bronchiectasis: etiology and outcome. 2016.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alduihi, F.A., Khoury, A. Factors affecting readmitted patients with acute exacerbation of bronchiectasis. Egypt J Intern Med 31, 779–782 (2019). https://doi.org/10.4103/ejim.ejim_44_19
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/ejim.ejim_44_19