
Abstract
Objectives
To perform an interprovincial comparison of unintentional population-based injury hospitalization and death rates for Canadian children ages 0–19 years and compare trends between 2006 and 2012.
Methods
Annual population-based hospitalization rates per 100,000 from unintentional injuries were calculated for children/youth (< 19 years) using data from the Discharge Abstract Database between 2006 and 2012. Annual mortality rates were analyzed using provincial coronial data. The mean annual change in the rate of hospitalizations due to unintentional injuries was reported for each province.
Results
The average annual rate of hospital admissions for unintentional injuries was 305.10 per 100,000 population between 2006 and 2012, and this decreased by − 11.91 over time (p < 0.01, − 15.85; − 7.77). Saskatchewan had the highest average annual morbidity rate (550.76 per 100,000) from all unintentional causes, and Ontario had the lowest average annual rate (238.89 per 100,000). Saskatchewan had the highest average annual rate for all subcauses except for drowning. Ontario was the only province with an average annual injury morbidity rate that was consistently below the Canadian average. The average annual mortality rate from all unintentional injury was highest in Saskatchewan (17.51 per 100,000) and lowest in Ontario (5.99 per 100,000) when compared to Canada (7.97 per 100,000).
Conclusion
Injury prevention policies vary considerably among provinces. Although the unintentional injury hospitalization rate is decreasing over time, some subcauses such as choking/suffocation have shown an increase in certain provinces. Evidence-based childhood injury prevention policies, such as playground equipment safety and four-sided pool fencing among others, should be standardized across Canada.
Résumé
Objectifs
Effectuer une comparaison interprovinciale des taux d’hospitalisation et de mortalité dus aux blessures non intentionnelles dans la population des enfants canadiens de 0 à 19 ans et comparer les tendances entre 2006 et 2012.
Méthode
Les taux d’hospitalisation annuels p. 100 000 habitants dus aux blessures non intentionnelles ont été calculés pour les enfants et les jeunes (< 19 ans) à l’aide des données de la Base de données sur les congés des patients pour la période de 2006 à 2012. Les taux de mortalité annuels ont été analysés à l’aide des données des coroners provinciaux. Le changement annuel moyen du taux d’hospitalisation pour blessures non intentionnelles a été déclaré pour chaque province.
Résultats
Le taux annuel moyen d’hospitalisation pour blessures non intentionnelles a été de 305,10 p. 100 000 entre 2006-2012 et a diminué de -11,91 avec le temps (p < 0,01, -15,85; -7,77). La Saskatchewan a affiché le taux annuel moyen de morbidité le plus élevé (550,76 p. 100 000), toutes causes non intentionnelles confondues, et l’Ontario, le taux annuel moyen le plus faible (238,89 p. 100 000). La Saskatchewan a présenté le taux annuel moyen le plus élevé pour toutes les causes secondaires sauf les noyades. L’Ontario a été la seule province où le taux annuel moyen de morbidité était systématiquement en deçà de la moyenne canadienne. Le taux annuel moyen de mortalité pour l’ensemble des blessures non intentionnelles a été le plus élevé en Saskatchewan (17,51 p. 100 000) et le plus faible en Ontario (5,99 p. 100 000) par rapport à la moyenne canadienne (7,97 p. 100 000).
Conclusion
Les politiques de prévention des blessures varient considérablement d’une province à l’autre. Bien que le taux d’hospitalisation pour blessures non intentionnelles ait diminué au fil du temps, certaines causes secondaires, comme l’étouffement/la suffocation, sont en hausse dans certaines provinces. Les politiques de prévention des blessures chez les enfants fondées sur les preuves, entre autres les politiques sur la sécurité des équipements de jeu et sur les clôtures à quatre côtés autour des piscines, devraient être normalisées à l’échelle du Canada.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
In Canada, injuries kill more children and youth over the age of 1 year than any other cause (Public Health Agency of Canada 2008). Unintentional injuries are defined as injuries that are not caused with intention to harm (Chen et al. 2013). Over 10,000 Canadians died in 2010 as the result of an unintentional injury, which amounted to a total economic burden of $22.1 billion (Parachute, n.d.). According to a report that highlighted the differences in economic burden resulting from unintentional injuries across Canada (Parachute, n.d.), the economic cost per capita and potential years of life lost (PYLL) from injury varied by province. PYLL in Canada was 1337 per 100,000 population in 2010 with an average economic cost of $788 per capita. Ontario had the lowest number of PYLL (1128 per 100,000) while Saskatchewan had the highest (1953 per 100,000). Other studies have reported that among different provinces, the annual number of injuries varies. Chen et al. (2013) reported that between 2001 and 2007, British Columbia had the lowest overall mortality rate, and Newfoundland and Labrador had the lowest mortality rate for unintentional injuries, specifically (Chen et al. 2013). However, these injuries differ by subcause.
Falls are the leading cause of hospitalization for unintentional injury in Canada, accounting for 37% of hospitalizations (Yanchar et al. 2012). Falls accounted for 26% of all unintentional injury deaths in Canada for the period 2001 to 2007 (Chen et al. 2013). In another study that examined adolescent injury deaths and hospitalizations in Canada between 1979 and 2003, researchers found that among adolescents aged 15–19 years of age, falls were a main cause for injury hospitalization (Pan et al. 2007).
Unintentional poisoning, burns, choking, and drowning-related injuries are other significant causes of hospitalization and death in Canada. In 2016, Clemens et al. published a population-based study of drowning in Canada. The authors reported that between 2008 and 2012, the mean incidence rate of unintentional water-related fatalities was 1.05, 0.57, and 1.27 per 100,000 for children and youth ages 0–4, 5–14, and 15–19 years, respectively (Clemens et al. 2016). Injury prevention policies and legislation that aim to prevent unintentional injuries from a number of causes vary across the country (Macpherson et al. 2015; Rothman et al. 2016).
A policy is often considered a form of government action that may involve the modification or implementation of resources to support a value such as injury prevention or safety promotion (Macpherson et al. 2015). Some examples of injury prevention policies include window safety mechanisms to prevent fall-related injuries, four-sided pool fencing to prevent drowning-related injuries, and child-proof medical containers to prevent unintentional poisoning (Macpherson et al. 2015). Although evidence on the effectiveness of a number of these injury prevention policies exists and has been demonstrated over time, there is still a lack of harmonization of these policies across jurisdictions (Macpherson et al. 2015).
Given the burden of unintentional injuries among children and youth resulting from a number of preventable causes, together with the variability in provincial injury prevention policies and legislation in Canada, our objective was to perform an interprovincial comparison of unintentional population-based injury hospitalization and death rates for Canadian children and youth ages 0–19 years for the period 2006 to 2012.
Methods
Data collection
We conducted a retrospective analysis using morbidity data from the Canadian Institutes for Health Information (CIHI), extracted from the Discharge Abstract Database (DAD) (Canadian Institute for Health Information (CIHI) 2016). This database collects information on all hospital discharges, including deaths, sign-outs, and transfers. Data are collected from all provinces and territories except for Quebec (QC), which is not required to report these data. The territories were not included in this study because we were unable to investigate data by year due to small cell sizes. All children aged 0–19 years were included in this study; this number formed the denominator for computing injury rates. We obtained our denominators (i.e., number of children aged 0–19 years in each province) from Statistics Canada (2006–2012). Included data are collected by health professionals and later assigned diagnostic codes by health records personnel using the International Classification of Diseases and Related Health Problems, 10th revision, Canada (ICD-10-CA). ICD-10-CA external codes for unintentional injury mechanisms were categorized as V01-X59 and Y85-Y86. The overall category of unintentional injuries includes the following subcauses: transport, falls, poisonings, burns, choking, and drowning. All subcauses except transport-related injuries (occupant, cyclist, and pedestrian) were analyzed as we chose to focus solely on transport-related causes in a separate study. The DAD consists of many variables, some of which include sex, age, and diagnosis. Data are available for fiscal years 1979–1980 and 1994 onwards. Children and adolescents aged 0 to 19 years of age who were hospitalized after sustaining an unintentional injury between January 1, 2006 and December 31, 2012 in all provinces excluding QC were included in this study.
Mortality data were obtained from official coroners or medical examiners files at the provincial level. We excluded QC to be consistent with morbidity data over the same time period. Subcause analyses were not performed on mortality data since cell sizes were too small to report. Children and adolescents who died as the result of an unintentional injury between January 1, 2006 and December 31, 2012 were included in this study using coronial data.
Study variables
The primary outcome measure in this study was any unintentional injury-related hospitalization or death sustained between 2006 and 2012 in Canada. A number of variables were analyzed in this study, including cause of unintentional injury (ICD-10-CA codes: V01-X59 and Y85-Y86) and province of residence.
Statistical analyses
We analyzed the population-based hospitalization and mortality rates per 100,000 for each province by year, and cause of unintentional injury over the 7-year period (2006–2012), where possible, and reported the mean annual change in the rate of hospitalizations due to unintentional injuries, p values, and confidence intervals for trends over time. Admission year was used when calculating the hospitalization and mortality rates. An average annual incidence rate per 100,000 and a mean annual rate change was calculated for morbidity and mortality data over the 7-year study period. A positive mean annual rate change indicates an increase in the rate of unintentional injury hospitalization or mortality while a negative mean annual rate change indicates a decrease over time. Data analyses were conducted at the Research Data Centres (RDC) at York University using Statistical Package for the Social Sciences (SPSS) version 24 (IBM Corp n.d.). Ethics approval was obtained from York University.
Results
Unintentional injury rates in Canada
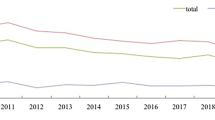
The average annual hospitalization rate for all unintentional-related injuries in Canada for children and youth (up to 19 years) was 305.10 per 100,000 population. Between 2006 and 2012, the Canadian population-based annual rates of hospital admissions from all unintentional causes decreased significantly from 335.75 to 277.69 per 100,000 (− 11.81; p < 0.01, − 15.85; − 7.77) (see Table 1). Saskatchewan (SK) had the highest average annual unintentional injury rates of hospital admissions from all causes (550.76 per 100,000) when compared to the Canadian average, and Ontario (ON) had the lowest average annual rate (238.89 per 100,000). SK’s population-based annual hospitalization rate decreased significantly over time by − 23.30 (p < 0.01, − 29.21; − 17.39). All nine Canadian provinces analyzed (excluding data from QC) showed a decrease in unintentional injury morbidity rates from 2006 to 2012, with the largest significant mean annual rate change in SK (− 23.30) (p < 0.01, − 29.21; − 17.39) and the smallest significant mean annual rate change in ON (− 5.37) (p < 0.01, − 7.69; − 3.05).
The average annual mortality rate from all unintentional injuries in Canada was 7.97 deaths per 100,000 children and youth between 2006 and 2012 (see Table 2). Compared to the Canadian average, the highest average annual mortality rate was 17.51 per 100,000 population in SK and the lowest rate was 5.99 per 100,000 in ON (see Table 2).
Provincial comparisons of unintentional injury rates by subcause
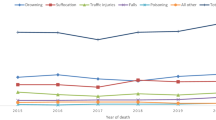
We analyzed the annual rate of unintentional injury hospitalization by a number of subcauses, including falls, poisoning, burns, choking, and drowning. Of the subcauses that were analyzed, falls accounted for the highest unintentional injury rates among children, with an average of 112.49 per 100,000 in Canada; these annual rates decreased significantly by − 2.71 annually (p < 0.01, − 3.50; − 1.93). Drowning demonstrated the lowest average annual hospitalization rate at 1.39 per 100,000 in Canada over time; this rate increased non-significantly by 0.02 annually (n.s., − 0.05; 0.09). SK had the highest average annual hospitalization rate for all subcauses except for drowning, while Manitoba (MB) had the highest average annual rate (see Table 3). SK’s annual rate of hospitalization decreased during the study period for all subcauses by − 0.10 (n.s., − 1.66; 1.45), − 0.63 (n.s., − 1.35; 0.09), − 1.95 (p < 0.01, − 3.40; − 0.49), and − 6.77 (p < 0.01, − 11.11; − 2.42) for burns, choking, poisoning, and fall-related injuries, respectively. Of these decreases, only falls and burns showed a significant reduction over time in SK. ON had the lowest average annual rate of unintentional injury hospitalization for falls, poisoning, and choking, whereas NS had the lowest average annual rate of hospitalization for burns. We were unable to report annual rates of hospitalization for burns and drowning in Prince Edward Island (PEI) since some cell sizes were less than 5.
Of the subcauses analyzed, choking-related injuries showed the highest increase (0.04) in childhood annual hospitalizations rates in Canada; this trend was not statistically significant (n.s., − 0.06; 0.14). The average annual rate of childhood choking-related injury hospitalization in Canada was 3.07 per 100,000 population. SK and AB were the only two provinces that showed a decrease in the annual rate of choking-related hospitalizations over time, − 0.63 (n.s., − 1.35; 0.09) and − 0.26 (n.s., − 0.65; 0.12), respectively, neither of which were statistically significant.
Discussion
In Canada, the annual rate of children and youth hospitalized as a result of injuries has shown an overall significant downward trend since 2006; however, the annual rate of change differs among provinces. For all-cause unintentional injury hospitalizations, including falls, poisoning, burns, choking, and drowning, SK demonstrated the largest significant decrease in unintentional average annual injury rates of hospital admissions over time (2006–2012), while ON saw the smallest significant decrease (Tables 4, 5, 6, and 7). SK had the greatest average annual rate of unintentional injury hospitalization compared to the Canadian average when examining all subcauses except drowning, while MB had the greatest average annual rate, although these findings were not statistically significant. SK had an annual hospitalization rate that was consistently above the Canadian average, but the hospitalization rate significantly decreased over the study period by − 17.69. ON was the only province with an annual unintentional injury morbidity rate that was consistently lower than the Canadian average. However, over the study period, the annual rate of hospitalization increased significantly in ON by 6.38 (p < 0.01, 1.50; 11.25).
Our study found that in Canada, fall-related injuries accounted for the highest rates of any unintentional injury subcause that was examined in this study, but decreased significantly by − 2.71 over the period under study. Only one province, PEI, showed an annual increase in the rate of fall-related hospitalizations over time. PEI had a smaller population, and therefore, rates of injuries were typically unstable in this province. In addition, the changes over time were not statistically significant. ON was the province that showed the lowest rate of annual unintentional injury hospitalization from fall-related injuries. Previous literature on fall-related injuries in a pediatric population suggests that window safety mechanisms that prevent children from being able to open windows, including devices such as bars and position locks, are one effective strategy to prevent falls (MacKay et al. n.d.; Spiegel and Lindaman 1995). Stair gates have also been shown to assist in the reduction of falls down stairs among young children (MacKay et al. n.d.; Towner et al. 2001). Although policies and legislation related to the prevention of fall-related injuries among children and youth have shown evidence of effectiveness, there are no national fall-related policies or legislation that require the installation of window bars and/or window safety devices in homes.
Another common cause of fall-related injuries is from playground equipment. In 1998, the Canadian Standards Association (CSA) introduced new guidelines to make playground equipment more safe. Intervention schools that received new, safer playground equipment saw a decrease in injuries when compared to non-intervention schools in Toronto (MacKay et al. n.d.; Canadian Standards Association n.d.; Howard et al. 2005). The CSA guidelines related to playground equipment are an example of an evidence-based policy that has shown evidence of effectiveness in reducing one cause of injury among Canadian children.
Our study found that drowning-related injuries accounted for the lowest annual rates of hospitalization of any subcause; however, drowning-related hospitalizations trended up over the study period by 0.02; these changes were not statistically significant. Safer pool-fencing legislation is one example of an evidence-based policy that has been implemented in several municipalities across Canada in an effort to prevent unintentional drowning-related incidents. The first global report on drowning claims that 75% of private backyard/garden swimming pool drowning deaths among young children could be prevented by four-sided pool fencing, completely separating the pool from the house and/or yard (World Health Organization (WHO) 2014). Despite the evidence of effectiveness, however, there is still considerable variation among provinces regarding pool fencing bylaws (Parachute, n.d.).
Additionally, choking-related injuries are common among young children. Although the annual rate of overall hospitalizations from all causes in Canada decreased over time, when we stratified by subcause, choking-related injuries showed an annual increasing trend between 2006 and 2012 by 0.04 (n.s.). Choking hazards are primarily associated with food, coins, and toys (American Academy of Pediatrics 2010). Legislation that reduces the risk of choking-related injuries in Canada, such as Bill C-36 on product safety, has not been systematically reviewed at a provincial level (Canadian Standards Association n.d.). Food is one cause of choking-related injuries among children under 3 years of age, and a mandatory system to label foods with appropriate warnings according to the associated choking risk has been suggested (American Academy of Pediatrics 2010). The number of choking-related injuries increased in Canada over time from 2.95 to 3.28 per 100,000; policies that focus on reducing these injuries should be implemented on a national basis.
This study suggests that relationships may exist between rates of child and youth injury and policy and legislation. Further research that can determine the significance of specific relationships of unintentional injury mortality and morbidity with the presence and construction of injury prevention policies is needed.
Strengths
The major strength of this study is that it highlighted the differences in annual childhood injury rates using both hospitalization and mortality data for a number of unintentional injury causes and subcauses, by province, over time. In addition, data were reported on a population-based level, permitting comparisons among provinces. These relationships serve as hypotheses for further research to determine the significance of specific relationships among unintentional injury morbidity and mortality and policy.
Limitations
We were unable to analyze mortality data by injury subcause and province, as the resultant cell sizes were too small to report (n < 5). Additionally, we were not able to include Quebec or the territories in our study. Another limitation was the lack of information around specific subcauses. For example, unintentional drowning can be coded as “drowning involving bathtub,” “drowning involving swimming pool,” “drowning involving natural water,” and “unspecified drowning,” but there is no way to ascertain if the swimming pool was a public pool or a backyard pool, for example. Another limitation to this study is that hospitalization and mortality rates did not reflect visits for less severe injuries to emergency rooms or physician’s offices.
In addition, factors other than policies and/or legislation, such as awareness campaigns, changes to the built environment, urban rural distribution of the population, or changes in health service utilization practices, may have influenced changes in the pediatric injury rates over time. Due to small cell sizes, we were unable to age-standardize the injury hospitalization rates; interprovincial differences may be attributed, in part, to differences in age distributions.
Childhood injury morbidity and mortality rates vary in Canada on a provincial level. Although overall unintentional injury rates decreased in this population over the 7-year period under study, some subcauses such as choking and drowning showed increased incidence.
This is the first study to compare injuries among children and youth across Canadian provinces in terms of hospitalization and death rates. This information may influence the entire spectrum of injury prevention, including the harmonization of policy and legislation in Canada. Future studies will be published that further describe differences between provincial injury prevention policies, including the year that legislation was implemented and the varying stipulations for each policy.
References
American Academy of Pediatrics. (2010). Policy statement—prevention of choking among children. Pediatrics, 125(3), 601–607.
Canadian Institute for Health Information (CIHI) (2016) Discharge Abstract Database (DAD) Metadata. Available at: https://www.cihi.ca/en/types-of-care/hospital-care/acute-care/dad-metadata. Accessed October 4, 2017.
Canadian Standards Association (n.d.) Children’s play spaces and equipment Z614–07, 2007.
Chen, Y., Mo, F., Yi, Q. L., Jiang, Y., & Mao, Y. (2013). Unintentional injury mortality and external causes in Canada from 2001 to 2007. Chronic Diseases and Injuries in Canada, 33(2), 95–102.
Clemens, T., Tamim, H., Rotondi, M., & Macpherson, A. K. (2016). A population based study of drowning in Canada. BMC Public Health, 16(559), 1–8.
Howard, A. W., Macarthur, C., Willan, A., Rothman, L., Moses-McKeag, A., & Macpherson, A. K. (2005). The effect of safer play equipment on playground injury rates among school children. Canadian Medical Association Journal, 172(11), 1443–1446.
IBM Corp (n.d.) Released 2016. IBM SPSS statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.
MacKay, M., Vincenten, J., Brussoni, M., Towner, E., Fuselli, P. (n.d.) Child Safety Good Practice Guide: good investments in unintentional child injury prevention and safety promotion—Canadian Edition. Available at: http://www.parachutecanada.org/downloads/research/reports/ChildSafetyGoodPracticeGuide-CanadianEdition.pdf. Accessed October 4, 2017.
Macpherson, A. K., Brussoni, M., Fuselli, P., Middaugh-Bonney, T., Piedt, S., & Pike, I. (2015). An evaluation of evidence-based paediatric injury prevention policies across Canada. BMC Public Health, 15(707), 1–7.
Pan, S. Y., Desmeules, M., Morrison, H., Semenciw, R., Ugnat, A. M., Thompson, W., & Mao, Y. (2007). Adolescent injury deaths and hospitalization in Canada: magnitude and temporal trends (1979-2003). The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 41(1), 84–92.
Parachute (n.d.-a) The cost of injury in Canada. Available at: http://www.parachutecanada.org/downloads/research/Cost_of_Injury-2015.pdf. Accessed October 4, 2017.
Parachute (n.d.-b) Preventing drowning: safer pool fencing legalisation chart. Available at: http://www.parachutecanada.org/downloads/policy/Pool_Fencing_Legislation_Chart.pdf. Accessed October 4, 2017.
Public Health Agency of Canada (2008) Leading causes of death, Canada. Available at: http://www.phac-aspc.gc.ca/publicat/lcd-pcd97/pdf/lcd-pcd-t1-eng.pdf. Accessed October 4, 2017.
Rothman, L., Pike, I., Belton, K., Olsen, L., Fuselli, P., & Macpherson, A. K. (2016). Barriers and enables to enacting child and youth related injury prevention legislation in Canada. International Journal of Environmental Research and Public Health, 13(656), 1–11.
Spiegel, C. N., & Lindaman, F. C. (1995). Children can’t fly: a program to prevent childhood mortality from window falls. Injury Prevention, 1(3), 194–198.
Towner, E., Dowswell, T., Mackereth, C., Jarvis, S. (2001) What works in preventing unintentional injuries in children and young adolescents? An updated systematic review. Prepared for the Health Development Agency (HDA), London. Department of Child Health, University of Newcastle upon Tyne, 2001.
World Health Organization (WHO) (2014) Global report on drowning: preventing a leading killer. Available at: http://apps.who.int/iris/bitstream/10665/143893/1/9789241564786_eng.pdf?ua=1&ua=1. Accessed October 4, 2017.
Yanchar, N.L., Warda, L.J., Fuselli, P. (2012). Child and youth injury prevention: a public health approach. Injury Prevention Committee, Canadian Pediatric Society, 1–9.
Acknowledgements
A.M. is supported by CIHR - Chairs in Reproductive and Child Health Services and Policy Research (#FRN 126341).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fridman, L., Fraser-Thomas, J., Pike, I. et al. An interprovincial comparison of unintentional childhood injury rates in Canada for the period 2006–2012. Can J Public Health 109, 573–580 (2018). https://doi.org/10.17269/s41997-018-0112-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/s41997-018-0112-z