
Abstract
Background
Personalized music programs have been proposed as an adjunct therapy for patients with Alzheimer disease related dementia, and multicenter trials have now demonstrated improvements in agitation, anxiety, and behavioral symptoms. Underlying neurophysiological mechanisms for these effects remain unclear.
Methods
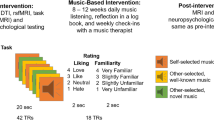
We examined 17 individuals with a clinical diagnosis of Alzheimer disease related dementia using functional MRI following a training period in a personalized music listening program.
Results
We find that participants listening to preferred music show specific activation of the supplementary motor area, a region that has been associated with memory for familiar music that is typically spared in early Alzheimer disease. We also find widespread increases in functional connectivity in corticocortical and corticocerebellar networks following presentation of preferred musical stimuli, suggesting a transient effect on brain function.
Conclusions
Findings support a mechanism whereby attentional network activation in the brain’s salience network may lead to improvements in brain network synchronization.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Individualized music programs have been proposed as adjunct treatments for a large and growing population of individuals with Alzheimer disease and related dementias (1). Approaches to formal interventions utilizing personalized music therapy consist of identifying favorite music of an individual through interviews with the individual, friends, and family, and training on a personalized music device, as well as observation of symptomatic improvement and evaluation for other causes of agitation or anxiety (2). Specific benefits from listening to personalized or favorite music, rather than background or “relaxation” music, have been shown (3, 4).
Several studies have investigated symptomatic improvements associated with personalized music therapy or listening programs. While an intervention that was not personalized for individual participants involving live music did not show benefit on levels of depression or quality of life (5), in contrast, personalized music programs have resulted in improvements in depression (6, 7), anxiety (6-9), agitation (10, 11), and behavioral symptoms (9, 12), although mixed results have also been observed (13, 14). In a retrospective study examining over 25,000 patients in long-term care facilities, those with individualized music programs showed decreased rates of antipsychotic medication, decreased anxiolytic medication, and reduced behavioral problems (15).
Even in patients with advanced dementia, music recognition appears to be a relatively spared domain of memory function (16). Memory of musical selections is preserved in patients with impaired verbal memory (17). There may be integration of music and autobiographical memory in the medial prefrontal cortex, facilitating retrieval of personally salient episodic memories when listening to familiar musical excerpts (18). Familiarity of music is directly related to engagement of brain resources in response to music (19), and positive valence of musical selection also enhances how memorable music may be (20).
Brain mechanisms for symptomatic benefits from individualized music programs are not well understood. Early reports of symptomatic improvement through personalized music therapy proposed a “Progressively Lowered Stress Threshold Model” as a conceptual framework (3, 21). This hypothesis posited that impaired sensory perception and processing lowered a stress threshold and heightened anxiety, and that familiar or personally meaningful music might be more easily perceptible than unfamiliar or background stimuli, resulting in decreased anxiety. More recent studies of emotive content of music have emphasized the role of brain reward circuits and dopamine responses as a mechanism for pleasure associated with listening to favorite music (22). Alternatively, benefits may be secondary to effects on brain attentional systems or through stimulation of brain regions associated with autobiographical stored memories. To discriminate among putative neurophysiological mechanisms, we performed functional brain imaging in a cohort of patients with mild Alzheimer disease.
Methods
All experimental procedures were performed following informed consent for research participants in accordance with protocols approved by the University of Utah Institutional Review Board and the Code of Ethics of the World Medical Association for protection of human subjects in scientific research.
Participant Selection and Characteristics
A total of 22 individuals participated in the evaluation and scanning portion of the study. After all data was collected, fMRI scans were visually inspected and pre-processed to account for head motion. Subjects with high motion during the resting-state (<100 motion-free volumes, n=4) or visible artifacts on BOLD images (n=1) were excluded from further processing, giving a final subject pool of n=17. Of these participants, there were 11 males and 6 females with a mean age of 71.82 ± 5.96 years.
Personalized Music Training
Each individual completed a period of personalized music training that consisted of meeting with the patient and caregivers, identifying favorite songs and music styles, training of patient and caregivers on an iPod device with personalized music, and confirmation over at least 3 weeks following the training that patients had used the device independently following the training.
Preferred Music for Participants
Participants submitted a list, in advance, of music that had personal significance to them. From each song, 20 second segments were selected to be played for the participant during a scan. The 20 second selections were taken from the most iconic and recognizable moments in each song. For popular music selections (i.e. country, jazz, rock, etc.), show tunes, and other modern lyrical songs selections were taken from the chorus, the first verse, or the opening of the song. For instrumental popular music, selections were taken from the refrain, introduction, or at the beginning for an iconic solo. For pieces of western art music (baroque, classical, romantic, etc.) selections were taken from easily recognizable statements of the main or secondary theme in exposition and recapitulation sections, as well as strongly defined introductions to developmental sections, and climactic cadential moments with loud dynamics. Lastly, choral selections were made similarly to popular music (choruses and introductions), but sometimes selections came from instrumental interludes with clear statements of a main theme.
Auditory Evaluation
We measured pure tone averages (PTA) in a sound booth. Subjects with a four-frequency (0.5, 1, 2, and 3 kHz) PTA greater (worse) than 40dB HL were not considered for the imaging portion of the study. This cutoff was chosen so that only subjects with relatively normal hearing or only mild hearing loss were included in the study. Subjects with hearing thresholds worse than 40dB HL could potentially confound the imaging data as we evaluate the central processing of sound because they lack peripheral (cochlear) acuity to deliver the stimulus to the brain.
For those subjects with a PTA less than 40dB HL, we measured standard word recognition scores to test peripheral auditory function. As per previously published protocols, we also administered three behavioral central auditory tests based on their standardization, ease of use, likelihood of being affected by dementia, and testing of different central auditory skills (23). The tests included the Synthetic Sentence Identification with Ipsilateral Competing Message test (SSI-ICM) (24) and two dichotic tests involving speech: the Dichotic Sentence Identification test (DST) (25) and the Dichotic Digits Test (DDT) (26). The sequence of test presentation was randomized to prevent an order effect.
MRI Acquisition
Imaging was performed in the sagittal plane on Siemens Trio 3T MRI Scanner with Siemens 32 channel head coil. Structural imaging consisted of MP2RAGE sequence (TR = 5 s, TE = 2.91 ms, TI = 700 ms, GRAPPA acceleration factor = 2, 1 x 1 x 1 mm resolution). Functional imaging consisted of one task fMRI sequence (8 minutes duration) and 2 resting-state fMRI sequences (10 minutes duration each). Resting-state fMRI acquisitions were acquired with participants’ eyes open and instructions to “allow your mind to wander and let thoughts pass through your mind.” fMRI sequences were acquired using multiband acquisition (multiband factor = 8, TR = 800 ms, TE = 33 ms, 2 x 2 x 2 ms resolution).
Structural MRI Processing
The FreeSurfer imaging analysis environment (v6.0.0), which is documented and freely available for download (http://surfer.nmr.mgh.harvard.edu/), was used to process structural scan data to obtain subject-specific subcortical regions of interest given characteristic volume loss in dementia patients and risk of volume averaging with the ventricles using a voxelwise atlas-based approach to region selection (27). A detailed description of the FreeSurfer pipeline can be found on the FreeSurfer website.
fMRI Music Task
A passive listening task consisted of 24 blocks of 20 seconds each presented in random order with instructions to listen to the musical selections. 8 blocks each of the music selection presented forward, 8 blocks with the same selections presented in reverse, and 8 blocks of silence were presented. Four preferred musical selections were chosen from each subject’s favorite musical selections by a professional classical composer (KB) to include iconic clips of the selected music (as detailed above). Song clips and reversed selections were created using Logic Pro X software.
Activation maps for forward music > silence, reverse music > silence, and forward music > reverse music were obtained for each subject using a general linear model in the SPM12 software suite (Wellcome Trust, London) following postprocessing that included motion correction (realign: estimate and reslice), coregistration to MP2RAGE image (coregister: estimate), normalization to MNI space (normalize: estimate and reslice), and smoothing (FWHM: 6 mm kernel). Second level estimates were obtained across 17 subjects using 2-direction t-tests for each of the three selected contrasts. Statistical significance was assessed using cluster-defining threshold of p<0.001 with familywise error corrected cluster-level significance to account for multiple comparisons.
Resting-state fMRI Processing
A postprocessing pipeline was selected to optimize correction for head motion and physiological artifacts, and physiological waveforms from heart rate and respiration were explicitly recorded for each subject during each resting state acquisition to use as regressors. Motion correction, coregistration, segmentation, and normalization of MP2RAGE and BOLD to MNI template was performed in SPM12 software (Wellcome Trust, London) for MATLAB (Mathworks, Natick MA). Phase-shifted soft tissue correction (28) was used to regress physiological waveforms as well as regressors obtained from 6 detrended subject motion parameters, degraded white matter, degraded cerebrospinal fluid, and soft tissues of the face and calvarium. Censoring of frames showing greater than 0.2 mm (motion scrubbing) was performed as a final step prior to analysis with concatenation of remaining frames (29). No significant differences were seen in root-mean-square head motion between initial and final resting state acquisitions for each subject using paired t-test across subjects.
Region of Interest Selection
Resting-state fMRI data were analyzed using brain parcellations at 2 levels of granularity. Average time series were extracted from each of 7 distributed brain networks associated with the cortical parcellation of Yeo et al. (30) and cerebellar parcellation of Buckner et al. (31). Cerebellar time series were extracted from left-lateralized and right-lateralized voxels in each of the 7 networks. Each network was treated as a single region of interest, and BOLD time series was averaged across all voxels for each of the 7 networks for each of the 740 volumes in each of the 2 runs for each subject after excluding the first 20 volumes of each run.
A finer parcellation consisted of 333 regions in the cerebral cortex (32). Fourteen subject-specific subcortical regions were added using FreeSurfer-derived segmentation (33) of bilateral thalamus, caudate, putamen, amygdala, hippocampus, pallidum, and nucleus accumbens, segmented independently for each subject. Fourteen cerebellar regions were also added (31) comprising left- and right-hemispheric representations of a 7-network parcellation. This combined parcellation scheme covering cortex, subcortical structures, and the cerebellum comprised a total of 361 regions. Average BOLD time series were extracted for each volume in each run for each subject.
Results
Auditory Testing Results
The average pure tone thresholds for the right and left ears were 24.9dB and 24.6dB, respectively, indicating normal peripheral hearing (average <25dB or the volume of a whispered voice). Average dichotic sentence scores for the right and left ears were 91% and 45%, respectively. Average dichotic digit scores for the right and left ears were 94% and 90%, respectively. Average Synthetic Sentence Identification test results with a 20dB, 0dB, and -20dB signal-to-noise ratio were 91%, 71%, and 40%, respectively.
Imaging Results
Participants listened to favorite musical selections, personalized for each individual, compared to the same selections played in reverse. When selections were played in reverse, auditory content was preserved while iconic motifs, language, and familiarity of the music was disrupted. Functional activation associated with forward and reversed musical stimuli is shown in Figure 1. Both forward and reverse musical stimuli elicited activation within bilateral auditory cortex and areas of left lateral frontal lobe, and cerebellum. There was specific activation seen in the bilateral, left greater than right, supplementary motor area for musical stimuli played forward, with a significant cluster for forward vs. reverse stimuli. Details of activated regions are displayed in Table 1.
To evaluate functional connectivity before and after the music task, we performed 10-minute resting-state fMRI acqisitions and calculated functional connectivity between mean time series of 7 brain networks from a previously published parcellation of the cerebral cortex (30) and cerebellum (31). The cerebellar time courses were calculated separately for left and right cerebellar hemispheres. Mean functional connectivity for each pair of cortical and cerebellar network time series was calculated as the correlation coefficient between the time series. A paired t-test across subjects was performed to identify network functional connectivity that differed significantly after the music task compared to before the music task, with results shown in Figure 2.
Significantly higher functional connectivity was observed after the music task for the visual network compared to somatomotor, salience, and executive networks, and for numerous cerebellar and corticocerebellar network pairs as shown. All results were corrected for multiple comparison corrections using false discovery rate approach. No network pairs showed significantly decreased functional connectivity after the music task.

Response to Favorite Music. Images show significant activation across participants to preferred musical selections played forward and in reverse greater than to blocks of silence (above), and to forward greater than reversed musical selctions (below). Results were cluster corrected using family-wise error, with display threshold set at p<0.001
To evaluate at a finer spatial distribution changes in functional connectivity, we computed time courses for 361 regions comprised of a 333-region functional brain parcellation of the cerebral cortex (32), 14 subcortical regions derived from subject-specific FreeSurfer segmentation, and the 14 cerebellar regions from the Buckner et al. parcellation shown in Figure 2 (31). Results for comparison of functional connectivity after vs. before the music test show in Figure 3 that for almost all brain region pairs functional connectivity after the music task was equal to or higher than before the task. While no individual connections were significant following full multiple comparison correction across all 361 x 361 region pairs given the modest sample size, the mean functional connectivity averaged across all region pairs was higher after the task compared to before (p=0.0167, paired t-test over 17 subjects).

Changes in functional connectivity after listening to preferred music. Colored squares show functional connections between 7 cortical networks and corresponding networks within the left and right cerebellum that showed greater connectivity after musical task than before, corrected by false discovery rate <0.05 across all connections. Color scale shows t-statistic from bidirectional paired t-test across 17 subjects
Discussion
In a cohort of patients with Alzheimer disease related dementia, we find that listening to preferred musical selections is specifically associated with activation of the supplementary motor area when compared with the same selections played in reverse such that passages were not clearly recognizable. After a period in which favorite musical selections were played, there were widespread increases in fMRI connectivity involving both corticocortical and corticocerebellar connections, particularly involving sensory and attentional networks.
These findings directly support previous research identifying the supplementary motor area as a region associated with selective activation to more familiar musical stimuli (34, 35). This region, in addition to the anterior insula that was also more active for familiar music, may play an important role in the preservation of musical memory in Alzheimer disease related dementia given that these areas tend to be relatively spared from neurodegenerative processes in the disease (34). Recognition of famous musical passages has also been associated with preservation of brain tissue in the anterior temporal lobes in Alzheimer and semantic dementias (36).

Changes in functional connectivity after listening to preferred music. Results from connections between 361 x 361 gray matter regions of interest, grouped by functional network. Warm colors represent greater connectivity after the music task and cool colors represent greater connectivity before the music task
The dorsal anterior cingulate, supplementary motor area, and frontal insula comprise a brain network known to process stimulus salience across multiple sensory and cognitive domains, and form a core part of the brain’s ventral attention network engaged in response to novel or unexpected stimuli (37). The specific activation of the supplementary motor area for favorite musical selections may suggest an attentional mechanism for symptomatic improvements associated with music listening whereby preferred musical selections evoke brain attentional responses, at least for a window time following the musical stimuli.
The brain’s salience network is closely associated with reward circuits in the ventral striatum, also known to play a key role in both salience processing and music appreciation. Activation of dopaminergic pathways in the ventral striatum is associated both with salience and valence of sensory stimuli (38), with dopamine signaling salience of rewarding stimuli (39). Selective activation of the ventral striatum has been associated with responses to musical stimuli evoking emotional chills (40), and specific activation of the dopaminergic striatum has been demonstrated in response to favorite music (22).
Widespread decreases in functional connectivity have been observed in Alzheimer disease related dementia, with earliest involvement of the brain’s default network (41-46). In contrast, the brain’s salience network is relatively preserved until late in Alzheimer disease and given the specific ability of familiar music to engage these circuits (34) may facilitate attention, reward, and motivation associated with the salience and mesolimbic networks (47).
Increased functional connectivity in our results associated with a personalized musical intervention suggests recruitment of brain networks that were highest among sensory regions and corticocerebellar circuits. Given that Alzheimer disease related dementia is typically associated with decreased functional connectivity (48), it is plausible that symptomatic relief observed after musical interventions may be related to such connectivity increases that occur in the context of apathetic and amotivational states observed in dementia. Anecdotal evidence from observation of music listening programs has highlighted precisely this type of “awakening” associated with musical interventions (49).
It remains unclear from our results the duration and generalizability of the effect on brain connectivity and attentional activation seen in our results. We studied only a single imaging session, and while participants had been trained for a period of weeks on a music-listening program, it is unknown whether such training was required to see an effect, whether such an effect persists beyond a brief period following stimulation, or whether other functional domains such as memory or mood may be enhanced by the specific changes in neural activation and connectivity in our results. Given the modest sample size in our study and known heterogeneity of symptoms in patients with early Alzheimer Disease, these results serve primarily a heuristic value in suggesting mechanisms for neurophysiological effects that can be tested in clinical trials with larger sample sizes and control of additional variables such as psychiatric comorbidities, personal musical history, environmental support, and pharmacotherapy. Further, while we do observe widespread increases in functional connectivity following music listening, our study is not powered to specifically identify which brain networks are primarily affected.
Nevertheless, we find support for an effect in Alzheimer patients for personalized music interventions that utilize favorite musical selections of individuals to promote improved attention and function consistent with the empirical benefits seen in clinical practice (15). Given the potential benefit of adjunctive therapies such as personalized music intervention, particularly given the low cost, few reported adverse side effects, and wide potential availability of these interventions in a large and growing patient group with enormous social cost and personal impact, continued evaluation of mechanisms and potential applications of personalized music programs and music therapy is warranted.
Acknowledgments: All authors report no competing interests.
Funding: This work was supported by grants from A. Scott Anderson and the American Otological Society.
Ethical standard: All experimental procedures were performed following informed consent for research participants in accordance with protocols approved by the University of Utah Institutional Review Board and the Code of Ethics of the World Medical Association for protection of human subjects in scientific research.
References
Gerdner LA. Individualized music intervention protocol. J Gerontol Nurs. 1999;25:10–6.
Gerdner LA, Schoenfelder DP. Evidence-based guideline. Individualized music for elders with dementia. J Gerontol Nurs. 2010;36:7–15.
Gerdner LA. Effects of individualized versus classical «relaxation» music on the frequency of agitation in elderly persons with Alzheimer’s disease and related disorders. Int Psychogeriatr. 2000;12:49–65.
Sakamoto M, Ando H, Tsutou A. Comparing the effects of different individualized music interventions for elderly individuals with severe dementia. Int Psychogeriatr. 2013;25:775–84.
Cooke M, Moyle W, Shum D, Harrison S, Murfield J. A randomized controlled trial exploring the effect of music on quality of life and depression in older people with dementia. J Health Psychol. 2010;15:765–76.
Guetin S, Portet F, Picot MC, Pommie C, Messaoudi M, Djabelkir L, et al. Effect of music therapy on anxiety and depression in patients with Alzheimer’s type dementia: randomised, controlled study. Dement Geriatr Cogn Disord. 2009;28:36–46.
Gallego MG, Garcia JG. Music therapy and Alzheimer’s disease: Cognitive, psychological, and behavioral effects. Neurologia. 2017;32:300–8.
Sung HC, Chang AM, Lee WL. A preferred music listening intervention to reduce anxiety in older adults with dementia in nursing homes. J Clin Nurs. 2010;19:1056–64.
Ueda T, Suzukamo Y, Sato M, Izumi S. Effects of music therapy on behavioral and psychological symptoms of dementia: a systematic review and metaanalysis. Ageing Res Rev. 2013;12:628–41.
Ridder HM, Stige B, Qvale LG, Gold C. Individual music therapy for agitation in dementia: an exploratory randomized controlled trial. Aging Ment Health. 2013;17:667–78.
Sung HC, Chang AM. Use of preferred music to decrease agitated behaviours in older people with dementia: a review of the literature. J Clin Nurs. 2005;14:1133–40.
Raglio A, Bellelli G, Traficante D, Gianotti M, Ubezio MC, Villani D, et al. Efficacy of music therapy in the treatment of behavioral and psychiatric symptoms of dementia. Alzheimer Dis Assoc Disord. 2008;22:158–62.
Raglio A, Bellandi D, Baiardi P, Gianotti M, Ubezio MC, Zanacchi E, et al. Effect of Active Music Therapy and Individualized Listening to Music on Dementia: A Multicenter Randomized Controlled Trial. J Am Geriatr Soc. 2015;63:1534–9.
van der Steen JT, van Soest-Poortvliet MC, van der Wouden JC, Bruinsma MS, Scholten RJ, Vink AC. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst Rev. 2017;5:CD003477.
Thomas KS, Baier R, Kosar C, Ogarek J, Trepman A, Mor V. Individualized Music Program is Associated with Improved Outcomes for U.S. Nursing Home Residents with Dementia. Am J Geriatr Psychiatry. 2017;25:931–8.
Cuddy LL, Duffin J. Music, memory, and Alzheimer’s disease: is music recognition spared in dementia, and how can it be assessed? Med Hypotheses. 2005;64:229–35.
Samson S, Dellacherie D, Platel H. Emotional power of music in patients with memory disorders: clinical implications of cognitive neuroscience. Ann N Y Acad Sci. 2009;1169:245–55.
Janata P. The neural architecture of music-evoked autobiographical memories. Cereb Cortex. 2009;19:2579–94.
Pereira CS, Teixeira J, Figueiredo P, Xavier J, Castro SL, Brattico E. Music and emotions in the brain: familiarity matters. PLoS One. 2011;6:e27241.
Eschrich S, Munte TF, Altenmuller EO. Unforgettable film music: the role of emotion in episodic long-term memory for music. BMC Neurosci. 2008;9:48.
Hall GR, Buckwalter KC. Progressively lowered stress threshold: a conceptual model for care of adults with Alzheimer’s disease. Arch Psychiatr Nurs. 1987;1:399–406.
Salimpoor VN, Benovoy M, Larcher K, Dagher A, Zatorre RJ. Anatomically distinct dopamine release during anticipation and experience of peak emotion to music. Nature neuroscience. 2011;14:257–62.
Gates GA, Anderson ML, Feeney MP, McCurry SM, Larson EB. Central auditory dysfunction in older persons with memory impairment or Alzheimer dementia. Arch Otolaryngol Head Neck Surg. 2008;134:771–7.
Jerger J, Hayes D. Diagnostic speech audiometry. Arch Otolaryngol. 1977;103:216–22.
Fifer RC, Jerger JF, Berlin CI, Tobey EA, Campbell JC. Development of a dichotic sentence identification test for hearing-impaired adults. Ear Hear. 1983;4:300–5.
Musiek FE, Gollegly KM, Kibbe KS, Verkest-Lenz SB. Proposed screening test for central auditory disorders: follow-up on the dichotic digits test. Am J Otol. 1991;12:109–13.
Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage. 1999;9:179–94.
Anderson JS, Druzgal TJ, Lopez-Larson M, Jeong EK, Desai K, Yurgelun-Todd D. Network anticorrelations, global regression, and phase-shifted soft tissue correction. Hum Brain Mapp. 2011;32:919–34.
Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage. 2012;59:2142–54.
Yeo BT, Krienen FM, Sepulcre J, Sabuncu MR, Lashkari D, Hollinshead M, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106:1125–65.
Buckner RL, Krienen FM, Castellanos A, Diaz JC, Yeo BT. The organization of the human cerebellum estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106:2322–45.
Gordon EM, Laumann TO, Adeyemo B, Huckins JF, Kelley WM, Petersen SE. Generation and Evaluation of a Cortical Area Parcellation from Resting-State Correlations. Cereb Cortex. 2016;26:288–303.
Fischl B, Salat DH, Busa E, Albert M, Dieterich M, Haselgrove C, et al. Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron. 2002;33:341–55.
Jacobsen JH, Stelzer J, Fritz TH, Chetelat G, La Joie R, Turner R. Why musical memory can be preserved in advanced Alzheimer’s disease. Brain. 2015;138:2438–50.
Groussard M, La Joie R, Rauchs G, Landeau B, Chetelat G, Viader F, et al. When music and long-term memory interact: effects of musical expertise on functional and structural plasticity in the hippocampus. PLoS One. 2010;5.
Hsieh S, Hornberger M, Piguet O, Hodges JR. Neural basis of music knowledge: evidence from the dementias. Brain. 2011;134:2523–34.
Seeley WW, Menon V, Schatzberg AF, Keller J, Glover GH, Kenna H, et al. Dissociable intrinsic connectivity networks for salience processing and executive control. J Neurosci. 2007;27:2349–56.
Cooper JC, Knutson B. Valence and salience contribute to nucleus accumbens activation. Neuroimage. 2008;39:538–47.
Berridge KC, Robinson TE. What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience? Brain Res Brain Res Rev. 1998;28:309–69.
Salimpoor VN, van den Bosch I, Kovacevic N, McIntosh AR, Dagher A, Zatorre RJ. Interactions between the nucleus accumbens and auditory cortices predict music reward value. Science. 2013;340:216–9.
Greicius MD, Srivastava G, Reiss AL, Menon V. Default-mode network activity distinguishes Alzheimer’s disease from healthy aging: evidence from functional MRI. Proc Natl Acad Sci U S A. 2004;101:4637–42.
Adriaanse SM, Binnewijzend MA, Ossenkoppele R, Tijms BM, van der Flier WM, Koene T, et al. Widespread disruption of functional brain organization in early-onset Alzheimer’s disease. PLoS One. 2014;9:e102995.
Adriaanse SM, Sanz-Arigita EJ, Binnewijzend MA, Ossenkoppele R, Tolboom N, van Assema DM, et al. Amyloid and its association with default network integrity in Alzheimer’s disease. Hum Brain Mapp. 2014;35:779–91.
Rombouts SA, Damoiseaux JS, Goekoop R, Barkhof F, Scheltens P, Smith SM, et al. Model-free group analysis shows altered BOLD FMRI networks in dementia. Hum Brain Mapp. 2009;30:256–66.
Song J, Qin W, Liu Y, Duan Y, Liu J, He X, et al. Aberrant functional organization within and between resting-state networks in AD. PLoS One. 2013;8:e63727.
Wang L, Zang Y, He Y, Liang M, Zhang X, Tian L, et al. Changes in hippocampal connectivity in the early stages of Alzheimer’s disease: evidence from resting state fMRI. Neuroimage. 2006;31:496–504.
Bromberg-Martin ES, Matsumoto M, Hikosaka O. Dopamine in motivational control: rewarding, aversive, and alerting. Neuron. 2010;68:815–34.
Sheline YI, Raichle ME. Resting state functional connectivity in preclinical Alzheimer’s disease. Biol Psychiatry. 2013;74:340–7.
Rossato-Bennett M. Alive Inside. Projector Media; 2014.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
King, J.B., Jones, K.G., Goldberg, E. et al. Increased Functional Connectivity After Listening to Favored Music in Adults With Alzheimer Dementia. J Prev Alzheimers Dis 6, 56–62 (2019). https://doi.org/10.14283/jpad.2018.19
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14283/jpad.2018.19