
Abstract
Background
Several indexes based on clinical and laboratory tests to identify frailty and to predict mortality have been produced. Only two studies, mixing clinical and laboratory parameters were made about a frailty index made of laboratory tests (FI-Lab) and mortality in older patients hospitalized for COVID-19. The aim of this study was to explore the accuracy and precision of an FI-Lab constructed with some common bio-humoral tests and mortality in a cohort of patients hospitalized for COVID-19.
Methods
The FI-Lab was constructed using 40 different biohumoral tests during the first four days of hospitalization, with a score from 0 to 1. The association between FI-Lab and mortality was assessed using a multivariate Cox’s regression analysis, reported as hazard ratios (HRs) and 95% confidence intervals (CIs). The accuracy of the FI-Lab was reported as area under the curve (AUC) and the precision with the C-Index.
Results
376 patients (mean age: 65 years; 53.7% males) were initially included. During the follow-up period, 41 deceased. After adjusting for five different factors, an FI-Lab value >0.54, the median value of our cohort, was associated with a relative risk about five times greater than lower values. Modeling FI-LAB as a continous variable, each increase in 0.01 points was associated with an increased risk in mortality of 8.4% (HR=1.084; 95%CI: 1.039–2.044). The FI-Lab was highly accurate (AUC=0.91; 95%CI: 0.87–0.95) and precise (C-Index=0.81) in predicting death.
Conclusions
A simple index based on common laboratory tests can be used to predict mortality among older people hospitalized for COVID-19.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the evaluation of frailty, several models are proposed. Among the most known and used, the frailty index (FI) is based on a series of deficits accumulation (1). Briefly, FI is based on various clinical health measures across physiological systems, usually as yes or no conditions, which are then summed and divided by the total number of assessments made (1). The resultant FI score is a parameter that reflects the state of an individual’s health, with a particular focus on comorbidities (2). In this way, the FI reduces dozens of dimensions typical of older people into a single score ranging from 0 to 1, higher scores reflecting a higher presence of deficits and, therefore, higher risk of death and other negative outcomes (2).
Recently, some authors have proposed an FI constructed using laboratory data (FI-Lab). This tool employs laboratory data to substitute or to complement the count of deficits (3,4). The literature supporting the use of the FI-Lab indicates that laboratory derived components are better than the original FI based on clinical parameters, since FI-Lab is more objective (5). The first FI-Lab was developed in an animal model (6). About ten years ago, some authors developed the first formal FI-Lab in humans (4). After that, several other works have proposed and confirmed its utility in clinical practice, across different settings and situations (5). One important point is that the FI-Lab can be calculated easily since its components can be obtained from commonly measured hospital tests (5). Consequently, operationalizing standard laboratory data into an FI-Lab could be an easy and accessible way to assess frailty in a clinical setting, such as hospital, making this instrument ideal for the early detection and screening of frailty (7).
A recent systematic review with meta-analysis found that in 38 different studies, from community to hospital setting, higher FI-Lab scores were associated with a higher mortality risk and with a variety of adverse health outcomes (5). However, to the best of our knowledge limited literature explored the use of FI-Lab in older patients affected by COVID-19, overall finding that higher FI-Lab values were associated with unfavourable outcomes, also after adjusting for potential confounders (8,9). In our opinion, to confirm or not the validity, accuracy and precision of Fi-Lab in older patients affected by COVID-19 is of importance since this condition, despite an important vaccination campaign is still present and associated with a high mortality rate in older people as well as to a higher risk of hospitalization and poor quality of life (10), making this population different from those analyzed so far.
Given this background, the aim of this study was to explore the accuracy and precision of an Fi-Lab constructed with some bio-humoral tests commonly available and mortality in a cohort of patients hospitalized for COVID-19 in Palermo, Italy.
Materials and methods
Study Population
From 1 September 2020 to 30 April 2021, all patients aged 18 years or older were enrolled at the Department of Internal Medicine and/or Geriatrics of the PO «Policlinico Paolo Giaccone» in Palermo, with a diagnosis of SARS-CoV-2 infection confirmed by the observation of SARS-CoV-2 nucleic acid on a nasopharyngeal swab by RT-PCR and with radiological evidence of pneumonia (11).
No other inclusion criteria were considered to better represent a real-life scenario. The study was approved by the Local Ethics Committee at its meeting on 28 April 2021 (protocol number 04/2021). At the time of hospital admission, no patients were vaccinated against COVID-19. For hygienical reasons, informed consent to participate in the study was collected orally and reported in the medical record.
Exposure: construction of the Fl-Lab
The FI-Lab was built on 40 different laboratory values, collected in the first four days of hospitalization, which included blood count, liver function, renal function, pancreatic function, blood glucose and lipid profile, serum electrolytes, coagulation parameters, inflammatory parameters, blood gas analysis parameters, serum vitamin D values, cardiovascular profile parameters (troponin, proBNP), thyroid profile. The entire list of the factors considered is reported in Supplementary Table 1. For each parameter, a value of 0 was given if the subject had normal values and 1, if abnormal. We then added up the number of abnormalities and divided by the number of exams available for a subject with a final score with a value between 0 and 1, higher values corresponding to a higher number of abnormalities. No imputation methods were used and we only excluded patients having less than ten bio-humoral tests available.
Outcome: mortality
Mortality was recorded through the medical documentation available in the medical records and through death certificates. The follow-up was the length of stay in hospital that, in our cohort, was in median nine days.
Covariates
In addition to demographics (age and gender), we have introduced as factors in multivariate analyses:
-
The Cumulative Illness Rating Scale (CIRS): it is an index designed to assess the severity of a patient’s comorbidities. The scale format consists of 13 relatively independent areas grouped by apparatus. Ratings are made on a 5-point «degree of severity» scale, ranging from «none» to «extremely severe» (12). As a rapid, objective, and easily quantifiable evaluation technique, the scale is well suited to a variety of research uses;
-
The Pneumonia Severity Index (PSI) score was used to identify the mortality risk of patients with radiological evidence of pneumonia enrolled in the study (13). The PSI was derived and validated as part of the prospective Pneumonia Patient Outcomes Research Team cohort study to identify patients with community acquired pneumonia, at low risk of mortality. PSI stratified adults with radiographic evidence of pneumonia into five risk classes for all-cause death within 30 days of presentation. Predictive variables were derived from medical history, physical examination, and selected laboratory and radiographic results readily available at the time of patient presentation.
-
Typical COVID symptoms: Typical signs and symptoms of COVID such as anorexia, anosmia, fever, gastrointestinal symptoms etc. have been included (14).
Statistical analysis
Patients were divided according to survival status during their hospital stay. Values for continuous variables were reported as means and standard deviations (SD) or as absolute and relative frequencies (in %) in the two groups. The normality of the continuous variables was assessed using the Kolgomorov-Smirnov test. Continuous variables were compared between the two groups using the Student’s T-test for independent samples and categorical variables were compared with the Chi-Square test, using Fisher’s correction where necessary.
The association between the FI-Lab and in-hospital mortality was analyzed using Cox regression, adjusted for potential confounders. Factors were included in the multivariate analysis as they were statistically different between patients with a p-value below 0.05 or associated with the outcome of interest with a p< 0.10. The results were then reported as hazard ratio (HR) and 95% confidence intervals (95%CI). We considered as statistically significant the results with a p-value below 0.05. Since no univocal cut-off was available for the FI-Lab, we used the median value of 0.54 for the main analysis. We have then modeled the FI-Lab score as increase in 0.01 points. To test the robustness of our results, we did run some sensitivity analyses (age less or more than 65 years, gender). Finally, we performed an analysis of the accuracy of the FI-Lab, added to age and gender, in predicting mortality, reporting the data as area under the curve (AUC) and its 95% CI. Similarly, we have calculated the Harrell’s C Index which summarises how well a predicted risk score describes an observed sequence of events in survival analyses (precision).
All analyses were performed using the SPSS 26.0 for Windows (SPSS Inc., Chicago, Illinois). All statistical tests were two-tailed and statistical significance was assumed for a p-value <0.05.
Results
Initially, in the COMEPA study, 430 patients were hospitalized. We excluded 40 patients since no sufficient data to create the FI-Lab were available and 14 patients who were lost during the follow-up. Therefore, 376 patients were finally included in this analysis. This sample size aged a mean of 65±17 years and were prevalently males (53.7%). The most common bio-humoral alteration was the presence of abnormal lymphocites (73.9%). The 186 males reported significantly higher FI-Lab scores than females (mean difference=0.03±0.01; p=0.002).
Table 1 shows the baseline data of the included patients, by their baseline value of the FI-Lab. The patients with a FI-Lab >0.54 were significantly older than those reporting scores lower than the median value (p<0.0001), whilst no differences emerged in terms of percentage of males. Moreover, patients with higher FI-Lab scores reported significantly higher PSI scores (p<0.0001) and lower diastolic blood pressure (p=0.001). As expected, patients with a FI-Lab >0.54 were affected by more medical conditions (p<0.0001) (Table 1).
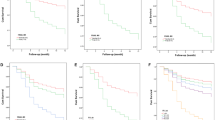
Table 2 shows the multivariate analysis of the factors that, at the univariate analyses, were associated with mortality. Overall, after adjusting for five different factors, an FI-Lab value >0.54 was associated with a relative risk about five times greater than lower values (HR=5.142; 95%CI: 2.092–12.641; p<0.0001) (Figure 1). Modeling FI-LAB as a continous variable, each increase in 0.01 points was associated with an increased risk in mortality of 8.4% (HR=1.084; 95%CI: 1.039–2.044; p<0.0001). In the multivariate analysis, both age and PSI, were significnatly associated with a higher risk of death: practically, for each additional year of age, mortality increased by 7% as well as an extra point at PSI increased the risk by 1% (Table 2).

Association between laboratory frailty index and survival in older patients hospitalized for COVID-19
Figure 2 shows the accuracy of the FI-Lab in predicting mortality. It can be seen from the figure that the frailty index constructed with laboratory parameters was highly predictive of mortality being the AUC=0.91 (95%CI: 0.87-0.95, p<0.0001). The value of 0.54, which we chose for our analyses as cutoff value, had a good sensitivity of 81% and a fair specificity of 74%. The Harrell’s C-Index was 0.81, indicating a good precision of FI-Lab in predicting mortality.

Accuracy of the laboratory frailty index in predicting mortality
To test the robustness of our results, we did run some sensitivity analyses (age less or more than 65 years, gender), but the results were not significantly different across strata at a p-value of 0.05, since the p for interaction for age was 0.97 and for gender was 0.37.
Discussion
In our study, including 376 older patients hospitalized for COVID-19, we found that higher FI-Lab scores were associated with a higher risk of mortality, also taking in account several demographics and clinical factors and that this score was highly accurate and precise in predicting death. Our findings reinforce the idea that an FI-Lab, created using simple bio-humoral exams usually requested for clinical reasons, may increase our awareness in screening frailty in hospitalized older patients.
From a clinical perspective, the deficits investigated by the FI-Lab are probably easier to collect than those based on clinical assessments, since in several centers, bio-humoral tests are automatically available in medical records (15). This characteristic makes this tool ideal for a first screening of frailty, particularly in the case of large number of patients and when time is limited (16). At the same time, standard laboratory tests can be core measures used to create an FI-Lab, which may make available routinely collected data (4).
In the literature available so far, only two studies investigated the possible role of FI-Lab in COVID-19, among older people. The first one included 615 older patients across seven Veterans Health Administration medical centers in Florida and Puerto Rico, overall finding that one FI-Lab made of thirteen components of a complete blood count analysis, thirteen elements of a comprehensive metabolic profile, and five vital signs was strongly associated with mortality and longer hospital stay (8). The second one includes only nine laboratory measures over 48 possible deficits considered again finding that this FI-Lab was highly predictive of mortality across different timepoints (10). Even if these works were of importance, we believe that our works was different and novel for several reasons. First, our FI-Lab was made only of laboratory measures and not clinical parameters as the previous two. Second, we also considered blood tests commonly used not only in COVID-19, but also in other respiratory diseases, such as arterial blood gas parameters. In this sense, it is hardly surprising that we found a median FI-Lab of 0.54 vs. a median value of 0.18 as indicated in Mak et al. (9), mostly motivated by the fact that we considered only laboratory indicators including those commonly altered in COVID-19 such as blood gas and inflammatory parameters.
In a previous meta-analysis including 38 observational studies, the authors found that a small increase in FI-Lab was associated with an important increase in mortality risk of 4% (5), whilst in our work each increase in 0.01 points corresponded to an increase in mortality of 8%. Other than the number and type of covariates included, we can hypothesize that some factors typically altered in COVID-19, such as blood gas parameters, have better defined our tool compared to the previous literature. It is noteworthy that, despite the methodological differences that must be taken in consideration, the effect size that we reported is similar to that found using a clinical FI score (17). Moreover, as novel finding, we also propose that FI-Lab is an extremely accurate way to predict mortality in our cohort: the AUC of this tool, in fact, is 0.91, indicating that this tool has appropriate characteristics to screen patients at higher mortality risk, i.e., frail patients.
Another important point to discuss is that the association between higher FI-Lab scores and mortality was not affected by age or by gender, confirming previous literature about this topic. For example, a large study made in the NHANES context and including 8088 participants showed that FI-Lab is not as strong predictor of mortality in younger adults compared to older adults, even if as proposed by the same authors the mortality rate in younger people is probably too low and, therefore, future research should explore the possible association between FI-Lab with other negative outcomes in younger people (18). About the possible gender differences, we found that in men the FI-Lab was significantly higher than in women, but no effect on mortality was found by gender. Our finding is similar to that present in literature since in the meta-analysis cited before 3/11 studies that evaluated sex differences concluded that men have higher FI-Lab scores than women, while 2 found the opposite and another 5 found no difference (5). In our opinion, to include sex-hormones in the alterations included in the FI-Lab could better refine the question if any gender differences exist for the association between FI-Lab and mortality.
The findings of our work must be interpreted within its limitations. First, we included only patients affected by COVID-19 that may represent a selection bias in our findings since these patients, particularly during some periods, were clinically unstable. Therefore, it could be problematic to generalize our data in other cohorts. Second, we did not include any estimate of frailty, from a clinical point of view, including the social determinants of health that are part of frailty (19). Unfortunately, our study collected data during the first waves of COVID-19 and some procedures routinely done in our center; however, the evaluation of frailty was not performed. Third, we evaluated our FI-Lab only at the baseline, without considering the inherent changes of the bio-humoral parameters during the in-hospital stay.
In conclusion, our study suggests that a simple index based on common laboratory tests can be used to predict mortality among older people hospitalized for COVID-19. Our findings indicate that FI-Lab might be an easily applicable and accurate screening instrument in clinical settings.
Key summary points
Aim: to explore the accuracy and precision of an FI-Lab constructed with some bio-humoral tests commonly available and mortality in a cohort of patients hospitalized for COVID-19.
Findings: The FI-Lab was highly accurate and precise in predicting mortality in older people affected by COVID-19.
Message: A simple index based on common laboratory tests can be used to predict mortality among older people hospitalized for COVID-19.
References
Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC geriatrics. 2008;8(1):1–10.
Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. A global clinical measure of fitness and frailty in elderly people. Cmaj. 2005;173(5):489–95.
Howlett SE, Rutenberg AD, Rockwood K. The degree of frailty as a translational measure of health in aging. Nature Aging. 2021;1(8):651–65.
Howlett SE, Rockwood MR, Mitnitski A, Rockwood K. Standard laboratory tests to identify older adults at increased risk of death. BMC medicine. 2014;12:1–8.
Sapp DG, Cormier BM, Rockwood K, Howlett SE, Heinze SS. The frailty index based on laboratory test data as a tool to investigate the impact of frailty on health outcomes: a systematic review and meta-analysis. Age and Ageing. 2023;52(1):afac309.
Parks RJ, Fares E, MacDonald JK, Ernst MC, Sinal CJ, Rockwood K, et al. A procedure for creating a frailty index based on deficit accumulation in aging mice. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences. 2012;67(3):217–27.
Rockwood K, McMillan M, Mitnitski A, Howlett SE. A frailty index based on common laboratory tests in comparison with a clinical frailty index for older adults in long-term care facilities. Journal of the American Medical Directors Association. 2015;16(10):842–7.
Resendes NM, Chada A, Torres-Morales A, Fernandez M, Diaz-Quiñones A, Gomez C, et al. Association between a Frailty Index from Common Laboratory Values and Vital Signs (FI-LAB) and Hospital and Post-Hospital Outcomes in Veterans with COVID-19 Infection. J Nutr Health Aging. 2023;27(2):89–95.
Mak JKL, Eriksdotter M, Annetorp M, Kuja-Halkola R, Kananen L, Boström AM, et al. Two Years with COVID-19: The Electronic Frailty Index Identifies High-Risk Patients in the Stockholm GeroCovid Study. Gerontology. 2023;69(4):396–405.
Wei SC, Freeman D, Himschoot A, Clarke KE, Van Dyke ME, Adjemian J, et al. Who Gets Sick From COVID-19? Sociodemographic Correlates of Severe Adult Health Outcomes During Alpha-and Delta-Variant Predominant Periods: September 2020–November 2021. The Journal of Infectious Diseases. 2024;229(1):122–32.
Barbagallo M, Citarrella R, Dominguez L, Giannitrapani L, Licata A, Mansueto P, et al. COMEPA (COVID-19 Medicina Policlinico Palermo): a study in hospitalized patients. Geriatric Care. 2021(7):9895–7.
Linn BS, Linn MW, Gurel L. Cumulative illness rating scale. Journal of the American Geriatrics Society. 1968;16(5):622–6.
Aujesky D, Fine MJ. The pneumonia severity index: a decade after the initial derivation and validation. Clinical infectious diseases. 2008;47(Supplement_3):S133–S9.
Burke RM, Killerby ME, Newton S, Ashworth CE, Berns AL, Brennan S, et al. Symptom profiles of a convenience sample of patients with COVID-19—United States, January–April 2020. Morbidity and Mortality Weekly Report. 2020;69(28):904.
Ellis HL, Wan B, Yeung M, Rather A, Mannan I, Bond C, et al. Complementing chronic frailty assessment at hospital admission with an electronic frailty index (FI-Laboratory) comprising routine blood test results. Cmaj. 2020;192(1):E3–E8.
Satake S, Arai H. Implications of frailty screening in clinical practice. Current Opinion in Clinical Nutrition and Metabolic Care. 2017;20(1):4–10.
Kojima G, Iliffe S, Walters K. Frailty index as a predictor of mortality: a systematic review and meta-analysis. Age and ageing. 2018;47(2):193–200.
Blodgett JM, Theou O, Howlett SE, Rockwood K. A frailty index from common clinical and laboratory tests predicts increased risk of death across the life course. Geroscience. 2017;39(4):447–55.
Ragusa FS, Veronese N, Smith L, Koyanagi A, Dominguez LJ, Barbagallo M. Social frailty increases the risk of all-cause mortality: a longitudinal analysis of the English longitudinal study of ageing. Experimental Gerontology. 2022:111901.
Funding
Funding: The costs of the publication are supported by the Premio Ferrante 2021, given to prof. Nicola Veronese.
Author information
Authors and Affiliations
Consortia
Contributions
Authors’ contribution: Vincenza Briganò, Stefano Ciriminna, Antonina Ganci, Federica Bifara, Francesco Pollicino, Maria Chiara Garlisi, Francesca Tantillo participated in data collection; Nicola Veronese, Laura Vernuccio, Giuseppina Rizzo drafted the first version of the paper. Nicola Veronese and Simona Amodeo participated in data analysis. Ligia Dominguez, Pasquale Mansueto, Anna Licata, Lydia Giannitrapani and Mario Barbagallo participated in revision of the paper. All authors saw and approved the final version and no other person made a substantial contribution to the paper..
Corresponding author
Ethics declarations
Conflict of interest: none.
Ethical standards: The study was approved by the Local Ethics Committee at its meeting on 28 April 2021 (protocol number 04/2021). Informed consent was obtained orally for hygienical reasons and reported in medical records.
Additional information
How to cite this article: N. Veronese, V. Briganò, S. Ciriminna, et al. Prognostic Value of a Laboratory Index of Frailty in Older Patients Hospitalized for COVID-19: The COMEPA Study. J Frailty Aging 2024; https://doi.org/10.14283/jfa.2024.29
The COMEPA study includes: Affronti Marco, Amodeo Simona, Barbagallo Mario, Briganò Vincenza Maria, Cacioppo Federica, Capitano Walter M., Carruba Luca, Cavaleri Francesco, Catanese Giuseppina, Citarrella Roberto, Di Bella Giovanna, Di Franco Giuseppina, Di Prazza Agnese, Dominguez Ligia Juliana, Giannitrapani Lydia, Licata Anna, La Carruba Anna, Mansueto Pasquale, Mirarchi Luigi, Morgante Maria Chiara, Parinello Alessandra, Pecoraro Emanuela, Peralta Marco, Piccione Ercole, Polizzotto Carla, Pollicino Francesco, Quartetti Federico, Randazzo Giusi, Rizzo Angelo, Rizzo Giuseppina, Sanfilippo Valeria, Soresi Maurizio, Malerba Valentina, Vernuccio Laura, Veronese Nicola, Zerbo Maddalena.
Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Veronese, N., Briganò, V., Ciriminna, S. et al. Prognostic Value of a Laboratory Index of Frailty in Older Patients Hospitalized for COVID-19: The COMEPA Study. J Frailty Aging 13, 213–217 (2024). https://doi.org/10.14283/jfa.2024.29
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14283/jfa.2024.29