
Abstract
Background
Using residual values calculated from models regressing appendicular lean mass on fat mass and height is one of several suggested strategies for adjusting appendicular lean mass for body size when measuring sarcopenia. However, special consideration is required when using this technique in different subgroups in order to capture the correct individuals as sarcopenic.
Objectives
To provide guidance about how to conduct stratified analyses for the regression adjustment technique using age groups as an example.
Design
Cross-sectional study.
Setting
Data collected at baseline (2012–2015) for the Canadian Longitudinal Study on Aging.
Participants
Community dwelling participants of European descent aged 45 to 85 years (n=25,399).
Measurements
Appendicular lean mass, height, and weight were measured. Sex-specific residuals were calculated in participants before and after stratifying participants by age group (45–54, 55–64, 65–74, 75–85 years). Cut offs corresponding to the sex-specific 20th percentile residual values in participants ≥65 years were determined first in the residuals calculated in all participants and residuals calculated in only those aged ≥65 years. For each set of cut offs, the percentage of age and sex-stratified participants with low appendicular lean mass were compared for the residuals calculated in all participants and the residuals calculated after stratifying by age.
Results
In 12,622 males and 12,737 females, regardless of the cut off used, the percentage of participants with low appendicular lean mass decreased with age when residuals were calculated after age stratification. When the residuals were calculated in all participants, the percentage of participants with sarcopenia increased from the youngest to the oldest age groups.
Conclusions
Sex-specific residuals in all participants should be calculated prior to stratifying the sample by age group, or other stratification variables, for the purposes of developing appendicular lean mass cut offs or subgroup analyses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sarcopenia refers to the decline in muscle mass, muscle strength, and muscle function that occurs with age (1). It is associated with an increased risk of falls and fractures, activities of daily living limitations, and mortality (2–5). Given the profound individual and societal costs of sarcopenia, there has been substantial interest in finding ways to prevent and treat sarcopenia. However, the field of sarcopenia research has been hindered by the lack of a clear definition and standardized diagnostic criteria (6).
Four expert-group definitions for sarcopenia define sarcopenia as the combination of low muscle mass, typically measured as appendicular lean mass (ALM), with either low muscle strength or impaired physical performance (6–10). There is a consensus among the definitions that ALM should be adjusted for body size due to the strong correlation between ALM with height and weight, however there is little agreement about which measure of body size should be utilized (6, 11). Four techniques are recommended; dividing by height squared, body mass, body mass index (BMI), and regressing ALM on height and fat mass (6–10). Of these methods, regressing ALM on height and fat mass may most accurately identify individuals with low ALM as it adjusts for two measures of body size whereas the other techniques only adjust for one measure of body size (12). This technique involves creating a regression model (ALM = intercept + height (m2) + fat mass (kg)) in a sample of individuals. For each individual, a predicted value of ALM is calculated based on the regression equation. Subtracting the estimated value of ALM from the actual value of ALM for each person provides a residual value. Positive residual values indicate that the individual has more ALM than would be expected given their height and weight and negative residual values indicate the individual has less ALM than would be expected given their height and weight.
Unlike adjusting ALM by height, weight, or BMI which are done at the individual level and are not influenced by other participants, calculating residuals is dependent on the sample. For height, weight, and BMI adjustment, the adjusted values refer to the same amount of ALM relative to the anthropometric measure adjusted for regardless of the person or sample. In contrast, the residual value for each person is dependent on the regression equation which in turn is dependent on the distribution of the variables in the sample. Consequently, even if low ALM offs are developed in a random, population-based sample, they cannot be appropriately applied to another population unless the two samples have identical joint distributions of ALM, fat mass, and height. Due to the unavailability of cut offs, studies that have investigated sarcopenia using the residual adjustment technique have considered the lowest quintile of sex-specific residual values as sarcopenic (13–19). However, a consequence of using the lowest quintile is that sarcopenia prevalence is the same for all studies, regardless of age, which is problematic for a condition for which the prevalence increases with age. This poses additional challenges for studies with a wide range of ages which want to conduct age stratified analyses.
To our knowledge, there has not been any discussion in the literature about the implications of stratifying a sample by age when applying the residual technique. We aimed to provide the necessary guidance for how to handle age stratification when calculating residual values for ALM adjusted for height and fat mass.
Methods
Setting and study population
We used data from the Canadian Longitudinal Study on Aging (CLSA), a national longitudinal research platform. There were 51,338 participants aged 45 to 85 years recruited from the ten Canadian provinces at baseline. Participants had to be physically and cognitively able to participate on their own as well as not living in institutions such as long term care to be eligible for the study. The participants were recruited in to one of two cohorts, the Tracking cohort and the Comprehensive cohort. Participants from all ten provinces were randomly selected for the Tracking cohort (n=21,241) and were interviewed by telephone. The Comprehensive cohort participants (n=30,097) lived within 25–50kg of one of 11 Data Collection Sites located in seven provinces. The Comprehensive cohort participants were interviewed in-person and also completed in-depth physical assessments and provided blood and urine samples. Details on the study design have been described elsewhere (20). Only participants from the Comprehensive cohort (n=30,097) were included in these analyses as the physical assessment data was required. The sample was further limited to those identifying as European as ALM, muscle strength, and physical function have shown to vary by ethnicity (21–23). This project uses data collected at baseline (September 2011 to May 2015). Ethics approval was received by the Hamilton Research Ethics Board (#2686).
Clinical measurements
Trained research assistants collected data on height, weight, and muscle mass. Height was measured twice using a stadiometer and the mean value of the two measurements was used in the analyses. The Hologic Discovery ATM DXA machine was calibrated daily using a spine phantom, weekly using a whole body step phantom, and yearly using a gold standard phantom. DXA provides a valid measures of ALM and fat mass when compared to the gold standards of computerized tomography (CT) and magnetic resonance imaging (MRI) scans (24, 25).
All analyses were stratified by sex. We used multiple linear regression models with ALM as the dependent variable and height (m2) and fat mass (kg) as the independent variables to estimate the predicted value of ALM for each participant. The residual values were calculated as the predicted value of ALM subtracted from the actual value of ALM. To test the impact of age stratification on the residual values, we first calculated residuals based on the regression model including participants aged 45 to 85 years. We then calculated residuals based on regression models run separately for each age strata (45 to 54, 55 to 64, 65 to 74, and 75 to 85 years). We followed the EWGSOP recommendation of using the lowest sex-specific 20th percentile of residual values as the cut off for low ALM (7). We chose to limit the sample for calculating cut offs to participants ≥65 years based on guidance from the literature (7). To explore the impact of age stratification on the values of the residual cut offs, we determined the cut offs for the residuals in the model that included all participants aged 45 to 85 years, as well as for residual values based on a model that only included participants 65 years and older.
The cut-offs detertmined using the non-age stratified residuals and the residuals calculated in just participants aged ≥65 years were applied to the residuals calculated in the whole sample and the age-stratified residuals. Therefore, there were four different strategies used to identify participants: Strategy 1: all residuals calculated in all participant; Strategy 2: individual residuals calculated in all participants, cut offs developed in participants ≥65 years; Strategy 3: individual residuals calculated in specific age groups, cut offs developed in all participants; Strategy 4: individual residuals calculated in specific age groups, cut offs developed in participants ≥65 years.
Statistical anaylses
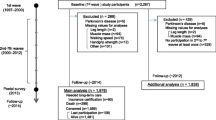
Of the 30,097 participants at baseline, 1324 were excluded as they were non-European, 3356 were excluded for missing ALM, grip strength, gait speed, or BMI data resulting in a final sample size of 25,399 participants. All statistical analyses were completed using SAS (version 12.3).
The percentage of age and sex-stratified participants categorized as having low ALM by each of the four strategies for handling age-stratification for the development of cut offs and individual residual values were determined. Bootstrap percentile confidence intervals were calculated for each estimate. This technique involves resampling with replacement and calculating the proportion of participants with sarcopenia for each resample (26). We resampled 10,000 times and identified the values corresponding to the 2.5th and 97.5th percentiles of the 10,000 resamples in order to estimate the 95% confidence interval. This technique has the advantage of only including valid values of parameter estimates in the confidence interval (26).
Results
Participant characteristics
The mean (SD) age of the participants was 62.8 (10.2) years and 49.9% of the sample were males (Table 1). Younger males and females had greater mean (SD) ALM: 27.2kg (4.2) and 17.9kg (3.4), grip strength: 47.3kg (9.1) and 28.6kg (5.6), and gait speed: 1.03m/s (0.18) and 1.02m/s (0.19) compared to older males and females (ALM: 24.4kg (3.7) and 16.3kg (2.9), grip strength: 39.4kg (8.5) and 23.6kg (5.2), and gait speed: 0.94m/s (0.19) and 0.90m/s (0.19).
Distribution of residuals
The overall distribution of the residual values was calculated in all participants versus calculating the residuals in age-stratified groups. In males, the mean (SD) for all participants was 0 (2.90), while the mean of the residuals for all age-stratified residuals pooled together was 0 (3.13). The corresponding values were 0 (2.08) and 0 (2.16) in females. However, the distribution of the data within each age group was markedly different. In both males and females, when the residuals were calculated after stratifying the sample by age, the residuals of each age group had a mean of 0. In contrast, when the residuals were calculated in the whole sample, there was a gradient of mean values when stratified by age group. The mean residual value for males 45 to 54 years was 1.36 and for females was 0.84 which decreased to -1.95 in males and -0.67 in females aged 75 to 85 years (Supplementary Appendix 1).
Muscle mass cut off estimates
The lowest 20th percentile cut offs corresponded to -3.51 for males and -2.15 for females when the residual values were calculated all participants, then restricted to participants aged ≥65 years. When the residuals were calculated in only participants ≥65 years, the 20th percentile cut offs were -2.23 for males and -1.58 for females.
Low muscle mass prevalence
The lower cut offs determined using the non-age stratified residual values of -3.51 for males and -2.23 for females identified fewer participants as having low muscle mass compared to the age-stratified residual values of -2.15 for males and -1.58 for females (Figure 1). For these cut offs, the prevalence of low muscle mass was 12.3% for males and 14.6% for females when the individual residuals were not age stratified (Strategy 1) and 10.3% for males and 13.8% for females when the individual residuals were age stratified (Strategy 3). The cut offs developed using residual values calculated in only participants >65 years, identified 23.8% of males and 22.8% of females as having low ALM when the non-age stratified residual values (Strategy 2) and 21.7% of males and 21.9% of females as having low ALM when the age-stratified values were used (Strategy 4).

Percentage of participants with low ALM adjusted for height and fat mass stratified by age group and sex
When looking at the percentage of people with low muscle mass within each age group, the percentage of males and females with low muscle mass increased with age when the individual residuals were not age-stratified, regardless of the cut offs used (Strategy 1 and Strategy 2). In contrast, the percentage of males and females with low muscle mass decreased with age when the age-stratified residuals were used (Strategy 3 and Strategy 4).
Discussion
To our knowledge, this is the first study to investigate the implications of age stratification when using the residual values for ALM after regressing on height and fat mass. We determined that residual values should be calculated in all participants before stratifying by age for the purposes of subgroup analyses or developing muscle mass cut offs (Strategy 1).
Stratifying the sample by age prior to calculating residuals for the purpose of subgroup analyses based on age or for developing cut offs proved problematic. When the sample was stratified by age before calculating the residuals (Strategy 3 and Strategy 4), the percentage of participants with low ALM decreased from the youngest to the oldest age groups (Figure 1) because of how the residuals are calculated. The maximum likelihood estimation technique used in linear regression to calculate the residuals requires that the sum of the residuals for the sample to equal zero. When the sample was stratified by age before calculating the residuals, the mean value of the residuals for each age group was zero. However, the standard deviation decreased with age (Supplementary Appendix 1). The greater the standard deviation for the age group, the more participants were below the low ALM cut off and therefore the higher the percentage of people with low ALM.
The problems we encountered stratifying our sample by age before calculating the residuals extend to any situation in which residuals calculated in one sample are combined or applied to another sample. Residual values are sample dependent and therefore unless two groups of participants have identical joint distributions of ALM, height, and fat mass, the residuals from one study will not identify people with the same amount of ALM relative to height and fat mass. This means that cut offs for the residual technique, even if developed in a population-based random sample with cut offs validated against relevant health outcomes, cannot be meaningfully applied to another sample. For this reason, in our analyses Strategy 1 which calculates the residuals in all participants before limiting to those ≥65 years to determine the lowest quintile is the appropriate strategy.
To resolve the issue of residual values and corresponding cut offs not being comparable between studies, prediction equations, similar to those that have been used for lung function can be developed (27). A sample of representative older adults could be used to create sex-specific prediction equations for ALM based on height and fat mass. Variables such as age, ethnicity, and other body composition variables could be explored for inclusion in the equation, as well as possible interactions between variables. These equations would allow for results to be meaningfully compared between studies and would also allow clinicians to use this technique to diagnose low ALM in individuals. Low ALM cut offs, ideally determined by assessing which cut offs best predict health outcomes relevant to sarcopenia, could be established and used differents studies.
To our knowledge, only one study has assessed the relationship between low ALM operationalized using the residual adjustment technique with health (12, 28). Cawthon et al. observed that low ALM adjusted for height and fat mass was significantly associated with risk of functional limitations and mortality, but not recurrent falls or hip fractures (12). Studies operationalizing sarcopenia as low ALM only often do not find significant associations with health, therefore the associations found with functional limitations and mortality are particularly notable (12, 29, 30). Given this evidence as well as the strong face validity for adjusting ALM simultaneously for height and fat mass, future studies are required to determine if adjusting ALM for height and fat mass, alone and in combination with muscle strength or function, better identifies people at poor risk for health compared to the other adjustment techniques.
In conclusion, adjusting ALM for height and fat mass using the regression technique is a promising method of operationalizing low ALM that warrants greater inclusion in future sarcopenia studies. In this study, we show that to appropriately apply the residual technique to a stratified sample, the regression equation must be calculated in all participants before stratifying the sample in order to identify the correct individuals as sarcopenic.
References
Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr 1997;127:990S–911S
Kim JH, Lim S, Choi SH, et al. Sarcopenia: an independent predictor of mortality in community-dwelling older Korean men. J Gerontol A Biol Sci Med Sci 2014;69:1244–1252
Landi F, Cruz-Jentoft AJ, Liperoti R, et al. Sarcopenia and mortality risk in frail older persons aged 80 years and older: results from ilSIRENTE study. Age Ageing 2013;42:203–209
Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairement and physical disability. J Am Geriatr Soc 2002;50:889–896
Yeung SSY, Reijnierse EM, Pham VK, et al. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J Cachexia Sarcopenia Muscle 2019;10:485–500
Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019;48:16–31
Cruz-Jentoft A, Baeyens J, Bauer J, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010;39:412–423
Studenski SA, Peters KW, Alley DE, et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. Journals Gerontol Med Sci 2014;69:547–558
Fielding RA, Vellas B, Evans WJ, et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and conseuqences. International Work Group on Sarcopenia. Am Med Dir Assoc 2011; 12:249–256
Chen L-K, Liu L-K, Woo J, et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc 2014; 15:95–101
Gallagher D, Visser M, De Meersman RE, et al. Appendicular skeletal muscle mass: effects of age, gender, and ethnicity. J Appl Physiol 2017;83:229–239
Cawthon PM, Blackwell TL, Francisco S, et al. An evaluation of the usefulness of consensus definitions of sarcopenia in older men: results from the observational Osteoporotic Fractures in Men (MrOS) cohort study. J Am Diet Assoc 2016;63:2247–2259
Menant JC, Weber F, Lo J, et al. Strength measures are better than muscle mass measures in predicting health-related outcomes in older people: time to abandon the term sarcopenia? Osteoporos Int 2016; 1–12
Delmonico MJ, Harris TB, Lee J-S, et al. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J Am Geriatr Soc 2007;55:769–774
Newman AB, Kupelian V, Visser M, et al. Sarcopenia: Alternative Definitions and Associations with Lower Extremity Function. J Am Geriatr Soc 2003;51:1602–1609
Figueiredo CP, Domiciano DS, Lopes JB, et al. Prevalence of sarcopenia and associated risk factors by two diagnostic criteria in community-dwelling older men: The São Paulo Ageing & Health Study (SPAH). Osteoporos Int 2014;25:589–596
Domiciano DS, Figueiredo CP, Lopes JB, et al. Discriminating sarcopenia in community-dwelling older women with high frequency of overweight/obesity: The São Paulo Ageing & Health Study (SPAH). Osteoporos Int 2013;24:595–603
Chalhoub D, Cawthon PM, Ensrud KE, et al. Risk of nonspine fractures in older adults with sarcopenia, low bone mass, or both. J Am Geriatr Soc 2015;63:1733–1740
Scott D, Chandrasekara SD, Lasiert LL, Cicuttini F, Ebeling PR, Jones G. Associations of sarcopenic obesity and dynapenic obesity with bone mineral density and incident fractures over 5–10 years in community-dwelling older adults. Calcif Tissue Int 2016;99:30–42
Raina PS, Wolfson C, Kirkland SA, et al. Cohort profile: The Canadian Longitudinal Study on Aging (CLSA). Can J Aging 2009;28:221–229
Capistrant BD, Glymour MM, Berkman LF. Assessing mobility difficulties for cross-national comparisons: Results from the World Health Organiation Study on Global AGEing and Adult Health. J Am Geriatr Soc 2015;62:329–335
Leong DP, Teo KK, Rangarajan S, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015;386:266–273
Silva AM, Shen W, Heo M, et al. Ethnicity-related skeletal muscle differences across the lifespan. Am J Hum Biol 2010;22:76–82
Buckinx F, Landi F, Cesari M, et al. Pitfalls in the measurement of muscle mass: a need for a reference standard. J Cachexia Sarcopenia Muscle 2018;9:269–278
Kullberg J, Brandberg J, Angelhed JE, et al. Whole-body adipose tissue analysis: Comparison of MRI, CT and dual energy X-ray absorptiometry. Br J Radiol 2009;82:123–130
Carpenter J, Bithell J. Bootstrap confidence intervals: when, which, what? A practical guide for medical statisticians. Stat Med 2000; 19:1141–1164
Falaschetti E, Laiho J, Primatesta P, Purdon S. Prediction equations for normal and low lung function from the health survey for England. Eur Respir J 2004;23:456–463
Beaudart C, Zaaria M, Reginster J. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS One 2017;12:e0169548
Schaap LA, Schoor NM Van, Lips P, Visser M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: The Longitudinal Aging Study Amsterdam. Journals Gerontol Med Sci 2018;73:1199–1204
Bischoff-Ferrari HA, Orav JE, Kanis JA, et al. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Sarcopenia 2015;26:2793–2802
Acknowledgements
This research was made possible using the data/biospecimens collected by the Canadian Longitudinal Study on Aging (CLSA). Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation. This research has been conducted using the CLSA dataset, Baseline Comprehensive Dataset version 4.0, under Application Number 160608. The CLSA is led by Drs. Parminder Raina, Christina Wolf son and Susan Kirkland. The opinions expressed in this manuscript are the author’s own and do not reflect the views of the Canadian Longitudinal Study on Aging.
Funding
No funding to report.
Author information
Authors and Affiliations
Contributions
AJM, SMP, and PR conceptualized this project with feedback from NS, LT, PDM, RJd and GP. AJM and NS completed the analysis of the data. AJM, NS, and PR interpreted the results. AJM completed the draft of the manuscript with revisions from the remaining authors. All authors provided approval for the final version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval for this project was received by the Hamilton Research Ethics Board (#2686).
Additional information
Conflict of interest
None declared
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Mayhew, A.J., Phillips, S.M., Sohel, N. et al. Methodological Issues and the Impact of Age Stratification on the Proportion of Participants with Low Appendicular Lean Mass When Adjusting for Height and Fat Mass Using Linear Regression: Results from the Canadian Longitudinal Study on Aging. J Frailty Aging 10, 150–155 (2021). https://doi.org/10.14283/jfa.2020.48
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.14283/jfa.2020.48