
Abstract
Background
Ovarian cancer with miliary disease spread is an aggressive phenotype lacking targeted management strategies. We sought to determine whether adjuvant intravenous/intraperitoneal (IV/IP) chemotherapy is beneficial in this disease setting.
Methods
Patient/tumor characteristics and survival data of patients with stage IIIC epithelial ovarian cancer who underwent optimal primary debulking surgery from 01/2010 to 11/2014 were abstracted from records. Chi-square and Mann–Whitney U tests were used to compare categorical and continuous variables. The Kaplan–Meier method was used to estimate survival curves, and outcomes were compared using log-rank tests. Factors significant on univariate analysis were combined into multivariate logistic regression survival models.
Results
Among 90 patients with miliary disease spread, 41 (46%) received IV/IP chemotherapy and 49 (54%) received IV chemotherapy. IV/IP chemotherapy, compared with IV chemotherapy, resulted in improved progression-free survival (PFS; 23.0 versus 12.0 months; p = 0.0002) and overall survival (OS; 52 versus 36 months; p = 0.002) in patients with miliary disease. Among 78 patients with nonmiliary disease spread, 23 (29%) underwent IV/IP chemotherapy and 55 (71%) underwent IV chemotherapy. There was no PFS or OS benefit associated with IV/IP chemotherapy over IV chemotherapy in these patients. On multivariate analysis, IV/IP chemotherapy was associated with improved PFS (HR, 0.28; 95% CI 0.15–0.53) and OS (HR, 0.33; 95% CI 0.18–0.61) in patients with miliary disease compared with those with nonmiliary disease (PFS [HR, 1.53; 95% CI 0.74–3.19]; OS [HR, 1.47; 95% CI 0.70–3.09]).
Conclusions
Adjuvant IV/IP chemotherapy was associated with oncologic benefit in miliary disease spread. This survival benefit was not observed in nonmiliary disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The increasing use of phenotypic, genetic, and molecular profiling is rapidly changing the therapeutic landscape of ovarian cancer. For example, testing for homologous recombination deficiency has opened the door for the use of poly ADP-ribose polymerase (PARP) inhibition, and laparoscopic assessment of disease burden/distribution has emerged as a modality to determine the likelihood of achieving a successful surgical resection.1,2 Several studies have demonstrated that miliary disease distribution, defined as diffuse abdominal and pelvic tumor studding in the absence of bulky pelvic and abdominal disease, is associated with decreased rates of complete gross resection and worse prognoses.3,4 Despite the aggressive nature of this tumor phenotype, there are no targeted strategies for its clinical management.
In the mid-1980s, pharmacologic and clinical studies showed a survival benefit with intravenous/intraperitoneal (IV/IP) administration of chemotherapy in the management of ovarian cancer, which was subsequently validated by multicenter, randomized controlled trials Gynecologic Oncology Group (GOG) 104, GOG 114, and GOG 172.5,6,7,8,9 In 2006, the National Cancer Institute issued a clinical announcement supporting the use of IV/IP chemotherapy in the treatment of optimally cytoreduced advanced-stage ovarian cancer, stating that “a combination of IV and IP administration of chemotherapy conveys a significant survival benefit among women with optimally debulked epithelial ovarian cancer compared to IV administration alone.” However, these findings were later contradicted by the results of GOG 252, which suggested no benefit with IV/IP chemotherapy when administered in conjunction with maintenance bevacizumab.10
Given the peritoneal-based pattern of spread of ovarian cancer, we hypothesized that patients with disseminated miliary disease at presentation may uniquely benefit from adjuvant IV/IP chemotherapy. The primary objective of this study was to compare the oncologic outcomes of patients with miliary, high-grade, stage IIIC epithelial ovarian/fallopian tube/primary peritoneal carcinoma (EOC) who underwent IV/IP chemotherapy versus those who underwent IV chemotherapy alone. The secondary objective was to compare the survival outcomes of patients with nonmiliary disease spread who underwent IV/IP chemotherapy with those who underwent IV chemotherapy alone.
Patients and Methods
After institutional review board approval, we performed a retrospective chart review of patients at Brigham and Women’s Hospital and Massachusetts General Hospital who underwent primary debulking surgery for stage IIIC EOC between 1 January 2010 and 31 November 2014. Patients were excluded from analysis if they were treated with neoadjuvant chemotherapy; had not undergone debulking surgery; underwent suboptimal debulking; had stage I, II, or IV disease; had nonepithelial or low-grade disease; did not have a description of initial disease distribution or residual tumor burden documented in their operative report; or had incomplete medical records. Patients were then categorized as having had miliary or nonmiliary disease spread based on the description of initial disease burden previously defined by Torres et al.3,4 The miliary subtype group included patients with diffuse abdominal and pelvic tumor studding with or without omental caking in the absence of bulky pelvic and abdominal disease, as described in their operative records (Supplementary Fig. 1). The nonmiliary subtype group included patients with bulky abdominopelvic disease who did not meet the descriptive criteria for miliary disease.
Patients in both groups were then further separated into two groups based on whether they had (at least one cycle) or had not received IV/IP chemotherapy (Fig. 1). Treatment with IV/IP chemotherapy was based on the surgeon’s discretion. IV/IP chemotherapy regimens included the “GOG 172 regimen” (IV paclitaxel 135 mg/m2 × 24 h on day 1 followed by IP cisplatin 100 mg/m2 on day 2, then IP paclitaxel 60 mg/m2 on day 8) and the “modified GOG 172 regimen” (IV paclitaxel 135 mg/m2 × 24 h on day 1 followed by IP cisplatin 75 mg/m2 on day 2, then IP paclitaxel 60 mg/m2 on day 8). The intent of adjuvant chemotherapy was to administer six cycles of treatment to both the IV/IP chemotherapy and IV chemotherapy alone groups.

Study design
Differences in clinical and treatment factors between patients who underwent IV chemotherapy and those who underwent IV/IP chemotherapy were examined for both the miliary and nonmiliary patient subgroups. Clinical factors included age, body mass index (BMI), Charlson comorbidity index (CCI), and BRCA mutational status. Treatment-related factors included mean operative time, mean estimated blood loss, receipt of maintenance therapy, surgical complexity, extent of residual disease at the conclusion of primary debulking surgery, mean number of IV/IP chemotherapy cycles, and receipt of the GOG 172 regimen versus the modified GOG 172 regimen. Surgical procedures were assigned a complexity score reflecting the difficulty and number of procedures performed, as described by Aletti et al.11,12 Patients with visible remaining gross residual disease ≤ 1 cm (maximal diameter of largest residual tumor nodule) after primary debulking surgery were considered to have undergone optimal debulking, and those with no visible disease were considered to have undergone a complete gross resection.
Differences in variables were examined with the chi-square test for categorical variables and Mann–Whitney U test for continuous variables, as indicated. p-Value < 0.05 was considered statistically significant. Associations are reported as hazard ratios (HRs) with 95% confidence intervals. Progression-free survival (PFS) was defined as the number of months between date of primary debulking surgery and disease progression based on computed tomography (CT) findings or biopsy, or death, whichever came first. Overall survival (OS) was defined as the number of months between date of primary debulking surgery and death from any cause. Patients who were alive and progression free or alive with disease were censored for PFS and OS, respectively, at date of last follow-up. The Kaplan–Meier method was used to estimate survival curves, and survival outcomes were compared using log-rank tests. Factors significant on univariate analysis were then combined into a multivariate logistic regression model of PFS and OS. The SAS version 9.4 (SAS Institute Inc, Cary, NC) statistical package was used for all statistical analyses.
Results
Among 168 patients who underwent optimal cytoreduction for stage IIIC high-grade EOC during the study period, 90 (54%) had miliary spread and 78 (46%) did not.
Miliary Subtype Group: Patient and Treatment Characteristics
Of patients with miliary disease, 41 (46%) received IV/IP chemotherapy and 49 (54%) received IV chemotherapy alone. The mean number of IP chemotherapy cycles was 4.4 (SD 1.7), and 17 patients (41%) completed all six cycles of IV/IP chemotherapy. Of 39 patients with available dosing information, 19 (49%) received the GOG 172 regimen and 20 (51%) received the modified GOG 172 regimen.
Miliary patients undergoing IV/IP chemotherapy versus IV chemotherapy alone were more likely to be < 70 years old (83% versus 59%, respectively; p = 0.01) and have lower mean BMI (25.5 kg/m2 versus 28.5 kg/m2, respectively; p = 0.01). There were no significant differences in BRCA mutational status, receipt of maintenance therapy, or age-adjusted CCI between those who received IV/IP chemotherapy and those who received IV chemotherapy alone (Table 1).
Patients with miliary disease who received IV/IP chemotherapy compared with those who received IV chemotherapy alone had longer mean operative time (275.5 versus 218.1 min, respectively; p ≤ 0.05) but lower mean estimated blood loss (EBL; 557.5 versus 832.7 mL, respectively; p = 0.02). Rates of high surgical complexity were similar (75.6% versus 81.6%, respectively; p = 0.49). Patients who received IV/IP chemotherapy were also more likely to have undergone complete gross resection (29% versus 12%, respectively; p = 0.04) (Table 1).
Nonmiliary Subtype Group: Patient and Treatment Characteristics
Of the 78 patients with nonmiliary disease, 23 (29%) received IV/IP chemotherapy and 55 (71%) received IV chemotherapy alone. The mean number of IP chemotherapy cycles was 4.7 (SD 1.9), and 14 patients (61%) completed all six cycles of IV/IP chemotherapy. Of 22 patients with available dosing information, 12 (54.5%) received the GOG 172 regimen and 10 (45.5%) received the modified GOG 172 regimen.
There were no significant differences in age, mean BMI, BRCA mutational status, receipt of maintenance therapy, or CCI between patients who received IV/IP chemotherapy and those who received IV chemotherapy alone (Table 1).
There were no significant differences in mean operative time or mean EBL between patients who received IV/IP chemotherapy and those who received IV chemotherapy alone (Table 1). There was no difference between the rates of high surgical complexity (65% versus 74%, respectively; p = 0.53). There was also no difference between the rates of complete gross resection (78% versus 80%, respectively; p = 0.86).
Miliary Subtype Group: Progression-Free and Overall Survival
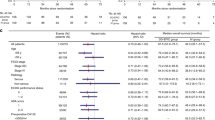
Among the 90 patients with miliary disease, there were 77 recurrences (86%). Patients who received IV/IP chemotherapy had an 11-month improvement in median PFS compared with patients who received IV chemotherapy alone (23.0 versus 12.0 months, respectively; p = 0.0002) (Fig. 2). On univariate analysis, IV/IP chemotherapy compared with IV chemotherapy alone was associated with decreased risk of recurrence (HR, 0.29; 95% CI 0.16–0.52). Optimal cytoreduction compared with complete gross resection was associated with an increased risk of recurrence (HR, 3.31; 95% CI 1.42–7.75). Other variables, including age, surgical complexity, and age-adjusted CCI, did not significantly influence PFS (Supplementary Table 1). On multivariate analysis, which included variables of age, receipt of IV/IP chemotherapy, residual disease burden, and histology, IV/IP chemotherapy compared with IV chemotherapy alone was independently associated with improved PFS (HR, 0.28; 95% CI 0.15–0.53) (Table 2).

Association of IV/IP chemotherapy with progression-free survival in miliary (a) and nonmiliary patients (b)
There were 56 deaths (62%) among the 90 patients with miliary disease. Median OS was 16.0 months longer for patients who received IV/IP chemotherapy compared with those who received IV chemotherapy alone (52.0 versus 36.0 months, respectively; p = 0.002) (Fig. 3). On univariate analysis, IV/IP chemotherapy compared with IV chemotherapy alone was associated with decreased risk of death (HR, 0.33; 95% CI 0.18–0.61). Optimal cytoreduction compared with complete gross resection was associated with a trend towards increased risk of death (HR, 2.22; 95% CI 0.95–5.21). Age ≥ 70 years was also associated with a trend towards increased risk of death (HR, 1.51; 95% CI 0.87–2.63). There were no significant differences in OS based on surgical complexity or age-adjusted CCI (Supplementary Table 1). On multivariate analysis, which included variables of age, receipt of IV/IP chemotherapy, and residual disease burden, IV/IP chemotherapy compared with IV chemotherapy alone was independently associated with OS (HR, 0.33; 95% CI 0.18–0.61) (Table 2).

Association of IV/IP chemotherapy with overall survival in miliary (A) and nonmiliary patients (b)
Nonmiliary Subtype Group: Progression-Free and Overall Survival
Among the 78 patients with nonmiliary disease, there were 56 recurrences (72%). Median PFS was similar between patients treated with IV/IP chemotherapy and those treated with IV chemotherapy alone (17.0 versus 29.0 months, respectively; p = 0.33) (Fig. 2). On univariate analysis, IV/IP chemotherapy did not significantly impact risk of recurrence (HR, 1.61; 95% CI 0.79–3.32). Other variables, including age, CCI, surgical complexity, and residual disease burden, did not significantly influence PFS (Supplementary Table 2). On multivariate analysis, which included variables of age, receipt of IV/IP chemotherapy, residual disease burden, and histology, IV/IP chemotherapy compared with IV chemotherapy alone did not impact PFS (HR, 1.53; 95% CI 0.74–3.19) (Table 3).
There were 33 deaths (42%) among the 78 patients with nonmiliary disease. Median OS was 64.0 months for patients who received IV/IP chemotherapy versus not reached for patients who received IV chemotherapy alone (p = 0.29) (Fig. 3). On univariate analysis, IV/IP chemotherapy compared with IV chemotherapy alone did not significantly impact risk of death (HR, 1.56; 95% CI 0.76–3.20). Other variables, including age, CCI, and residual disease burden, did not significantly influence OS. On multivariate analysis, which included variables of age, receipt of IV/IP chemotherapy, residual disease burden, and histology, IV/IP chemotherapy compared with IV chemotherapy alone was not significantly associated with OS (HR, 1.47; 95% CI 0.70–3.09) (Table 3).
Discussion
The findings of this retrospective cohort study demonstrated a significant survival benefit associated with use of IV/IP chemotherapy over IV chemotherapy alone among patients with stage IIIC ovarian cancer who presented with disseminated miliary disease spread. Specifically, PFS was prolonged by 11.0 months and OS by 16.0 months in patients who received IV/IP chemotherapy. This benefit was not observed in patients with nonmiliary disease spread, with no significant difference in PFS or OS associated with IV/IP chemotherapy.
The magnitude of the survival benefit observed in the miliary subtype group represents a potentially consequential finding, but also merits discussion on the possible confounding variables associated with the study outcome. Specifically, we sought to exclude two possibilities: (1) unintended patient selection bias among the IV and IV/IP subgroups of patients with miliary disease and between the miliary and nonmiliary cohorts; and (2) significant differences in the chemotherapy regimens and/or cycle completion between the IV/IP cohorts of the miliary and nonmiliary subtypes.
In the first assessment, we sought to determine whether certain characteristics known to drive survival benefit, such as age, CCI, surgical complexity, BRCA status, receipt of maintenance therapy, and residual disease volume, explained the survival improvement observed in patients with miliary disease who received IV/IP chemotherapy.11 While there was no significant difference in CCI, surgical complexity, BRCA status, or receipt of maintenance therapy between patients in the miliary subtype group who received IV chemotherapy and those who received IV/IP chemotherapy, we did find that the patients triaged to IV/IP chemotherapy were younger and were more likely to have undergone complete gross resection. Given that age and residual disease volume are associated with OS and were significantly different between patients with miliary disease who received IV chemotherapy and those who received IV/IP chemotherapy, we performed a multivariate logistic regression analysis that included age, residual disease volume, and use of IV/IP chemotherapy. In this model, IV/IP chemotherapy remained significantly associated with improved OS (HR, 0.33; 95% CI 0.18–0.66).
We performed a similar analysis among patients with nonmiliary disease to determine whether there was a disproportionate representation of poor prognostic factors in the nonmiliary subtype group who received IV/IP chemotherapy that could explain the lack of benefit with this approach. Of note, there were no differences in age, CCI, surgical complexity, BRCA status, receipt of maintenance therapy, or residual disease volume between those who received IV chemotherapy alone and those who received IV/IP chemotherapy. Although these factors were not found to be significantly different on univariate analysis, because of their known impact on survival, we incorporated age and residual disease volume as well as IV/IP chemotherapy into a multivariate logistic regression model. Under this model, IV/IP chemotherapy was not significantly associated with a survival benefit.
In the second assessment, we investigated whether patients with miliary disease compared with those without miliary disease were more likely to have received or completed the more aggressive GOG 172 regimen, which is more time consuming and less tolerable.13 In total, 47% of miliary patients were treated with the GOG 172 regimen, with a mean of 4.4 (SD 1.7) IP chemotherapy cycles, while 50% of the patients in the nonmiliary subtype group were treated with the GOG 172 regimen, with a mean of 4.7 (SD 1.9) IP chemotherapy cycles. The similarity in cycle number and chemotherapy dosage between the two subtype groups suggests this did not account for the differences in survival advantage observed with IV/IP chemotherapy administration between patients with miliary versus nonmiliary disease.
The recently published findings of study GOG 252 did not demonstrate a survival advantage with IV/IP chemotherapy over IV chemotherapy, and many have questioned whether modifications in the dosing and scheduling of IV/IP chemotherapy, and/or the addition of bevacizumab, underlie the discrepant results of GOG 252 and GOG 172.10 In the context of our data and findings, it is possible that the unique characteristics of the patient cohorts, specifically the mix of patients with miliary and nonmiliary spread, which were not reported in the GOG trials, contributed to our results. Similar questions have been explored in previous investigations of IV/IP chemotherapy in patient subsets stratified by retroperitoneal-based disease, tumor histology, and BRCA mutational status, but not on the basis of miliary versus nonmiliary phenotype.14,15,16 These phenotype subsets represent an intriguing target for future research to validate whether EOC patients with miliary disease represent an appropriate group for IV/IP chemotherapy.
As with other retrospective studies, this report and its conclusions are limited by the accuracy and completeness of medical records, the reliance on individual surgeon discretion in assigning patients to IV/IP chemotherapy, and the relatively small number of patients included in this analysis, which limits the power and confidence to make definitive conclusions. Because miliary disease is a poor prognostic factor in ovarian cancer, we first separated patients into miliary and nonmiliary disease subtype groups before examining the association of IV/IP chemotherapy with improved survival outcomes. This ultimately restricted our sample sizes to 23 patients in the nonmiliary group who received IV/IP chemotherapy and 41 patients in the nonmiliary group who received IV chemotherapy. Additionally, this study does not provide information describing the mechanism of action driving the benefit of IV/IP chemotherapy in patients with miliary spread. Possible explanations may include the chemotherapeutic sensitivity of miliary tumor subtypes or the addition of IP chemotherapy resulting in local targeting of miliary tumor, which may be more peripheral and less accessible to IV-administered therapeutics; however, additional investigation is warranted.4,17,18
In conclusion, this study identified a subset of patients with advanced-stage ovarian cancer (i.e., those with miliary disease) in whom IV/IP chemotherapy was associated with a significant survival benefit. This survival benefit was not observed in a similar cohort of patients with nonmiliary spread. The association between IV/IP chemotherapy and improved PFS and OS in the miliary subtype group maintained its significance after adjusting for age and residual disease burden in multivariate analysis. On additional analysis, there were no differences in baseline or treatment characteristics between the miliary and nonmiliary groups who received IV/IP chemotherapy. Taken together, our findings suggest that patients with optimally cytoreduced, stage IIIC ovarian cancer with miliary spread may represent a subset of patients with aggressive disease who could benefit from IV/IP chemotherapy.
Disclosure
Michael Worley Jr.: CONMED corporation (consulting and honoraria). All other authors report no conflicts of interest.
References
Konstantinopoulos PA, Ceccaldi R, Shapiro GI, D’Andrea AD. Homologous Recombination deficiency: exploiting the fundamental vulnerability of ovarian cancer. Cancer Discov. 2015;5(11):1137–54.
Fagotti A, Ferrandina G, Fanfani F, Ercoli A, Lorusso D, Rossi M, et al. A laparoscopy-based score to predict surgical outcome in patients with advanced ovarian carcinoma: a pilot study. Ann Surg Oncol. 2006;13(8):1156–61.
Fagotti A, Vizzielli G, De Iaco P, Surico D, Buda A, Mandato VD, et al. A multicentric trial (Olympia-MITO 13) on the accuracy of laparoscopy to assess peritoneal spread in ovarian cancer. Am J Obstet Gynecol. 2013;209(5):462e1–11.
Torres D, Kumar A, Wallace SK, Bakkum-Gamez JN, Konecny GE, Weaver AL, et al. Intraperitoneal disease dissemination patterns are associated with residual disease, extent of surgery, and molecular subtypes in advanced ovarian cancer. Gynecol Oncol. 2017;147(3):503–8.
Alberts DS, Liu PY, Hannigan EV, O’Toole R, Williams SD, Young JA, et al. Intraperitoneal cisplatin plus intravenous cyclophosphamide versus intravenous cisplatin plus intravenous cyclophosphamide for stage III ovarian cancer. N Engl J Med. 1996;335(26):1950–5.
Markman M, Bundy BN, Alberts DS, Fowler JM, Clark-Pearson DL, Carson LF, et al. Phase III trial of standard-dose intravenous cisplatin plus paclitaxel versus moderately high-dose carboplatin followed by intravenous paclitaxel and intraperitoneal cisplatin in small-volume stage III ovarian carcinoma: an intergroup study of the Gynecologic Oncology Group, Southwestern Oncology Group, and Eastern Cooperative Oncology Group. J Clin Oncol. 2001;19(4):1001–7.
Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354(1):34–43.
Dedrick RL, Myers CE, Bungay PM, DeVita VT Jr. Pharmacokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat Rep. 1978;62(1):1–11.
Markman M, Howell SB, Lucas WE, Pfeifle CE, Green MR. Combination intraperitoneal chemotherapy with cisplatin, cytarabine, and doxorubicin for refractory ovarian carcinoma and other malignancies principally confined to the peritoneal cavity. J Clin Oncol. 1984;2(12):1321–6.
Walker JL, Brady MF, Wenzel L, Fleming GF, Huang HQ, DiSilvestro PA, et al. Randomized trial of intravenous versus intraperitoneal chemotherapy plus bevacizumab in advanced ovarian carcinoma: an nrg oncology/gynecologic oncology group study. J Clin Oncol. 2019;37(16):1380–90.
Manning-Geist BL, Hicks-Courant K, Gockley AA, Clark RM, Del Carmen MG, Growdon WB, et al. Moving beyond “complete surgical resection” and “optimal”: is low-volume residual disease another option for primary debulking surgery? Gynecol Oncol. 2018;150(2):233–228.
Aletti GD, Podratz KC, Moriarty JP, Cliby WA, Long KH. Aggressive and complex surgery for advanced ovarian cancer: an economic analysis. Gynecol Oncol. 2009;112(1):16–21.
Wright AA, Cronin A, Milne DE, Bookman MA, Burger RA, Cohn DE, et al. Use and effectiveness of intraperitoneal chemotherapy for treatment of ovarian cancer. J Clin Oncol. 2015;33(26):2841–7.
Landrum LM, Java J, Mathews CA, Lanneau GS Jr, Copeland LJ, Armstrong DK, et al. Prognostic factors for stage III epithelial ovarian cancer treated with intraperitoneal chemotherapy: a Gynecologic Oncology Group study. Gynecol Oncol. 2013;130(1):12–8.
Naumann RW, Morris JC, Tait DL, Higgins RV, Crane EK, Drury LK, et al. Patients with BRCA mutations have superior outcomes after intraperitoneal chemotherapy in optimally resected high grade ovarian cancer. Gynecol Oncol. 2018;151(3):477–80.
Lesnock JL, Darcy KM, Tian C, Deloia JA, Thrall MM, Zahn C, et al. BRCA1 expression and improved survival in ovarian cancer patients treated with intraperitoneal cisplatin and paclitaxel: a gynecologic oncology group study. Br J Cancer. 2013;108(6):1231–7.
Los G, Mutsaers PH, Lenglet WJ, Baldew GS, McVie JG. Platinum distribution in intraperitoneal tumors after intraperitoneal cisplatin treatment. Cancer Chemother Pharmacol. 1990;25(6):389–94.
Hasovits C, Clarke S. Pharmacokinetics and pharmacodynamics of intraperitoneal cancer chemotherapeutics. Clin Pharmacokinet. 2012;51(4):203–24.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Fig. 1
Miliary disease type
Supplemental Table 1
Univariate analysis of factors associated with survival in miliary patients (DOCX 20 KB)
Supplemental Table 2
Univariate analysis of factors associated with survival in nonmiliary patients (DOCX 20 KB)
Rights and permissions
About this article

{kind=link}
Cite this article
Manning-Geist, B.L., Sullivan, M.W., Sarda, V. et al. Disease Distribution at Presentation Impacts Benefit of IP Chemotherapy Among Patients with Advanced-Stage Ovarian Cancer. Ann Surg Oncol 28, 6705–6713 (2021). https://doi.org/10.1245/s10434-021-09746-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-09746-w