
Abstract
Molecular genomic testing provides clinicians with both prognostic and (sometimes) predictive information that can help individualize treatment and decrease the risk of over- or under-treatment. We review the genomic tests that are currently available for clinical use in management of breast cancer, discuss ongoing research related to validating and expanding their utility in different patient populations, and explain why it is important for surgeons to know how to incorporate these tools into their clinical practice in order to individualize patient treatment, reduce unnecessary morbidity, and, accordingly, improve outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Survival after breast cancer diagnosis has improved dramatically over the past 50 years with the introduction and refinement of multidisciplinary treatment regimens that include surgical resection, radiation treatment, and systemic therapy. However, many highly effective systemic agents are also associated with significant, and sometimes permanent, toxicity. Accordingly, increasing attention has been devoted to improving clinicians’ collective ability to discern which patients are most and least likely to benefit from receipt of systemic chemotherapy. Molecular genomic assays have emerged as important tools in the pursuit of increasingly personalized treatment for breast cancer.
Although most of these tests were developed for and are still primarily used after definitive surgical resection, their use in the neoadjuvant setting is also being explored. For this and other reasons, we believe they are important tools with which surgeons should be familiar and should feel comfortable ordering for their patients. There are advantages to having the surgeon identify the appropriate patient for genomic testing; For example, the time to a decision about administration of systemic chemotherapy is much shorter when the surgeon orders the test than when it is ordered by the medical oncologist. At the University of Texas MD Anderson Cancer Center, this window of time was cut approximately in half when the surgeon ordered the test, which has obvious benefits for both the patient and the multidisciplinary team. Surgeon-initiated testing would often allow patients and their medical oncologists to come to a firm decision on chemotherapy benefit at the time of their initial consultation. In contrast, when the medical oncologist orders the test at the initial consultation, there can be a 10- to 14-day waiting period for the score to return, resulting in an already anxious patient’s having to wait for a decision regarding chemotherapy. Furthermore, concerns about the surgeon’s not being qualified to identify appropriate patients appear unfounded. A 2011 study by Joh and colleagues found that surgeons actually had the highest degree of accuracy (compared with medical oncologists and pathologists) in predicting which patients would eventually receive systemic chemotherapy.1
Here, we review the genomic tests that are currently available and/or in development for clinical use in management of breast cancer (Table 1), discuss ongoing research related to validating and expanding their utility in different patient populations, and explain why it is important for surgeons to know how to incorporate these tools into their clinical practice.
Genomic Assays
Oncotype DX
First developed in 2004, Oncotype DX® (Genomic Health, Redwood, CA) is a 21-gene (16 breast-cancer-related genes and 5 reference genes) reverse-transcriptase polymerase chain reaction (RT-PCR) assay that was developed through a multistep process that involved (1) development of an RT-PCR method that could use formalin-fixed, paraffin-embedded (FFPE) samples, (2) selection of 250 candidate genes based on reviews of published literature and microarray experiments, (3) conducting studies using three independent cohorts of breast cancer patients (n = 447), viz. participants in the NSABP-20 trial [all node-negative (LN−) and estrogen receptor (ER)-positive (ER−)],2 patients with extensive (≥ 10 involved nodes) axillary disease who received treatment at Rush University Medical Center [Chicago, IL; including both ER+ and ER-negative (ER−) patients],3 and women treated for breast cancer at Providence St. Joseph’s Medical Center [Burbank, CA; including node-positive (LN+), LN−, ER+ , and ER− patients],4 to examine the association between the candidate genes and breast cancer recurrence, and (4) using the results of these studies to select the 21 genes for the panel and to develop a genome-based algorithm for predicting recurrence.5
The assay was retrospectively validated in 668 tumor samples from women who received adjuvant tamoxifen as part of the NSABP-14 trial, the participants of which all had ER+ , HER2/neu nonamplified (HER2−), LN− breast cancer, and was shown to be able to quantify both the likelihood of distant recurrence within 10 years (i.e., to be prognostic) and also the likely magnitude of improved distant-recurrence-free survival that would occur with receipt of both adjuvant endocrine therapy and chemotherapy as opposed to only receiving endocrine therapy (i.e., to be predictive).5,6 Although not formally approved by the Food and Drug Administration (FDA), Oncotype DX is currently the only genomic assay recommended in treatment guidelines published by the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Center Network (NCCN) and is also recommended by both the European Society for Medical Oncology (ESMO) and the St. Gallen International Breast Cancer Conference for management of invasive carcinoma. A 12-gene version has also been shown to exhibit prognostic reliability for local recurrence of ductal carcinoma in situ (DCIS).7,8
Oncotype DX uses FFPE from surgical specimens to categorize patients into one of three tiers based on a calculated recurrence score (RS): low (< 18), intermediate (18–30), and high (≥ 31–100), reflecting their likelihood of distant recurrence in 10 years. In the Trial Assigning IndividuaLized Options for Treatment (Rx), also known as TAILORx, women with recurrence score less than 11 were found to have < 1% risk of recurrence in 10 years with receipt of endocrine therapy alone, further bolstering support for a paradigm shift away from mandatory chemotherapy within the context of multimodal treatment.9 Results from the West German Study Group phase III PlanB trial provided additional, prospectively generated evidence that patients with Oncotype DX RS ≤ 11 could avoid chemotherapy without compromising outcomes, even if said patients had clinicopathologic characteristics that would otherwise point towards high risk of recurrence.10 Based on the prospective, level-one data from TAILORx documenting excellent outcomes for patients with score < 11, the upcoming 8th edition of the American Joint Commission on Cancer (AJCC) Cancer Staging Manual allows patients with Oncotype DX recurrence score < 11 to be downstaged from the previous anatomic stage/prognostic group to stage IA.11 Currently, Oncotype DX is the only genomic assay that can be used in the AJCC 8th edition to downstage patients.
Oncotype DX currently issues separate reports for LN− and LN+ (N1–3) patients. The Rx for Positive Node, Endocrine Responsive Breast Cancer (RxPONDER) trial was initiated in 2011 to explore whether ER+ , HER2− patients with limited nodal disease (1–3 LNs) and low to intermediate Oncotype DX scores would experience decreased survival if chemotherapy were omitted from their regimen; another aim of this trial is to determine whether there is an optimal RS cutoff point for these patients, above which chemotherapy should always be recommended.12. The 21-gene Oncotype DX assay is mentioned in the NCCN guidelines as a possible consideration to help guide addition of chemotherapy in patients with limited (1–3) positive nodes, since there are ample data from the Southwest Oncology Group (SWOG) 8814,13 the NSABP B-28,14 and the studies mentioned above to suggest that it provides predictive utility of chemotherapy benefit in patients with limited nodal involvement. The results from the RxPONDER trial should help clarify the role of genomic testing with Oncotype DX in LN+ patients.
As the most widely used genomic assay for breast cancer in the USA, Oncotype DX has also been the most frequently examined in independent patient cohorts and cost analyses.15 However, it has been demonstrated to have a high false-negative rate for tumors that are HER2+ , and, therefore, is not indicated for use in HER2+ patients.16 Furthermore, the intermediate RS category sometimes represents a clinical conundrum for providers, and its accuracy in the neoadjuvant setting has yet to be prospectively demonstrated.
Advantages of neoadjuvant systemic therapy include not only improving the feasibility of breast conservation in patients with large primary tumors but also the provision of prognostic information regarding tumor response. Those who achieve pathologic complete response (pCR) fare better in terms of both recurrence-free and overall survival.17 However, due not only to the side-effects of neoadjuvant chemotherapy but also to the potential for disease progression while on therapy, patients must be carefully selected. There are limited data to date on the utility of any molecular genomic testing for predicting the efficacy of neoadjuvant chemotherapy; For instance, Yardley et al. tested Oncotype DX on core-needle biopsy samples of breast cancer patients prior to undergoing neoadjuvant chemotherapy.18 All patients who achieved pCR following neoadjuvant chemotherapy had pretreatment Oncotype DX score greater than 31, which corresponded to a 17% pCR rate in ER+ patients and 31% pCR rate in ER– patients with high Oncotype DX score. Similar results were seen in a recent, prospective, multicenter pilot trial examining whether Oncotype DX scores on core-needle biopsy blocks from patients with hormone receptor-positive (HR+), Her2− invasive breast cancer can accurately guide neoadjuvant systemic therapy.19 Patients were randomized to receive either neoadjuvant hormone therapy or neoadjuvant chemotherapy. The highest clinical response rates occurred in patients with Oncotype DX score of 26 or greater receiving neoadjuvant chemotherapy. Furthermore, in-breast and nodal pCR were only observed in this group, and conceptually it makes sense that those at greatest risk of recurrence as demonstrated by high Oncotype DX score would benefit most from neoadjuvant chemotherapy. This novel use of molecular genomic testing in the neoadjuvant setting highlights the importance of ongoing research that focuses on increasingly selective application of chemotherapy regimens to those who would receive the most benefit.
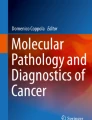
Even though Oncotype DX can be performed on core biopsy specimens, at MD Anderson, the test is usually ordered on the final pathology specimen rather than the core biopsy sample, in order to minimize the likelihood of having ordered an inappropriate test if multiple positive nodes are identified at operation, thus establishing the need for chemotherapy regardless of Oncotype RS. Figure 1 provides an algorithm that surgeons can use to assist them in appropriate use of Oncotype DX on core-needle and surgical specimens.

Proposed Oncotype DX algorithm for surgeons
In a recent trial comparing Oncotype DX with other predictive assays, Oncotype DX assigned the highest proportion of tumors to the low-risk category, thereby potentially sparing the greatest number of women from overtreatment with chemotherapy. Arguments that some of these patients might be undertreated based on low scores appear unfounded based on recent data showing that patients with low Oncotype recurrence scores had recurrence rates of around 1% at 10 years.9,20,21
MammaPrint
MammaPrint®, which was first described in 2006, is a 70-gene DNA assay developed by Agendia (Irvine, CA), a commercial spin-off of the Netherlands Cancer Institute (NKI) and Antoni van Leeuwenhoek Hospital in Amsterdam.22 It consists of a customized microarray slide that assesses in triplicate the messenger RNA (mRNA) expression of 70 genes initially identified in 78 tumors from a cohort of T1-2, LN− breast cancer patients under the age of 55 years at diagnosis and treated at NKI; 50% of these patients were ER+.23 The assay can use either fresh-frozen tumor samples or FFPE. The MammaPrint index (i.e., score) ranges from −1 to +1; tumors with MammaPrint index < 0.4 are classified as having low risk of distant metastasis in 10 years, while those tumors with score ≥ 0.4 are at high risk for developing distant metastases in 10 years.24,25 MammaPrint was the first genomic assay approved by the FDA and is the most widely used breast cancer-specific genomic assay in Europe.
Initially, MammaPrint was internally validated using only 19 tumors, and its development was criticized for the small size of both the reference and test cohorts. However, its prognostic value was subsequently validated through a retrospective series using 61 LN− patients from the initial reference group as well as 144 new LN+ patients and 90 new LN− patients and was found to better predict 5-year overall survival and the likelihood of developing distant metastases at 5 years than the clinicopathologic risk criteria for recurrence found within the then-current guidelines of both St. Gallen and the National Institutes of Health (NIH); 77% of the 295 patients in this study were ER+.23 Retrospective validation was again performed as part of the international multicenter trial by the TRANSBIG consortium, which included 302 T1-2, LN− patients diagnosed prior to 1999 who were less than 61 years old at diagnosis and whose treatment was limited to locoregional therapy (i.e., did not receive systemic therapy); 70% of these patients were ER+ . The trial was conducted to determine which of three candidate microarrays, viz. MammaPrint, the 76-gene Rotterdam/Veridex signature, or the Genomic Grading Index, should be selected for prospective validation in what would eventually become the MINDACT trial. No significant difference was found between the three methods, and the TRANSBIG consortium ultimately decided to use MammaPrint for prospective validation.22,24
The primary objective of the Microarray In node-negative and 1–3 positive lymph node Disease may Avoid ChemoTherapy (MINDACT) trial, which was launched in 2007, was to determine whether patients with ER+ or ER− disease and low MammaPrint score but deemed high risk for recurrence according to traditional clinicopathologic characteristics (as determined through use of Adjuvant Online!®) could safely be spared chemotherapy.24 It was estimated that 10–20% of women who would have received adjuvant chemotherapy based on clinicopathological criteria would be able to forgo systemic therapy without having any adverse effect on their survival. A total of 6693 patients were enrolled in the study between 2007 and 2011 across nine countries; 80% were LN−, 88% were HR+ , and 10% were HER2/neu-amplified (HER2+). Patients with concordant high-risk (n = 1806) and low-risk (n = 2745) assessments either underwent chemotherapy or did not receive chemotherapy, respectively. Of the remaining patients with discordant evaluations, 592 were deemed low risk by Adjuvant Online! and high-risk by MammaPrint while 1550 were deemed high risk by Adjuvant Online! and low risk by MammaPrint. Among the latter cohort of 1550 patients, 748 were randomized to receive no chemotherapy; of these 748 patients, 644 were confirmed to have no change in risk post-enrollment and, therefore, received no chemotherapy. The primary analysis of these 644 patients in the MINDACT study was presented at the 2016 American Association for Cancer Research (AACR) meeting, and the full results were published in 2016.26 The authors reported that, after median follow-up of 5 years, distant metastasis-free survival was > 94% in the patients with discordant evaluations regardless of the treatment arm to which they were randomized. Also, 48% of the patients in the group deemed high risk using Adjuvant Online! and low risk according to MammaPrint had involved lymph nodes. Thus, MammaPrint may show promise as a reliable prognosticator for breast cancer patients, regardless of ER or LN status. The study authors found no added value for MammaPrint in patients who were identified as clinically low risk but had a high MammaPrint result. Notably, the MINDACT study was not powered to predict differential responses to chemotherapy, and the results of the trial should be understood in that context.
Similar results to the MINDACT trial were reported in the prospective, community-setting Netherlands study.27 With median follow-up of 61.6 months, omission of adjuvant chemotherapy supported by results from MammaPrint did not compromise outcome in terms of distant recurrence-free interval despite the risk assessment results from Adjuvant Online!. In the Adjuvant Online! high-risk group, if MammaPrint were to be used, 32% fewer patients would be eligible for adjuvant chemotherapy.
Mammostrat
First launched in 2010, Mammostrat® (Clarient Diagnostic Services, Aliso Viejo, CA) is a five-biomarker, immunohistochemical (IHC) assay that measures levels of SLC7A5, HTF9C, P53, NDRG1, and CEACAM5 in FFPE tumor samples to stratify patients receiving endocrine therapy for HR+ tumors into three groups (low, moderate, and high) that reflect risk of relapse if chemotherapy is omitted from adjuvant treatment.28 It has been retrospectively validated in multiple cohorts of patients with ER+ , ER−, LN+ , and LN− breast cancer, but its application in the USA remains limited and is not approved by the FDA.28
Prosigna Breast Cancer Prognostic Gene Signature Assay (Formerly Called the PAM50 Test)
Prosigna® (NanoString Technologies, Seattle, WA) is based on a 50-gene RT-PCR microarray (PAM50 test) that uses its proprietary nCounter® digital technology to process postoperative FFPE samples of invasive carcinoma and assign tumors to one of four intrinsic subtypes: luminal A, luminal B, HER2+ , and basal-like. In addition, the Prosigna gene signature also generates an individualized risk of recurrence (ROR) score (high, intermediate, or low) representing an estimate of the likelihood of developing recurrent disease through an algorithm that takes into account intrinsic subtype, correlation between molecular subtype and a subset of proliferative genes, and tumor size on final pathology. It has been retrospectively validated in postmenopausal women receiving adjuvant endocrine therapy for both LN+ and LN− breast cancer and was cleared by the FDA for marketing as a prognostic tool in 2013.29
Breast Cancer Index
The Breast Cancer Index (SM) (bioTheranostics Inc., San Diego, CA) represents a combination of two diagnostic tests: the two-gene, HoxB13/IL17BR ratio index (HI) and the Molecular Grade Index, a real-time RT-PCR, five-gene microarray assay; it has been retrospectively validated to predict the likelihood of late (i.e., 5–10 years after treatment) recurrence as well as the likelihood of benefit from a 10-year course of adjuvant endocrine therapy in women with early-stage, LN−, ER+ breast cancer.30,31 Specimens can be FFPE or fresh frozen. It is not currently approved by the FDA for marketing in the USA.
EndoPredict
The EndoPredict Test® (Sividon Diagnostics, Köln, Germany) combines EndoPredict—an eight-gene, mRNA-based assay that uses RT-PCR on FFPE tumor samples—with patient tumor size and nodal status to assign patients with early-stage, ER+ , HER2− breast cancer a score that reflects likelihood of distant recurrence within 10 years of diagnosis. Patients with score < 3.3 are at low risk for recurrence, while those with score ≥ 3.3 are at high risk for recurrence.32 The EndoPredict Test is not currently approved by the FDA for marketing in the USA but is approved for use in Europe.
Genomic Grade Index
The genomic grade index (MapQuant Dx, Ipsogen, France) is a DNA microarray-based assay that uses FFPE tumor samples to measure the expression of 97 genes and assign the tumor a molecular grade. The assay was developed by comparing the gene expression profiles of grade I (i.e., low-grade, well-differentiated) and grade III (i.e., high-grade, poorly differentiated) tumors and has also been streamlined into an RT-PCR version that can also use FFPE samples. The test reclassifies grade II (i.e., intermediate-grade) ER+ cancers into high- or low-grade categories and thereby confers significantly different prognoses on otherwise similar tumors.33 High GGI is associated with decreased relapse-free survival in patients who do not go on to receive adjuvant chemotherapy and is also associated with increased sensitivity to neoadjuvant chemotherapy in both ER− and ER+ patients.34
IHC4
The IHC4 assay incorporates a semiquantitative assessment of ER, progesterone receptor (PR), HER2, and Ki67 expression using IHC with clinicopathologic factors into a multivariate model for predicting risk of distant metastasis. As originally described, it uses FFPE samples, can theoretically be performed locally, and is a potentially cost-effective method for improving prognostication of early-stage breast cancer with a validated recurrence risk signature.35 However, its accuracy may be difficult to reproduce in clinical practice given potentially significant interobserver variability in IHC assessment, especially with regards to Ki67.35 The NexCourse® IHC4 assay (Genoptix, Carlsbad, CA) purports to minimize this potential variability through use of its internally developed automated quantitative analysis (AQUA) technology for quantification of ER, PR, and Ki67 expression, though HER2 expression continues to be assessed using IHC or fluorescent in situ hybridization (FISH) in their assay. In the recently published results of the OPTIMA Prelim trial, there was no significant difference between the conventional IHC4 assay and NexCourse IHC4 with regards to risk assessment for women with ER+ breast cancer.36 The applicability of this method to clinical practice continues to be a subject of investigation.
Npi+
The nottingham prognostic index (NPI) is a clinical tool that has been utilized for over 30 years to predict prognosis after breast cancer diagnosis. Using a formula that incorporates tumor grade, tumor size, and nodal involvement, patients can be categorized into one of four groups associated with different overall survival estimates, with higher NPI being associated with worse likelihood of survival at 5 years.37 More recently, a more granular method of molecular subtyping using 10 vetted biomarkers has expanded the four-tiered intrinsic subtype system, resulting in the identification of seven new breast cancer subtypes: three luminal (luminal-A, luminal-N, and luminal-B), two basal (basal p53 altered, basal p53 normal), and two HER2+ (HER2+/ER+ , HER2+/ER−).38 The NPI formula—individualized for each subgroup to only include the most significant clinicopathologic prognostic factors—was then used to further stratify these seven subgroups into prognostic groups, thereby generating a new prognosticator, NPI+ , that may prove helpful in clinical decision-making.38,39
MammaTyper
MammaTyper® is an in vivo diagnostic test (BioNTech AG, Mainz, Germany) launched in 2015 that categorizes tumors into intrinsic subtypes through quantitative measurement of ER, PR, HER2, and Ki67 using RT-PCR of mRNA from FFPE samples. It was developed to improve discrimination between luminal A and B subtypes.40 The accuracy of subtype classification with MammaTyper has not yet been compared with PAM50 or IHC, and it is not currently approved for use by the FDA.
BreastPRS
BreastPRS™ (Signal Genetics, Carlsbad, CA) is a molecular assay that uses an algorithm based on 200 genes sourced from a metaanalysis of publicly available genomic databases to stratify patients into groups at low or high risk for recurrence. It can use RNA extracted from either fresh-frozen or FFPE samples and was shown to be able to reclassify patients with intermediate Oncotype DX RS into low- and high-risk designations.41 It has not been validated in any further studies.
BreastOncPx
The Breast Cancer Prognosis Gene Expression Assay (BreastOncPx™, LabCorp, Burlington, NC) is a 14-gene RT-PCR assay that uses FFPE samples to assign patients with ER+ , LN− breast cancer a low-, moderate-, or high-risk metastasis score (MS) that represents an estimated risk of distant metastases at 10 years after diagnosis.42 It has not been validated in any further studies.
Conclusions
There is a substantial body of evidence to support use of genomic testing in clinical management of patients with breast cancer, and we believe that surgeons are well poised to initiate this testing, since we frequently represent the first treating providers encountered by patients following diagnosis with breast cancer. Judicious use of genomic testing in the context of multidisciplinary care has the potential to expedite time to treatment and improve personalization of care. Notably, however, a recent trial comparing the performance of Prosigna, Oncotype DX, MammaPrint, MammaTyper, the NexCourse IHC4 assay, and the conventional IHC4 assay demonstrated significant discordance in risk assessment, with approximately 60% of trial participants being assigned to different categories (high vs. intermediate/low).36 Thus, further investigation of the prognostic and predictive power of these tools needs to be pursued to help us collectively refine management of patients spanning the spectrum of breast malignancy from DCIS to metastatic disease. It will be important for surgeons to be not only a part of these investigations but also the standard-bearers for their application in clinical practice.
References
Joh JE, Esposito NN, Kiluk JV, et al. The effect of Oncotype DX recurrence score on treatment recommendations for patients with estrogen receptor-positive early stage breast cancer and correlation with estimation of recurrence risk by breast cancer specialists. Oncologist. 2011;16:1520–1526.
Paik S, Shak S, Tang G, et al. Multi-gene RT-PCR assay for predicting recurrence in node negative breast cancer patients–NSABP studies B-20 and B-14. Breast Cancer Res Treat. 2003;82:A16.
Cobleigh MA, Tabesh B, Bitterman P, et al. Tumor gene expression and prognosis in breast cancer patients with 10 or more positive lymph nodes. Clin Cancer Res. 2005;11:8623–8631.
Esteban J, Baker J, Cronin M, et al. Tumor gene expression and prognosis in breast cancer: multi-gene RT-PCR assay of paraffin-embedded tissue. Proc Am Soc Clin Oncol. 2003;22:850.
Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351:2817–2826.
Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol. 2006;24:3726–3734.
Rakovitch E, Nofech-Mozes S, Hanna W, et al. A population-based validation study of the DCIS Score predicting recurrence risk in individuals treated by breast-conserving surgery alone. Breast Cancer Res Treat. 2015;152:389–398.
Solin LJ, Gray R, Baehner FL, et al. A multigene expression assay to predict local recurrence risk for ductal carcinoma in situ of the breast. J Natl Cancer Inst. 2013;105(10):701–710.
Sparano JA, Gray RJ, Makower DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med. 2015;373:2005–2014.
Gluz O, Nitz UA, Christgen M, et al. West German Study Group Phase III PlanB Trial: first prospective outcome data for the 21-gene recurrence score assay and concordance of prognostic markers by central and local pathology assessment. J Clin Oncol. 2016;34(20): 2341–2349.
AJCC Cancer Staging Manual. Springer, New York; 2017.
Hayes DF. Targeting adjuvant chemotherapy: a good idea that needs to be proven! J Clin Oncol. 2012;30:1264–1267.
Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11:55–65.
Mamounas EP, Bryant J, Lembersky B, et al. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: results from NSABP B-28. J Clin Oncol. 2005;23:3686–3696.
Zanotti L, Bottini A, Rossi C, et al. Diagnostic tests based on gene expression profile in breast cancer: from background to clinical use. Tumor Biol. 2014;35:8461–8470.
Dabbs DJ, Klein ME, Mohsin SK, et al. High false-negative rate of HER2 quantitative reverse transcription polymerase chain reaction of the Oncotype DX test: an independent quality assurance study. J Clin Oncol. 2011;29:4279–4285.
Symmans WF, Wei C, Gould R, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35:1049–1060.
Yardley DA, Peacock NW, Shastry M, et al. A phase II trial of ixabepilone and cyclophosphamide as neoadjuvant therapy for patients with HER2-negative breast cancer: correlation of pathologic complete response with the 21-gene recurrence score. Breast Cancer Res Treat. 2015;154:299–308.
Bear HD, Wan W, Robidoux A, et al. Using the 21-gene assay from core needle biopsies to choose neoadjuvant therapy for breast cancer: a multicenter trial. J Surg Oncol. 2017;115:917–923.
Shak S, Petkov V, Miller D, et al. Abstract P5-15-01: breast cancer specific survival in 38,568 patients with node negative hormone receptor positive invasive breast cancer and oncotype DX recurrence score results in the SEER database. Cancer Res. 2016;76:P5–P15.
Stemmer S, Steiner M, Rizel S, et al. Abstract P5-08-02: Real-life analysis evaluating 1594 N0/Nmic breast cancer patients for whom treatment decisions incorporated the 21-gene recurrence score result: 5-year KM estimate for breast cancer specific survival with recurrence score results ≤ 30 is > 98%. Cancer Res. 2016;76:P5–08.
Mook S, Veer L, Rutgers EJT, et al. Individualization of therapy using Mammaprint®ì: from development to the MINDACT Trial. Cancer Genom Proteom. 2007;4:147–155.
van de Vijver MJ, He YD, van ‘t Veer LJ, et al. A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med. 2002;347:1999–2009.
Cardoso F, Piccart-Gebhart M, Van’t Veer L, Rutgers E. The MINDACT trial: The first prospective clinical validation of a genomic tool. Mol Oncol. 2007;1:246–251.
Liu J. Model Selection/Validation. In: Cosmatos D, Chow S-C (eds) Translational medicine: strategies and statistical methods. Boca Raton, FL: Chapman and Hall/CRC, Taylor & Francis Group; 2009.
Cardoso F, van’t Veer LJ, Bogaerts J, et al. 70-Gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375:717–729.
Drukker CA, Bueno-de-Mesquita JM, Retèl VP, et al. A prospective evaluation of a breast cancer prognosis signature in the observational RASTER study. Int J Cancer. 2013;133:929–936.
Bartlett JM, Thomas J, Ross DT, et al. Mammostrat® as a tool to stratify breast cancer patients at risk of recurrence during endocrine therapy. Breast Cancer Res. 2010;12:1–11.
Nielsen T, Wallden B, Schaper C, et al. Analytical validation of the PAM50-based prosigna breast cancer prognostic gene signature assay and nCounter Analysis System using formalin-fixed paraffin-embedded breast tumor specimens. BMC Cancer. 2014;14:1.
Ma XJ, Salunga R, Dahiya S, et al. A five-gene molecular grade index and HOXB13:IL17BR are complementary prognostic factors in early stage breast cancer. Clin Cancer Res. 2008;14:2601–2608.
Link JS, Buck LJ, Kapoor NS. The breast cancer index as a tool in decision making for adjuvant hormonal therapy in early luminal breast cancer: Initiation, withdrawal and continuance. In: Proceedings of the Thirty-Eighth Annual CTRC-AACR San Antonio Breast Cancer Symposium: 2015 Dec 8–12. Cancer Res. 2016;72: Abstract nr P5-08-10.
Dubsky P, Filipits M, Jakesz R, et al. EndoPredict improves the prognostic classification derived from common clinical guidelines in ER-positive, HER2-negative early breast cancer. Ann Oncol. 2013;24:640–647.
Gyorffy B, Hatzis C, Sanft T, et al. Multigene prognostic tests in breast cancer: past, present, future. Breast Cancer Res. 2015;17:11.
Liedtke C, Hatzis C, Symmans WF, et al. Genomic grade index is associated with response to chemotherapy in patients with breast cancer. J Clin Oncol. 2009;27:3185–3191.
Cuzick J, Dowsett M, Pineda S, et al. Prognostic value of a combined estrogen receptor, progesterone receptor, Ki-67, and human epidermal growth factor receptor 2 immunohistochemical score and comparison with the Genomic Health recurrence score in early breast cancer. J Clin Oncol. 2011;29:4273–4278.
Bartlett JM, Bayani J, Marshall A, et al. Comparing breast cancer multiparameter tests in the OPTIMA Prelim trial: no test is more equal than the others. J Natl Cancer Inst. 2016;108:djw050.
Haybittle JL, Blamey RW, Elston CW, et al. A prognostic index in primary breast cancer. Br J Cancer. 1982;45:361–366.
Rakha EA, Soria D, Green AR, et al. Nottingham prognostic index plus (NPI+): a modern clinical decision making tool in breast cancer. Br J Cancer. 2014;110:1688–1697.
Green AR, Soria D, Stephen J, et al. Nottingham prognostic index plus: validation of a clinical decision making tool in breast cancer in an independent series. J Pathol Clin Res. 2016;2:32–40.
Sinn P, Aulmann S, Wirtz R, et al. Multigene assays for classification, prognosis, and prediction in breast cancer: a critical review on the background and clinical utility. Geburtshilfe Frauenheilkd. 2013;73:932–940.
D’Alfonso TM, van Laar RK, Vahdat LT, et al. BreastPRS is a gene expression assay that stratifies intermediate-risk Oncotype DX patients into high- or low-risk for disease recurrence. Breast Cancer Res Treat. 2013;139:705–715.
Tutt A, Wang A, Rowland C, et al. Risk estimation of distant metastasis in node-negative, estrogen receptor-positive breast cancer patients using an RT-PCR based prognostic expression signature. BMC Cancer. 2008;8:339.
Acknowledgement
A version of this manuscript was published in The Breast: Comprehensive Management of Benign and Malignant Diseases. Ed. KI Bland, EM Copeland, VS Klimberg, WJ Gradishar. 5th ed. Philadelphia: Saunders, 2017.
Disclosure
Dr. Lucci-Speaker’s Bureau, Genomic Health, Inc.; Drs. Fayanju and Park-none.
Funding
Dr. Fayanju is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH) under Award Number 5KL2TR001115 (PI: Boulware) and by the NIH P30 Cancer Center Support Grant P30CA014236 (PI: Kastan) to the Duke Cancer Institute. The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fayanju, O.M., Park, K.U. & Lucci, A. Molecular Genomic Testing for Breast Cancer: Utility for Surgeons. Ann Surg Oncol 25, 512–519 (2018). https://doi.org/10.1245/s10434-017-6254-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-017-6254-z