
Abstract
Background
Randomized trials of radiation after breast-conserving surgery (BCS) for ductal carcinoma in situ (DCIS) found substantial rates of recurrence, with half of the recurrences being invasive. Decreasing local recurrence rates for invasive breast carcinoma have been observed and are largely attributed to improvements in systemic therapy. In this study, we examine recurrence rates after BCS for DCIS over 3 decades at one institution.
Methods
We retrospectively reviewed a prospectively maintained database of DCIS patients undergoing BCS from 1978 to 2010. Cox proportional hazard models were used to investigate the association between the treatment period and recurrence, controlling for other variables.
Results
Overall, 363 (12 %) recurrences among 2996 cases were observed. Median follow-up for patients without recurrence was 75 months (range 0–30 years); 732 patients were followed for ≥10 years. The 5-year recurrence rate for the period 1978–1998 was 13.6 versus 6.6 % for the period 1999–2010 [hazard ratio (HR) 0.62, p < 0.0001]. Controlling for age, family history, presentation, nuclear grade, necrosis, number of excisions, margin status, radiation, and endocrine therapy, treatment period remained significantly associated with recurrence, with later years associated with a lower HR (0.74, p = 0.02) compared to earlier. After stratification by radiation use, association of recurrence with treatment period persisted in those treated without radiation (HR 0.62, p = 0.003).
Conclusions
Recurrence rates for DCIS have fallen over time, with increases in screen detection, negative margins, and use of adjuvant therapies only partially explaining this decrease. The unexplained decline persists in women not receiving radiation, suggesting it is not due to changes in radiation efficacy but may be due to improvements in radiologic detection and pathologic assessment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Ductal carcinoma in situ (DCIS) accounts for over 20 % of all breast cancer diagnosed in the US annually.1 A 500 % increase in the incidence of DCIS between 1983 and 2003 was observed for women 50 years of age and older, likely due to screening mammography.2
Reported recurrence rates for DCIS treated with breast-conserving surgery (BCS) from four prospective randomized trials of radiation range from 26 to 36 % for those treated without radiation therapy, and from 9 to 23 % for those treated with radiation at 13–20 years of follow-up.3–6 These rates are higher than the 12-year ipsilateral breast tumor recurrence rates of 5–8 % for node-negative invasive breast cancer treated with radiation and systemic therapy.7
Local recurrence rates in early invasive cancer have declined over time,8–11 which has been attributed, at least in part, to advances in systemic therapy for invasive cancer.12
Temporal trends in DCIS recurrence are less well-studied. In this current study, we sought to examine changes in recurrence rates over time among women treated with BCS for DCIS, and to explore the reasons for the changes found.
Materials and Methods
After obtaining Institutional Review Board approval, we analyzed outcomes from a prospectively maintained database of DCIS patients undergoing BCS from 1978 to 2010 at the Memorial Sloan Kettering Cancer Center. Synchronous (n = 30) or metachronous 77 (n = 29) bilateral DCIS were entered as separate cases. Follow-up was routinely obtained by yearly contact with the patient, at follow-up clinician visits, or by mail, phone, or e-mail.
Variables examined included age at diagnosis, menopausal status (pre- or perimenopausal vs. postmenopausal), family history (at least one first- or second-degree family member with breast cancer), radiologic versus clinical presentation of DCIS, nuclear grade (non-high grade vs. high grade), necrosis, number of excisions (≤2 vs. ≥3), margin status [positive or close (≤2 mm) vs. negative (>2 mm)], radiation, endocrine therapy, and year of definitive surgery.
An event was defined as ipsilateral breast recurrence of DCIS or invasive cancer, ipsilateral regional recurrence in the absence of breast recurrence, or distant recurrence in the absence of locoregional recurrence or diagnosis of other malignancy. Time to recurrence was defined as the length of time between the last surgical excision and first event. Kaplan–Meier curves were created to compare recurrence rates by treatment period, and log-rank tests were used to determine significance. Patient, pathological, and treatment variables were compared between treatment periods using χ 2 analysis. The Cochran–Armitage test was used to test for trend in the proportion of women undergoing BCS versus mastectomy over time. Multivariable Cox models were built to examine differences in recurrence rates over time, controlling for other variables. Proportionality of hazards was checked for all Cox models and found to be appropriate. Statistical analysis was performed using SAS 9.2 (SAS Institute, Cary, NC, USA).
Results
From 1978 to 2010, a total of 2996 cases of DCIS treated with BCS were identified. Population characteristics are shown in Table 1. Patients without recurrence were followed for a median of 75 months (range 0–30 years); 732 were followed for at least 10 years. The median age of the entire population, and for the cohorts from both the early and late treatment periods, was 57 years (range 20–92 years).
Among the 1374 patients who underwent BCS alone, there were 223 recurrences, of which 117 were ipsilateral breast recurrences of DCIS, 98 were invasive (91 ipsilateral breast recurrences, two ipsilateral regional nodal recurrences, five ipsilateral breast and nodal recurrences), and 8 were ipsilateral breast recurrence of unknown type.
Among the 1588 patients who underwent BCS and radiation, there were 140 recurrences, of which 75 were ipsilateral breast recurrences of DCIS, 61 were invasive (56 ipsilateral breast recurrences, five ipsilateral breast and nodal recurrences), three were ipsilateral breast recurrence of unknown type, and there was a single case of distant metastasis without ipsilateral locoregional recurrence or diagnosis of other malignancy.
Recurrence Rates Over Time
Figure 1a shows recurrence rates by treatment period, dividing the study interval into six treatment periods. A significant decrease in recurrence rates over time was observed (p = 0.001). The change over time appeared non-linear, with an apparent break between the three earlier intervals and the three later intervals; we therefore dichotomized the treatment period into intervals of 1978–1998 and 1999–2010 for further analysis. Figure 1b shows a decline in 5-year recurrence rates from 13.6 % [95 % confidence interval (CI) 11.3–16.3] in 1978–1998 to 6.6 % (95 % CI 5.5–7.9) in 1999–2010 (p < 0.0001), with a hazard ratio (HR) of 0.62 (p < 0.0001) in the later period compared with the earlier period.

Proportion recurrence-free, by year of surgery for a six treatment periods; b two treatment periods; c breast-conserving surgery alone over two treatment periods; and d breast-conserving surgery with radiation over two treatment periods. HR hazard ratio, † indicates p value for difference compared with 1978–1990, ‡ indicates p value for difference compared with 1978–1998
Change in Patient, Tumor, and Treatment Variables Over Time
Patient, tumor, and treatment variables were compared between the dichotomized treatment periods to identify factors potentially contributing to the reduction in recurrence (Table 1).
For nearly all variables, there were more missing data from the earlier time period. In the more recent time period, family history was more frequently recorded as positive, patients more frequently presented as a result of radiologic screening, nuclear grade was less frequently rated as high, more women underwent at least three excisions to enable breast conservation, close margins were less frequent, and adjuvant radiation and endocrine therapies were more commonly used. Age at diagnosis, menopausal status, and the presence of necrosis did not change over time.
Multivariable Analysis
Recurrence rates by treatment period were compared using a multivariable model to control for known risk factors and the factors that changed over time (Table 2). Even after controlling for nine variables from Table 1, the later time period was associated with a lower risk of recurrence, with an HR of 0.74 compared with the earlier period (p = 0.02). The persistent association of time period with recurrence, even after controlling for other variables, indicates that increases in screen detection, negative margins, and use of radiation and endocrine therapies do not fully explain the decrease in recurrence rates observed over time.
Change in Recurrence Rates Over Time, Stratified by Use of Radiation
To determine whether the unexplained decline in recurrence occurred in patients treated with and without radiotherapy, we fit multivariable models stratified by radiation use (Table 3). This analysis demonstrated that the decrease in recurrence rates over time, not accounted for by change in other variables, was limited to the group not receiving radiation (HR for treatment period 0.62, p = 0.003), suggesting that improvement in radiation efficacy is not the primary cause of the observed decrease in recurrence rates.
Rates of Total Mastectomy Versus Breast-Conserving Surgery for Ductal Carcinoma In Situ
We compared annual rates of BCS versus mastectomy for DCIS at our institution from 1995 to 2010 to evaluate the possibility that decreased recurrence rates were due to selection bias. There was no significant change over time in the percentage of patients undergoing mastectomy for DCIS (40.1 % in 1995–1998 vs. 40.4 % in 1999–2010, p = 0.85) (Fig. 2).

Proportion and number of DCIS cases undergoing breast-conserving surgery versus therapeutic mastectomy, by year. Proportion of each bar shaded blue or yellow represents the proportion of all cases of DCIS that were treated with breast-conserving surgery or mastectomy, respectively, each year. The number treated by each type of surgery is shown overlying the appropriate portion of the bar. DCIS ductal carcinoma in situ
Discussion
Several groups have reported decreasing locoregional recurrence rates for invasive cancer.8–11 These improvements are largely attributed to improved systemic treatments, including chemotherapy, targeted anti-HER2 therapies, and endocrine therapies. In contrast, in DCIS, the only proven systemic therapy is endocrine therapy; use of endocrine therapy in DCIS is relatively low,13 suggesting that a similar decline in rates of locoregional recurrence might not have occurred.
We undertook this study to examine recurrence rates for DCIS treated with BCS over 30 years at a single institution. Examination of outcomes from 2996 cases revealed that recurrence rates significantly declined over time. We identified a number of temporal trends in our population which helped to explain this outcome.
Patients treated in later years more frequently presented with radiologically detected DCIS, and screen-detected DCIS is associated with lower rates of recurrence than cases presenting clinically, likely due to a lower volume of disease.4,5,14 While it is likely that the pathologically measured size of DCIS would have been smaller in later years, measured pathologic size was not available for the majority of our cases. This is due to the difficulty of accurate measurement of DCIS, which is generally not grossly visible. Size measurements were also missing in the majority of cases in the four prospective randomized trials.15 In the later treatment period, an increased proportion of patients underwent at least three surgical excisions, which may reflect a greater effort to achieve margins > 2 mm in the later treatment period, as demonstrated by the decrease in the proportion of women with close or positive margins. It is likely this contributed to the observed decline in recurrence rates as margin status is a known risk factor for local recurrence.4–6 Alternatively, it may reflect greater comfort with BCS for larger areas of DCIS in women who might have been advised to undergo mastectomy in prior years.
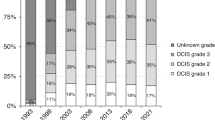
Over the study period, the proportion of cases with high nuclear grade fell from 49 % of those with known nuclear grade to 32 %. A similar decrease in the proportion of patients with high-grade DCIS was reported by Habel et al.16 Although studies have shown that local recurrence at 5 years is more common in patients with high-grade DCIS, these differences do not persist with longer follow-up.17,18 In our multivariable analysis, high nuclear grade was not associated with local recurrence, similar to findings in other studies with longer follow-up.17
We also found that patients treated in later years were significantly more likely to receive adjuvant radiation. Patients from the early years of this series were treated prior to publication of the first randomized trial of radiation for DCIS [the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-17] in 1993.19 The increasing use of radiation over time is well documented.13,16,20 Baxter et al. and Zujewski et al. have reported increased use of radiation for DCIS in the Surveillance, Epidemiology, and End Results Program of the National Cancer Institute (SEER) database.13,20 In the community setting, Habel et al. also found an increase in the use of radiation for the treatment of DCIS—from 25.8 % in 1990–1991 to 61.3 % in 2000–2001.16 Four prospective randomized studies have been published with over 12 years of follow-up, proving that radiation provides a durable reduction in local recurrence rates of approximately 50 %.3–6 Therefore, one clear reason for the observed decrease in recurrence rate in our series is the increased use of radiation.
Use of endocrine therapy also increased significantly over time, likely contributing to the decrease in recurrence rates. NSABP B-24, first published in 1999, was the first randomized study of tamoxifen use in women with DCIS treated with radiation.21 As a result of that study, and the UK/ANZ trial, the use of tamoxifen for DCIS increased.3,13,21 Habel et al. noted an increase in tamoxifen use from 2 % among those diagnosed in 1990–1991 to 34 % among those diagnosed in 2000–2001.16 Hiramatsu et al. and Halasz et al. reported that none of 76 patients treated prior to 1990 received endocrine therapy compared with 126 of 246 patients treated from 2001 to 2007.22,23
After adjustment for all factors that changed over time, including radiologic detection, negative margins, and use of adjuvant radiation and endocrine therapies, all of which clearly influence rates of recurrence, we found that the later treatment period remained significantly associated with a lower risk of recurrence. This suggests that factors not included in our model contributed to the reduction in recurrence risk. One possibility is improved efficacy of adjuvant radiotherapy. However, after stratifying for use of radiation, the unexplained decline in recurrence rate was limited to those not receiving radiation, suggesting that improvement in radiation efficacy is not responsible for the observed decline in recurrence rates.
Others have also reported a decline in local recurrence rates for DCIS treated with BCS. Halasz et al. compared the results of a series of 246 women treated with BCS and radiation from 2001 to 2007, with a median follow-up of 58 months (5-year recurrence rate, 0 %) with a series of 76 patients treated from 1976 to 1990, with a median follow-up of 74 months (10-year recurrence rate, 15 %), and concluded that recurrence rates had significantly improved in the modern era of mammographic detection and careful attention to margins.22,23 Similarly, Habel et al. reported a reduction in the 5-year local recurrence rate from 14.3 to 7.7 % in patients diagnosed in 1990–1991 compared with those diagnosed in 1998–1999.16 Similar to our observation, these investigators found that even after adjustment for adjuvant radiation and endocrine therapy use, there remained a reduced risk of recurrence in the later years. They also noted an increase in the frequency of negative margins and non-high-grade DCIS. These factors were not included in their multivariable model, and they hypothesized that the increase in negative margins and non-high-grade DCIS contributed to the decreased recurrence rates. However, in our analysis, even after inclusion of these factors in a multivariable model, treatment period remained significantly associated with a reduced recurrence risk.
Factors potentially responsible for the improved outcomes we observed and which we were unable to study include improvements in breast imaging and pathologic evaluation. Digital mammography, compared with film screen, is better able to detect faint microcalcifications,24–27 which may lead to earlier detection and to more complete excision of DCIS lesions, thereby improving recurrence rates.
Pathologic assessment of DCIS has changed over time, with an increased number of slides examined per case as well as standardized reporting with regard to extent of disease and margin status.28–30 The report of a negative margin in more recent years, after a more intensive pathologic examination, may indicate a lower burden of residual disease and result in lower recurrence rates.
Our findings have important implications for patients being treated in the modern era. The meta-analysis of the four randomized trials of BCS with and without radiation for DCIS reported a 5-year ipsilateral recurrence rate of 18 % in patients undergoing BCS alone.15 These trials began between 1985 and 1990. Our results suggest that current rates of local recurrence are substantially lower. Newer prospective studies support this contention, albeit in favorable subsets of patients.
McCormick et al. reported 5-year recurrence rates of 0.4 % among those randomized to radiation, and 3.5 % among those randomized to no radiation, in selected low-risk women with DCIS treated from 1999 to 2006.31 Two single-arm prospective studies have evaluated BCS without radiation for selected women treated in a more recent time period. Both required ≤2.5 cm of DCIS and widely negative inked margins. Wong et al. accrued patients between 1995 and 2002, and reported 5-year recurrence rates of 9.8 %.32 Hughes et al. accrued patients from 1997 to 2002 and reported 5-year recurrence rates of 6.1 % for low/intermediate-grade DCIS, and 15.3 % for high-grade DCIS.18
Although they represent selected populations, these rates are reassuringly lower than those from the first four randomized trials, and are consistent with our finding that recurrence rates have declined. The lower recurrence risk estimate for patients treated in recent years can be critical when counseling patients, especially in this era of increased use of uni- and bilateral mastectomy.33,34 An online risk estimation tool, which incorporates various factors, including year of treatment, has been validated in independent populations and may be helpful for patients and clinicians in weighing various treatment options and in obtaining more current and individualized risk estimates (http://nomograms.mskcc.org/Breast/DuctalCarcinomaInSituRecurrencePage.aspx).35–39
Conclusions
Recurrence rates after BCS for DCIS have declined over time. The increased proportion of patients with screen-detected DCIS, negative margins, and the increased use of radiation and endocrine therapies, only partly explains decreased recurrence rates. Advances in digital mammography and improvements in pathological assessment likely result in earlier detection and more complete resection, and thereby contribute to the reduction in recurrences seen in recent years. The expected recurrence rate for a woman treated today may be lower than that seen in the prospective randomized trials that began decades ago. This has implications for patient decision making, especially in view of the marked increase in recent years of the number of women choosing unilateral or bilateral mastectomy for treatment of their DCIS.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5–29.
Kerlikowske K. Epidemiology of ductal carcinoma in situ. J Natl Cancer Inst Monogr. 2010;2010(41):139–41.
Cuzick J, Sestak I, Pinder SE, et al. Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: long-term results from the UK/ANZ DCIS trial. Lancet Oncol. 2011;12(1):21–9.
Donker M, Litiere S, Werutsky G, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma in situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J Clin Oncol. 2013;31(32):4054–9.
Wapnir IL, Dignam JJ, Fisher B, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103(6):478–88.
Warnberg F, Garmo H, Emdin S, et al. Effect of radiotherapy after breast-conserving surgery for ductal carcinoma in situ: 20 years follow-up in the randomized SweDCIS Trial. J Clin Oncol. 2014;32(32):3613–8.
Anderson SJ, Wapnir I, Dignam JJ, et al. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in patients treated by breast-conserving therapy in five National Surgical Adjuvant Breast and Bowel Project protocols of node-negative breast cancer. J Clin Oncol. 2009;27(15):2466–73.
Cabioglu N, Hunt KK, Buchholz TA, et al. Improving local control with breast-conserving therapy: a 27-year single-institution experience. Cancer. 2005;104(1):20–9.
Canavan J, Truong PT, Smith SL, Lu L, Lesperance M, Olivotto IA. Local recurrence in women with stage I breast cancer: declining rates over time in a large, population-based cohort. Int J Radiat Oncol Biol Phys. 2014;88(1):80–6.
Mannino M, Yarnold JR. Local relapse rates are falling after breast conserving surgery and systemic therapy for early breast cancer: can radiotherapy ever be safely withheld? Radiother Oncol. 2009;90(1):14–22.
Ernst MF, Voogd AC, Coebergh JW, Poortmans PM, Roukema JA. Using loco-regional recurrence as an indicator of the quality of breast cancer treatment. Eur J Cancer. 2004;40(4):487–93.
Morrow M, Harris JR, Schnitt SJ. Surgical margins in lumpectomy for breast cancer–bigger is not better. N Engl J Med. 2012;367(1):79–82.
Zujewski JA, Harlan LC, Morrell DM, Stevens JL. Ductal carcinoma in situ: trends in treatment over time in the US. Breast Cancer Res Treat. 2011;127(1):251–7.
Collins LC, Achacoso N, Haque R, et al. Risk factors for non-invasive and invasive local recurrence in patients with ductal carcinoma in situ. Breast Cancer Res Treat. 2013;139(2):453–60.
Early Breast Cancer Trialists’ Collaborative Group, Correa C, McGale P, et al. Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. J Natl Cancer Inst Monogr. 2010;2010(41):162–77.
Habel LA, Achacoso NS, Haque R, et al. Declining recurrence among ductal carcinoma in situ patients treated with breast-conserving surgery in the community setting. Breast Cancer Res. 2009;11(6):R85.
Solin LJ, Kurtz J, Fourquet A, et al. Fifteen-year results of breast-conserving surgery and definitive breast irradiation for the treatment of ductal carcinoma in situ of the breast. J Clin Oncol. 1996;14(3):754–63.
Hughes LL, Wang M, Page DL, et al. Local excision alone without irradiation for ductal carcinoma in situ of the breast: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol. 2009;27(32):5319–24.
Fisher B, Costantino J, Redmond C, et al. Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med. 1993;328(22):1581–6.
Baxter NN, Virnig BA, Durham SB, Tuttle TM. Trends in the treatment of ductal carcinoma in situ of the breast. J Natl Cancer Inst. 2004;96(6):443–8.
Fisher B, Dignam J, Wolmark N, et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet. 1999;353(9169):1993–2000.
Hiramatsu H, Bornstein BA, Recht A, et al. Local recurrence after conservative surgery and radiation therapy for ductal carcinoma in situ: possible importance of family history. Cancer J Sci Am. 1995;1(1):55–61.
Halasz LM, Sreedhara M, Chen YH, et al. Improved outcomes of breast-conserving therapy for patients with ductal carcinoma in situ. Int J Radiat Oncol Biol Phys. 2012;82(4):e581–6.
Feeley L, Kiernan D, Mooney T, et al. Digital mammography in a screening programme and its implications for pathology: a comparative study. J Clin Pathol. 2011;64(3):215–9.
Karssemeijer N, Bluekens AM, Beijerinck D, et al. Breast cancer screening results 5 years after introduction of digital mammography in a population-based screening program. Radiology. 2009;253(2):353–8.
Hambly NM, McNicholas MM, Phelan N, Hargaden GC, O’Doherty A, Flanagan FL. Comparison of digital mammography and screen-film mammography in breast cancer screening: a review in the Irish breast screening program. AJR Am J Roentgenol. 2009;193(4):1010–8.
Del Turco MR, Mantellini P, Ciatto S, et al. Full-field digital versus screen-film mammography: comparative accuracy in concurrent screening cohorts. AJR Am J Roentgenol. 2007;189(4):860–6.
Miller KL, Marks LB, Barrier RC Jr, et al. Increased sectioning of pathologic specimens with ductal carcinoma in situ of the breast: are there clinical consequences? Clin Breast Cancer. 2003;4(3):198–202.
Lester SC, Bose S, Chen YY, et al. Protocol for the examination of specimens from patients with ductal carcinoma in situ of the breast. Arch Pathol Lab Med. 2009;133(1):15–25.
Siziopikou KP. Ductal carcinoma in situ of the breast: current concepts and future directions. Arch Pathol Lab Med. 2013;137(4):462–6.
McCormick B, Winter K, Hudis C, et al. RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J Clin Oncol. 2015;33(7):709–15.
Wong JS, Chen YH, Gadd MA, et al. Eight-year update of a prospective study of wide excision alone for small low- or intermediate-grade ductal carcinoma in situ (DCIS). Breast Cancer Res Treat. 2014;143(2):343–50.
Rutter CE, Park HS, Killelea BK, Evans SB. Growing use of mastectomy for ductal carcinoma-in situ of the breast among young women in the United States. Ann Surg Oncol. 2015;22(7):2378–86.
Tuttle TM, Jarosek S, Habermann EB, et al. Increasing rates of contralateral prophylactic mastectomy among patients with ductal carcinoma in situ. J Clin Oncol. 2009;27(9):1362–7.
Memorial Sloan Kettering Cancer Center. Breast cancer nomogram: ductal carcinoma in situ recurrence. 2014. http://nomograms.mskcc.org/Breast/DuctalCarcinomaInSituRecurrencePage.aspx. Accessed 8 Apr 2015.
Rudloff U, Jacks LM, Goldberg JI, et al. Nomogram for predicting the risk of local recurrence after breast-conserving surgery for ductal carcinoma in situ. J Clin Oncol. 2010;28(23):3762–9.
Sweldens C, Peeters S, van Limbergen E, et al. Local relapse after breast-conserving therapy for ductal carcinoma in situ: a European single-center experience and external validation of the Memorial Sloan-Kettering Cancer Center DCIS nomogram. Cancer J. 2014;20(1):1–7.
Wang F, Li H, Tan PH, et al. Validation of a nomogram in the prediction of local recurrence risks after conserving surgery for Asian women with ductal carcinoma in situ of the breast. Clin Oncol. 2014;26(11):684–91.
Collins LC, Achacoso N, Haque R, et al. Risk prediction for local breast cancer recurrence among women with DCIS treated in a community practice: a nested case-control study. Ann Surg Oncol. 2015. doi:10.1245/s10434-015-4641-x.
Acknowledgment
This study was funded in part by National Institutes of Health, National Cancer Center Support Grant P30 CA008748.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Subhedar, P., Olcese, C., Patil, S. et al. Decreasing Recurrence Rates for Ductal Carcinoma In Situ: Analysis of 2996 Women Treated with Breast-Conserving Surgery Over 30 Years. Ann Surg Oncol 22, 3273–3281 (2015). https://doi.org/10.1245/s10434-015-4740-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4740-8