
Abstract
Background
Inflammatory breast cancer (IBC) is a rare and aggressive subtype. This study analyzes the patterns of failure in patients with IBC treated at our institution.
Methods
We retrospectively analyzed the records of 227 women with IBC presenting between 1997 and 2011. Survival analysis was used to calculate overall survival (OS) and disease-free survival. Competing risk analysis was used to calculate locoregional recurrence (LRR).
Results
A total of 173 patients had locoregional-only disease at presentation (non-MET). Median follow-up in the surviving patients was 3.3 years. Overall, 132 (76.3 %) patients received trimodality therapy with chemotherapy, surgery, and radiotherapy. Three-year OS was 73.1 % [95 % confidence interval (CI) 64.9–82.4]. Cumulative LRR was 10.1, 16.9, and 21.3 % at 1, 2, and 3 years, respectively. No variable was significantly associated with LRR. Fifty-four patients had metastatic disease at presentation (MET). Median follow-up in the surviving patients was 2.6 years. Three-year OS was 44.3 % (95 % CI 31.4–62.5). Twenty-four (44.4 %) patients received non-palliative local therapy (radiotherapy and/or surgery). For these patients, median OS after local therapy was 2 years. Excluding six patients who received local therapy for symptom palliation, the crude incidence of locoregional progression or recurrence (LRPR) was 17 % (4/24) for those who received local therapy compared with 57 % (13/23) for those who did not.
Conclusions
For non-MET patients, LRR remains a problem despite trimodality therapy. More aggressive treatment is warranted. For MET patients, nearly 60 % have LRPR with systemic therapy alone. Local therapy should be considered in the setting of metastatic disease to prevent potential morbidity of progressive local disease.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Inflammatory breast cancer (IBC) is a rare but aggressive subtype of invasive breast cancer. It is diagnosed clinically, defined by a history of rapid onset of erythema involving a third or more of the breast, edema, and/or peau d’orange, and pathologic confirmation of invasive carcinoma.1,2 IBC is associated with a significantly younger age at diagnosis, decreased likelihood of estrogen receptor (ER) expression, higher cumulative incidence of locoregional recurrence (LRR) and distant soft-tissue disease, and worse overall survival (OS) when compared with non-inflammatory locally advanced breast cancer (LABC).3–5 It is likely that these clinical patterns are a result of differing underlying biology, including higher expression of pro-angiogenic factors and overexpression of cell adhesion molecules.3,6–9 LRR in patients with IBC is estimated to be between 10 and 27 %, compared with between 7 and 10 % for LABC.3,10–14 Five-year OS rates for patients with IBC presenting without metastatic disease range from 40–61 %, compared with 41–86 % in LABC.10,13–21
The current standard of care for newly diagnosed, non-metastatic IBC includes preoperative chemotherapy, including a trastuzumab-based regimen for human epidermal growth factor receptor 2 (HER2)-positive patients, modified radical mastectomy, adjuvant radiotherapy, including the chest wall and regional lymph nodes and, if ER- or progesterone receptor (PR)-positive, endocrine therapy.15,22,23 Limited research regarding local therapy in the setting of metastatic IBC has been conducted.24,25 Current National Comprehensive Cancer Network Guidelines and international expert panel recommendations do not address the role for local therapy in this population.2,26 As in the non-metastatic cohort, improved locoregional control could decrease the morbidity associated with locoregional progression or recurrence (LRPR). Additionally, recent retrospective literature suggesting improved survival in patients with metastatic inflammatory and non-inflammatory breast cancer who undergo local therapy compels further research in this cohort.25,27–29
In this analysis, we retrospectively examined the patterns of disease failure in a cohort of 227 women presenting to the Dana-Farber Cancer Institute/Brigham and Women’s Hospital with a diagnosis of IBC. We examined two subgroups of patients, those with (n = 54, 23.8 %) and without (n = 173, 76.2 %) metastatic disease on presentation.
Methods and Patients
Patients
This retrospective review was approved by the Dana-Farber/Harvard Cancer Center Institutional Review Board. Eligible patients included those with documented IBC diagnosed between 1 January 1997 and 31 December 2011. To be eligible for inclusion, the documented clinical presentation needed to be consistent with the American Joint Committee on Cancer and the International Union for Cancer Control (AJCC/UICC) and International Expert Consensus diagnostic criteria.1,2 Patients were not required to have documented pathologic evidence of dermal lymphatic involvement. Patients (n = 8; five metastatic at presentation, three locoregional-only at presentation) who developed IBC after an initial diagnosis of non-inflammatory disease (secondary or recurrent IBC) were included, given their similar disease prognosis and OS as those patients with primary IBC.30–32 The 31 December 2011 end date was selected to allow all patients a potential 2-year follow-up period.
Patients were deemed clinically node-positive on initial presentation if they had palpable lymph nodes or abnormally enlarged lymph nodes based on available radiographic studies. Pathologic complete response (pCR) was defined as no residual invasive disease in the breast and resected lymph nodes at the time of surgery. We performed a subgroup analysis on 132 patients, all of whom had completed trimodality therapy, which was defined as receipt of first-line chemotherapy (with or without HER2-directed therapy), modified radical mastectomy, and radiotherapy (TRIMOD). Any sequence was permitted as long as all three modalities were utilized. Those patients whose initial response to preoperative chemotherapy did not permit surgery, and therefore completed a second course of systemic therapy prior to definitive surgery, were excluded from this group.
Statistical Analysis
Disease-free survival (DFS) and OS were estimated using the Kaplan–Meier method,33 and 95 % confidence intervals (CI) were estimated using Greenwood’s formula.34 Competing risk analysis35 was used to estimate LRR-free survival in the TRIMOD cohort and LRPR-free survival for the MET cohort. In these analyses, death was treated as a competing risk. If no events were observed, survival times were censored at the date patients were last known to be alive. Of note, the distinction was made between LRR in the non-metastatic cohort and LRPR in the metastatic cohort in an effort to emphasize the group of patients who could have persistent locoregional disease, i.e. disease remaining in the retained breast following the completion of systemic therapy with or without radiation therapy, as opposed to those patients who completed trimodality therapy and were presumed to have no tumor remaining at the completion of definitive therapy. For this reason, LRR-free survival and LRPR-free survival for the trimodality group and MET group were calculated from the completion of trimodality therapy and diagnosis, respectively.
Competing risk regression36 was used to examine which variables were associated with the occurrence of LRR or LRPR (regardless of its occurrence before or after distant disease recurrence). Death was a competing risk in these models. Univariate regressions were performed using several patient, tumor and treatment variables. Variables with p < 0.25 in the univariate model were included in multivariate models. Stepwise regression procedures were used for model selection.37 Fisher’s exact test was used to identify whether any baseline characteristics were associated with receipt of local treatment in the MET cohort. All statistical tests were two-sided, with p values <0.05 considered significant.
Results
Patients with Locoregional-Only Disease at Presentation
Patient, tumor, and treatment characteristics are listed in Table 1. A total of 173 patients with locoregional disease only (non-MET) met the inclusion criteria. Of this cohort, 66 patients have died and the median follow-up of the surviving patients was 3.3 years (range 0.2–14.6 years). Median OS from diagnosis was 7.3 years (95 % CI 5.2–inf.). Three- and 5-year OS was 78.3 % (95 % CI 71.8–85.2) and 59.6 % (95 % CI 51.3–69.1), respectively. Of these 173 patients, 41 did not complete the intended course of multimodality therapy due to poor disease response. The most common reasons for exclusion included receipt of second-line chemotherapy due to inadequate initial response (n = 15, 37 %), disease progression prior to definitive surgery (n = 10, 24 %), and disease progression during adjuvant therapy (n = 11, 27 %).
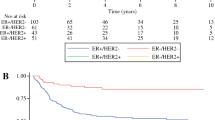
Among the 173 patients, 132 (76.3 %) met the criteria for inclusion in the trimodality subgroup. Two of these 132 patients had no documentation regarding LRR; therefore, 130 patients were analyzed in the TRIMOD cohort. Median OS from trimodality treatment completion was 8.6 years in this subgroup. Three-year OS was 73.1 % (95 % CI 64.9–82.4) and 5-year OS was 58.1 % (95 % CI 48.4–69.7). Median DFS after completion of trimodality therapy was 2.7 years (95 % CI 2.0–6.9). Three- and 5-year DFS was 47.7 % (95 % CI 39.2–58.0) and 41.0 % (95 % CI 32.4–52.0), respectively. All patients in the TRIMOD cohort underwent modified radical mastectomy. Two patients (1.5 %) had positive deep margins on final pathology. The cumulative incidence of LRR was 10.1, 16.9, and 21.3 % at 1, 2, and 3 years, respectively (Fig. 1). Univariate competing risk regression analysis did not identify any factors significantly associated with LRR in the TRIMOD cohort (Table 2), although several variables showed a marginally significant association with an increased risk of LRR, including higher tumor grade (p = 0.09), lack of pCR (p = 0.10), and residual lymphovascular invasion (LVI) at the time of surgery (p = 0.08). Tumor grade and pCR were included in the final multivariate competing risk regression model after stepwise selection. Neither variable was significant in the multivariate model (all p > 0.05).

Cumulative incidence of local failure in patients stratified by extent of disease at presentation. a Cumulative incidence of LRR in patients without metastatic disease at presentation who completed definitive trimodality therapy. Blue line represents the incidence of LRR, and the yellow line represents the competing risk of death. b Cumulative incidence of LRPR in patients with metastatic disease at presentation. Blue line represents the incidence of LRPR, and the yellow line represents the competing risk of death. LRR locoregional recurrence, LRPR locoregional progression or recurrence
Among the TRIMOD cohort, 50 patients (38.5 %) had HER2+ disease. The cumulative LRR incidence rate was 10.0, 12.2, and 17.8 % at 1, 2, and 3 years, respectively. In the subgroup that received HER2-directed therapy (n = 42, 84 %), the cumulative LRR incidence rate was 9.6, 12.3, and 16.0 % at 1, 2, and 3 years. In the subgroup that did not receive HER2-directed therapy (n = 8, 16 %), the cumulative LRR incidence rate was 12.5, 12.5, and 25 % at 1, 2, and 3 years. The receipt of HER2-directed therapy in patients with HER2-positive disease was not significantly associated with improved LRR (p = 0.53).
Patients with Metastatic Disease at Presentation
Fifty-four patients with metastatic disease at presentation (MET) were identified. Of these, 32 have died and the median follow-up of the surviving patients was 2.6 years (range 0.4–12.7 years). Median OS from diagnosis was 2.9 years (95 % CI 2.2–5.2). Three- and 5-year OS was 44.3 % (95 % CI 31.4–62.5) and 33.0 % (95 % CI 20.3–53.7). Of the 54 patients, one patient had unknown LRPR status; 53 patients were therefore included in the analysis. The cumulative incidence of LRPR was 30.5, 38.2, and 38.2 % at 1, 2, and 3 years, respectively (Fig. 1). Table 3 shows the results of the univariate and multivariate analyses examining predictors of LRPR. Patients with metastatic disease in non-locoregional lymph nodes (i.e. contralateral axilla, mediastinum) were more likely to have LRPR (p = 0.03). Tumor subtype was marginally associated with the occurrence of LRPR (p = 0.07). Patients with HER2+ disease were less likely to have LRPR than those with ER+ or PR+/HER2− or ER−/PR−/HER2− disease. Only two variables remained in the final multivariate competing risk regression model after stepwise selection: the presence of metastatic disease in non-locoregional lymph nodes at presentation (p = 0.05), and tumor subtype (p = 0.13).
In the MET cohort, 24 patients received local treatment (surgery and/or radiation therapy), 23 did not receive local treatment, six received palliative local treatment, defined as local treatment documented as recommended for symptom control (i.e. bleeding or pain from local tumor progression), and one had unknown local treatment information. Patients with grade II disease were more likely to receive local treatment for disease control than patients with grade III disease [odds ratio (OR) 6.1, 95 % CI 1.0–68.0; p = 0.03] (Table 4). There was a marginally significant trend for those with bone-only metastases at presentation to receive local therapy more often than those with other sites of distant metastases (p = 0.08). Of the 24 patients receiving non-palliative local therapy, 14 patients received surgery and radiotherapy, 3 received surgery but not radiotherapy, and 7 received radiotherapy but not surgery. The median survival after receipt of local therapy was 2 years (95 % CI 1.5–inf.). The cumulative incidence of LRPR and 1-year distant progression-free survival was 17.6 % and 41.8 % (95 % CI 25.5–68.5) 1 year after competing local therapy, respectively. Among the remaining 29 patients presenting with metastases, the cumulative incidence of LRPR and distant progression was 48.3 and 67.9 %, respectively, at 1-year after disease diagnosis.
Discussion
The current study retrospectively examined the patterns and predictors of locoregional and distant failure in a cohort of 227 women with IBC treated at a single institution from 1997 to 2011. Locoregional failure in IBC is of particular interest due to its associated morbidity and potential association with OS for those without metastatic disease who undergo multimodality therapy.19,22 This series, to our knowledge, represents the second largest single institution study examining the outcomes of patients with IBC undergoing trimodality therapy. By specifically presenting data on a cohort of patients who successfully completed trimodality therapy, we were able to study a homogenous patient population with results comparable to other published series and relevant to modern clinical care. The 3-year rate of LRR in our study (21.3 %) was consistent with other published results.13,14,17–19,38 This study did not identify any variables significantly associated with LRR in those patients receiving definitive trimodality therapy; however, there was a non-significant association between tumor grade, residual LVI, and pCR and LRR. Other studies analyzing predictors of LRR in women with IBC identified the number of positive lymph nodes, clinical response to chemotherapy, and surgical margin status as being significantly associated with LRR.13,18 Given the uniformity of surgical procedure and margin status in our patient cohort, we were unable to evaluate the impact of either of these variables on LRR.
While predictors of local failure are not consistent across studies, and analyses are limited by small numbers of events, response to chemotherapy predicts LRR in our study and others.13,18 Those patients with an incomplete pathologic response may be candidates for more aggressive local therapy. However, the means by which to escalate local therapy, whether by radiation approach, specifically with dose escalation or altered fractionation patterns, or by more aggressive surgery, remains unknown and should be the topic of further research.
This study also examined the locoregional outcomes in patients presenting with metastatic disease. In particular, in those patients who underwent surgery and post-mastectomy radiotherapy, our 5-year locoregional control rate was 83 %. Similarly, Takiar et al. found that patients with metastatic disease who received surgery and post-mastectomy radiotherapy had a 5-year locoregional control rate of 86 %.24 Akay et al. also found significantly improved local control in those patients with metastatic disease who underwent surgery with or without adjuvant radiotherapy.25 In their series, patients with better ECOG performance status, HER2+ disease, and response to chemotherapy more often underwent surgery. Our data suggest those with lower-grade disease or bone-only metastases on presentation were more likely to undergo non-palliative local therapy. Not surprisingly, in both retrospective, non-randomized series, factors that portended a better prognosis made providers more likely to recommend local therapy despite metastatic IBC. The finding in our study that metastatic disease in non-locoregional lymph nodes was the only significant predictor of LRPR is thought provoking; it is unclear whether this finding is truly explained by underlying pathophysiology or due to chance in the setting of small numbers of patients. It is worth noting in our series that those patients with metastatic disease who received local therapy had a median survival of 2 years after the receipt of local therapy. This suggests that with careful patient selection, the benefits of local therapy could impact quality of life for a significant period of time, even in the setting of metastatic disease.
In addition to improved local control, several retrospective studies have demonstrated that among women with metastatic IBC, primary tumor resection or surgery plus radiotherapy significantly improved OS.25,39 However, as receipt of local therapy was non-randomized in these studies, these data need to be interpreted cautiously, given the likelihood of selection bias.
The limitations of this study are as with any retrospective study. In particular, receipt of non-palliative local therapy in patients with IBC presenting with metastatic disease was entirely dependent on provider preference as there is no institutional standard regarding local therapy in this cohort. Therefore, any comparison between those who did and did not receive non-palliative local therapy is subject to selection bias. Additionally, although our series represents one of the largest single institutional series, our results are limited by small numbers and events, decreasing the statistical power. However, due to the low incidence of IBC, prospective randomized trials addressing local therapy in this patient population are unlikely to be completed, and retrospective series are essential to informing management and guiding future prospective trials.
Conclusions
For patients with stage III and IV IBC, local disease progression or recurrence can result in significant morbidity. LRR remains high despite trimodality therapy in those patients without metastatic disease, and further study should examine opportunities for improving locoregional outcomes in this cohort. For select patients with metastatic disease, it may be reasonable to offer aggressive locoregional therapy, including mastectomy and/or radiotherapy. Further study is warranted to determine which patients derive a benefit with limited treatment-associated morbidity.
References
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. American Joint Committee on Cancer staging manual. 7th ed. Chicago (IL): Springer; 2011.
Dawood S, Merajver SD, Viens P, et al. International expert panel on inflammatory breast cancer: consensus statement for standardized diagnosis and treatment. Ann Oncol. 2011;22(3):515–23.
Cristofanilli M, Valero V, Buzdar AU, et al. Inflammatory breast cancer (IBC) and patterns of recurrence: understanding the biology of a unique disease. Cancer. 2007;110(7):1436–44.
Anderson BWF, Chu KC, Chang S. Inflammatory breast carcinoma and noninflammatory locally advanced breast carcinoma: distinct clinicopathologic entities? J Clin Oncol. 2003;21(12):2254–9.
Chang S, Parker SL, Pham T, Buzdar AU, Hursting SD. Inflammatory breast carcinoma incidence and survival. The Surveillance, Epidemiology, and End Results Program of the National Cancer. Cancer. 1998;82(12):2366–72.
Cabioglu N, Gong Y, Islam R, et al. Expression of growth factor and chemokine receptors: new insights in the biology of inflammatory breast cancer. Ann Oncol. 2007;18(6):1021–9.
Kleer CG, Zhang Y, Pan Q, et al. WISP3 and RhoC guanosine triphosphatase cooperate in the development of inflammatory breast cancer. Breast Cancer Res. 2004;6(2):R110–5.
Shirakawa K, Kobayashi H, Heike Y, et al. Hemodynamics in vasculogenic mimicry and angiogenesis of inflammatory breast cancer xenograft. Cancer Res. 2002;62(2):560–6.
Tomlinson JS, Alpaugh ML, Barsky SH. An intact overexpressed E-cadherin/alpha,beta-catenin axis characterizes the lymphovascular emboli of inflammatory breast carcinoma. Cancer Res. 2001;61(13):5231–41.
Ellis GK, Livingston RB, Gralow JR, Green SJ, Thompson T. Dose-dense anthracycline-based chemotherapy for node-positive breast cancer. J Clin Oncol. 2002;20(17):3637–43.
Huang EH, Tucker SL, Strom EA, et al. Predictors of locoregional recurrence in patients with locally advanced breast cancer treated with neoadjuvant chemotherapy, mastectomy, and radiotherapy. Int J Radiat Oncol Biol Phys. 2005;62(2):351–7.
Liao Z, Strom EA, Buzdar AU, et al. Locoregional irradiation for inflammatory breast cancer: effectiveness of dose escalation in decreasing recurrence. Int J Radiat Oncol. 2000;47(5):1191–200.
Damast S, Ho AY, Montgomery L, et al. Locoregional outcomes of inflammatory breast cancer patients treated with standard fractionation radiation and daily skin bolus in the taxane era. Int J Radiat Oncol Biol Phys. 2010;77(4):1105–12.
Rehman S, Reddy CA, Tendulkar RD. Modern outcomes of inflammatory breast cancer. Int J Radiat Oncol Biol Phys. 2012;84(3):619–24.
Ellis GK, Barlow WE, Gralow JR, et al. Phase III comparison of standard doxorubicin and cyclophosphamide versus weekly doxorubicin and daily oral cyclophosphamide plus granulocyte colony-stimulating factor as neoadjuvant therapy for inflammatory and locally advanced breast cancer: SWOG 0012. J Clin Oncol. 2014;29(8):1014–21.
Brito RA, Valero V, Buzdar AU, et al. Long-term results of combined-modality therapy for locally advanced breast cancer with ipsilateral supraclavicular metastases: The University of Texas M.D. Anderson Cancer Center experience. J Clin Oncol. 2001;19(3):628–33.
Harris EER, Schultz D, Bertsch H, Fox K, Glick J, Solin LJ. Ten-year outcome after combined modality therapy for inflammatory breast cancer. Int J Radiat Oncol Biol Phys. 2003;55(5):1200–8.
Bristol IJ, Woodward WA, Strom EA, Cristofanilli M. Locoregional treatment outcomes after multimodality management of inflammatory breast cancer. Int J Radiat Oncol. 2008;72(2):474–84.
Liauw SL, Benda RK, Morris CG, Mendenhall NP. Inflammatory breast carcinoma: outcomes with trimodality therapy for nonmetastatic disease. Cancer. 2004;100(5):920–8.
Palangie T, Mosseri V, Mihura J, et al. Prognostic factors in inflammatory breast cancer and therapeutic implications. Eur J Cancer. 1994;30A(7):921–7.
Ueno NT, Buzdar AU, Singletary SE, et al. Combined-modality treatment of inflammatory breast carcinoma: twenty years of experience at M.D. Anderson Cancer Center. Cancer Chemother Pharmacol. 1997;40:321–9.
Panades M, Olivotto IA, Speers CH, et al. Evolving treatment strategies for inflammatory breast cancer: a population-based survival analysis. J Clin Oncol. 2005;23(9):1941–50.
Bauer RL, Busch E, Levine E, Edge SB. Therapy for inflammatory breast cancer: impact of doxorubicin-based therapy. Ann Surg Oncol. 1995;2(4):288–94.
Takiar V, Akay CL, Stauder MC, et al. Predictors of durable no evidence of disease status in de novo metastatic inflammatory breast cancer patients treated with neoadjuvant chemotherapy and post-mastectomy radiation. Springerplus. 2014;3:166.
Akay CL, Ueno NT, Chisholm GB, et al. Primary tumor resection as a component of multimodality treatment may improve local control and survival in patients with stage IV inflammatory breast cancer. Cancer. 2014;120(9):1319–28.
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer. 2014. http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Accessed 15 Dec 2014.
Hazard HW, Gorla SR, Scholtens D, Kiel K, Gradishar WJ, Khan SA. Surgical resection of the primary tumor, chest wall control, and survival in women with metastatic breast cancer. Cancer. 2008;113(8):2011–9.
Rapiti E, Verkooijen HM, Vlastos G, et al. Complete excision of primary breast tumor improves survival of patients with metastatic breast cancer at diagnosis. J Clin Oncol. 2006;24(18):2743–9.
Fields RC, Jeffe DB, Trinkaus K, et al. Surgical resection of the primary tumor is associated with increased long-term survival in patients with stage IV breast cancer after controlling for site of metastasis. Ann Surg Oncol. 2007;14(12):3345–51.
Henderson MA, McBride CM. Secondary inflammatory breast cancer: treatment options. South Med J. 1988;81(12):1512–7.
McBride CM, Hortobagyi GN. Primary inflammatory carcinoma of the female breast: staging and treatment possibilities. Surgery. 1985;98(4):792–8.
Piera JM, Alonso MC, Ojeda MB, Biete A. Locally advanced breast cancer with inflammatory component: a clinical entity with a poor prognosis. Radiother Oncol. 1986;7(3):199–204.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53(282):457–81.
Greenwood M. The errors of sampling of the survivorship tables. Reports Public Heal Stat Subj. 1926;33(1):26.
Gray R. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat. 1988;16:1141–54.
Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94(446):496–509.
Kuk D, Varadhan R. Model selection in competing risks regression. Stat Med. 2013;32(18):3077–88.
Rueth NM, Lin HY, Bedrosian I, et al. Underuse of trimodality treatment affects survival for patients with inflammatory breast cancer: an analysis of treatment and survival trends from the National Cancer Database. J Clin Oncol. 2014;32(19):2018–24.
Dawood S, Ueno NT, Valero V, et al. Identifying factors that impact survival among women with inflammatory breast cancer. Ann Oncol. 2012;23(4):870–5.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Warren, L.E.G., Guo, H., Regan, M.M. et al. Inflammatory Breast Cancer: Patterns of Failure and the Case for Aggressive Locoregional Management. Ann Surg Oncol 22, 2483–2491 (2015). https://doi.org/10.1245/s10434-015-4469-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4469-4