
Abstract
The multi-stage inertial cascade impactor is used to determine the mass-weighted aerodynamic particle size distribution (APSD) as a critical quality attribute for orally inhaled products (OIPs). These apparatuses progressively size-fractionate the aerosol passing through a series of stages containing one or more nozzles, by increasing particle velocity. Nozzle sizes for a given multi-nozzle stage can be described collectively by effective diameter (\( \overset{\sim }{W_0} \)), related to the cut-point size, providing the link to aerodynamic diameter. Users undertake stage mensuration periodically to assure that each stage \( \overset{\sim }{W_0} \) remains within the manufacturer’s tolerance, but there is no guidance on how frequently such checks should be made. We examine the philosophy that particle size-related specifications of the OIP should determine when an impactor is mensurated. Taking an example of a dry powder inhaler-generated aerosol sampled via a Next Generation Impactor with pre-separator, we find that there are only three critical stages that could have a material effect on the measured APSD specified as four groupings of stages following current regulatory practice. Furthermore, \( \overset{\sim }{W_0} \) for the most critical stage having the smallest nozzle sizes could be relaxed by a factor of four or more before risking an inability to measure the mass fraction of API in the group containing the finest particles to a specification within ± 10% of nominal. We therefore conclude that users should consider letting the specification for APSD performance of an OIP in terms of accepted stage groupings drive the impactor quality requirements and frequency that stage mensuration is undertaken.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
The inertial multi-stage cascade impactor is the most widely used apparatus for the determination of aerosol aerodynamic particle size distribution (APSD) from orally inhaled products (OIPs). Despite their labor-intensive operation, these apparatuses have not been replaced by alternative, more automated, aerosol particle sizing instrumentation, primarily because they uniquely are able to quantify the mass of active pharmaceutical ingredient(s) (API(s)) present in the emitted aerosol as a function of particle aerodynamic diameter [1]. Aerodynamic size is more directly related than physical size to the likely location and efficiency of deposition of such particles in the respiratory tract where either topical or systemic therapy can be delivered [2]. The multi-stage impactor operates as a sequential particle size-fractionating apparatus. Each component stage makes use of differences in particle inertia in a laminar flow field passing through one or multiple cylindrical nozzles of the same controlled diameter as the flow diverges in response to the approach to a solid surface located closely beneath the nozzle exit plane [3]. Larger particles will leave the air stream and be collected on this surface, which may be coated with a thin layer of energy-absorbent substrate, such as a surfactant, to mitigate bias from particle bounce and re-entrainment in the flow. Cascade impactors achieve size-fractionation of the incoming particles at progressively finer sizes by increasing the linear air velocity through the nozzles of each successive stage [4].
The maintenance of performance of the cascade impactor in terms of its size-fractionating capability is an important aspect to consider in the context of using these apparatuses as the means of ascertaining emitted aerosol APSD as a drug product critical quality attribute (CQA) contributing to the quality target product profile (QTPP) of an OIP, as described in a recent FDA draft guidance for industry in connection with the evaluation of pressurized metered dose inhalers (pMDIs) and dry powder inhalers (DPIs) [5]. In this context, we start by asking the following question: For a registered drug product, what constitutes sufficient and necessary criteria for the quality of the cascade impactor with which the inhaler manufacturer performs batch release testing? In response, we pose a further question: Should not the batch release requirements of the product itself dictate the accuracy and precision needed from the cascade impactor? Taking an analogous situation from everyday life, we do not need an atomic clock to enable us to catch public transit to and from work. The purpose of this article is therefore to start the process moving towards the goal of achieving a clearer understanding of what is necessary for the cascade impactor apparatus to be effective as an apparatus in the assessment of OIP quality for meeting the product specification in batch release testing.
THE ROLE OF STAGE NOZZLE DIMENSIONS AS CRITICAL COMPONENTS IN ESTABLISHING THE SIZE-FRACTIONATING CAPABILITY OF THE CASCADE IMPACTOR
Currently, the most widely used impactors, and the apparatuses on which we focus the present article, are the eight-stage Andersen non-viable cascade impactor (ACI) and the seven-stage Next Generation Pharmaceutical Impactor (NGI) [6]. Both impactors size-fractionate aerosols in the overall range from 0.1 to 12 μm aerodynamic diameter, the precise limits depending upon the operating flow rate, typically in the range from 30 (28.3) to 100 L/min [7]. The United States Food and Drug Administration (FDA) has in the past indicated a preference for a size-resolution of at least five data points between the clinically important range from 0.5 to 5.0 μm aerodynamic diameter so as to define adequately the aerosol APSD. This informal recommendation partly drove the design of the NGI [8] and has eliminated other apparatuses, such as the Multi-Stage Liquid Impinger and the Marple-Miller series of impactors, from use in product registrations for the US marketplace. The design of the NGI is unique in its adherence to the known principles of aerodynamic particle size fractionation [9,10,11], and for this reason the following discussion will tend to emphasize this impactor.
Currently, users include particle sizing data in their new drug applications to the FDA, and the cascade impactors that generate these data are by default assumed to perform aerodynamically in the same range as that allowed for newly manufactured impactors. Then, for used impactors, Good Cascade Impactor Practices (GCIP) require that the critical size-fractionating parts of the measurement apparatus are periodically measured [12]. These components are the diameters of the nozzles through which the incoming aerosol particles pass before being subjected to inertial size separation. This “stage mensuration” procedure is practiced to assure that significant changes have not occurred in use as a result of corrosion or plugging by debris. The effective diameter (\( \overset{\sim }{W_0} \)) calculated from the stage mensuration data [13] is a measure of the “average” nozzle diameter of a multi-nozzle stage [12]. \( \overset{\sim }{W_0} \) has been shown to be directly related to the cut-point size of the stage (D50), enabling traceability of the size-fractionating performance of the stage to the international length standard [13]. Therefore, impactors exhibiting \( \overset{\sim }{W_0} \) values in the same range as those of newly manufactured impactors are considered qualified for continued use.
The current logic underlying the setting of quality specifications for used cascade impactors is as follows:
- a)
Impactors supplying the data for new drug applications are assumed to meet manufacturer specifications.
- b)
The FDA issues batch release specifications for manufactured inhalers based partially on the mass captured in each stage or group of stages of the same model of cascade impactor.
- c)
As long as no values of \( \overset{\sim }{W_0} \) for used impactors are found to be outside of that allowed for newly manufactured impactors, the used impactors are considered to be of sufficient quality and therefore all mass-related impactor data taken for the batch release of the inhalable drug product are considered valid.
Given the foregoing, the inhaler testing community today does its best to ensure, at least at the time of periodic optical inspection of the impactor nozzles, that impactors used regularly for batch release testing of registered drug products are sufficiently accurate to ensure the validity of the batch release test data.
However, we question here whether the constraints on \( \overset{\sim }{W_0} \) are too strict. More specifically, we ask if it is unnecessary that the values of \( \overset{\sim }{W_0} \) measured for used impactors be in exactly the same range as those allowed by the manufacturer for new impactors? As difficult as this question may be to answer, it is also important to ask the opposite question whether both new impactors, made to manufacturer’s specifications, and used impactors meeting these same specifications, are unable to distinguish clinically important differences in the particle sizes delivered by a given inhalable drug product. Put another way, are either the new or used impactor quality specifications insufficient for ensuring a safe and efficacious drug product? Given that cascade impactor-based methodologies have been in place for more than 30 years without published evidence that OIPs have not met safety and efficacy criteria as a direct result of failure of the impactor as a result of changes in \( \overset{\sim }{W_0} \) to define the underlying aerosol APSD accurately, we will assume the answer to this second question regarding sufficiency, is no. We will further assume that the specifications for the drug product itself, as issued by FDA when it approves an inhalable drug product for sale, are sufficient for safety and efficacy. It therefore follows, as a baseline condition, that the quality of used impactors is sufficient if the values of \( \overset{\sim }{W_0} \) measured are within the same range as those allowed by the manufacturer for new impactors. We can then move forward and deal only with the question of “necessity” of the current method of setting pass/fail criteria on used impactors.
We show in the following sections, then, how an approach based on current FDA batch release criteria for a registered drug product might work to set these necessary quantitative limits on the quality of the cascade impactors used for batch release testing. The result will be necessary and sufficient impactor quality requirements that depend directly on the product quality specifications and are independent of the impactor quality specifications for new impactors. However, beforehand, a review of the measurement process is necessary to understand the origins of the sized and non-sized portions of the emitted OIP aerosol and exactly what can be measured in the context of defining the sized mass fraction.
FUNCTION OF THE APSD MEASUREMENT EQUIPMENT IN GENERATING THE NON-SIZED AND SIZED MASS FRACTIONS OF THE INCOMING AEROSOL
The complete APSD of the aerosol emitted from an OIP is never reported as a measure of product quality because the cascade impactor is preceded by components that do not have defined upper and lower limits on the captured particle size. This feature of OIP testing equipment is in contrast with applications of impactors in other applications, such as environmental aerosol measurement [14], where the sampled aerosol directly enters the impactor. This limitation is not regarded as being important when determining inhaler performance, because the so-called “non-sized” component comprises particles having sufficient inertia that they deposit in the oropharynx, and are therefore uninvolved in medication delivery to receptors in the airways of the lungs. In consequence, the non-sized mass in aggregate is regarded as a single component in the data grouping process [5].
In more detail, the incoming aerosol first passes through an inlet (induction port) whose purpose nominally is to represent passage of the aerosol through the oropharyngeal region of a patient using the inhaler. The internal passageway of the induction port may be made to be accurately representative of human oropharyngeal anatomy [15], or it can be of simplified internal construction (“idealized” inlet), but with sufficient detail to behave in a similar manner [16]. However, for APSD measurements in the context of product quality control, the United States Pharmacopeia/European Pharmacopoeia (USP/PhEur) induction port is the standard inlet [7]. This entry to the size-fractionating equipment consists of a pipe having a simple smooth internal finished right-angle bend; the inhaler is operated with its mouthpiece in the horizontal orientation and the aerosol exits vertically downwards. The portion that penetrates the induction port is sampled directly by the cascade impactor when testing soft mist inhalers (SMIs), products for nebulization, almost all pMDIs and those DPIs in which large carrier particles are not present in the formulation [7]. However, many formulations dispersed by currently marketed DPIs are formulated with relatively large carrier particles (typically lactose) upon which the API(s) are attached to the surface [17]. When inhaled, these carrier particles deposit in the oropharynx, so a pre-separator is needed to mimic this process when such DPIs are evaluated in the laboratory [7]. The pre-separator is located between the distal exit of the induction port and the entry to the impactor. Once subjected to a significant flow, the finer API-containing particles detach from the carrier, as the aerosol passes through the pre-separator where the carrier particles are removed by inertial separation. The remaining fine particle stream then passes to the cascade impactor for subsequent size fractionation therein [18]. The pre-separator also avoids potential bias that would occur if high inertia carrier-drug particles were to enter the impactor and therefore be prone to bounce and re-entrainment rather than impacting on the collection surface of the first size-fractionating stage.
When considering the way in which the aerosol from the OIP is processed by a particular apparatus for APSD measurement, it is important to appreciate that the sized and non-sized mass fractions represent the most fundamental division of the emitted particles (Fig. 1). The non-sized fraction comprises everything recovered from the induction port and pre-separator. In the case of the NGI including its pre-separator, the cut-point size at which 50% of the incoming particles penetrate the pre-separator (D50-presep) is known for operation between 30 and 100 L/min, because the stage collection efficiency-aerodynamic diameter profiles were established by calibration of an archival instrument using particles of known aerodynamic diameter [19]. It follows that the mass that subsequently enters the first impaction stage (stage 1) becomes part of the sized fraction because the upper bound size of particles entering that stage is known [20]. However, if the NGI pre-separator is not present, the API mass on stage one is assigned to the non-sized mass fraction and that recovered from the following stage (stage 2) becomes the largest sized component of the collected API mass [20]. For the ACI, none of its pre-separators that are available for use at different flow rates have defined values of D50 from archival calibration, so that the mass of API recovered from the uppermost stage of this impactor is always assigned to the non-sized mass fraction.

Fractionation of emitted aerosol from an OIP by pharmacopeial compendial methods: the apparatus is operated at a constant flow rate throughout the measurement for pMDIs, SMIs, and nebulizing systems; for DPI testing, the application of the vacuum at the exit of the apparatus initiates aerosol transfer from the exit of the inhaler through the USP/PhEur induction port via a pre-separator (if used) to the multi-stage cascade impactor. The collection efficiency curve for the pre-separator (where known) and for each impactor stage determines the size ranges into which the aerosol is ultimately grouped in order to compare against the product specification
The impactor-sized mass (ISM) is the sum of the mass of API recovered from the micro-orifice collector (NGI) or back-up filter together (NGI or ACI), and the corresponding mass recovered from each of the stages whose upper-bound size of entering particles is known. The APSD that is used as an indication of OIP quality is therefore based only on that portion of the total emitted mass that is contained in sizes within the limit used to define the ISM.
PRODUCT SPECIFICATION SETTING DEFINES THE CRITICAL STAGES OF THE MEASUREMENT APPARATUS FOR OIP APSD DETERMINATION
The QTPP is a prospective summary of the quality characteristics of a drug product that ideally will be achieved to ensure the desired quality, considering both product safety and efficacy [21]. The FDA recommends that the complete APSD of the inhaler product be always determined during product development for a variety of purposes, in particular support to the clinical program and establishing product stability in development, as well as suitability for batch release in production [5]. Statistical measures such as mass median aerodynamic diameter (MMAD) and geometric standard deviation (GSD), indicating central tendency and spread of the underlying APSD, respectively, are by themselves therefore deemed insufficient descriptors of product aerodynamic performance [5]. Implementation of this part of the guidance therefore necessitates recovering API from every size-fractionating stage of the cascade impactor, as well as the pre-separator when used. In addition, when setting product release specifications, applicants for product registration are also advised to propose acceptance criteria for groupings of consecutive stages rather than proposing an acceptance criterion for each individual stage of the impactor [18]. The exact number of groupings is not specified, as the applicant is expected to provide a rationale for the number of groupings and the associated particle size ranges, based on the specific physicochemical properties and clinical indication of the product being registered. In this context, the non-sized portion of the emitted mass of aerosol from the inhaler is generally treated in aggregate as a separate single grouping when setting specifications for product quality [22,23,24].
For the purpose of illustration, it is assumed that the following four groupings are the norm, based on information from APSD specifications given in OIP monographs published in the pharmacopeial compendia [19,20,21, 25]:
Group 1 comprises the non-sized mass fraction.
Group 2 contains the commonly termed “coarse” component of the sized fraction containing particles between about 5 μm aerodynamic diameter and the upper size limit of the impactor-sized mass.
Group 3 contains particles between about 5 μm and approximately 1 μm aerodynamic diameter, commonly referred to as the fine particle mass.
Group 4 contains the rest of the particles, typically sub-micron in size, and is often termed the extra-fine particle mass.
From the foregoing, it is self-evident that the stage whose cut-point size is closest to the lower bound size for a given group is identical with the stage defining the upper-bound size of the adjacent group containing finer particles, so that in effect only three components have collection efficiency-aerodynamic diameter profiles that are critical. Their collection efficiency-aerodynamic diameter profiles are identified in Fig. 1 by red curves. The only requirements for the non-critical stages, whose collection efficiency-size profiles are identified in black, is that they function as inertial impactors, for instance, meeting the design criteria for nozzle exit to collection surface distance identified by Marple and Liu [3]. In practice, these criteria are easily met by modern impactor designs. The only other condition, applicable to both critical and non-critical stages, is that that non-ideal influences, in particular particle bounce and re-entrainment, are eliminated [26, 27].
RELATIONSHIP OF THE MASS-PER-STAGE MEASUREMENT CAPABILITY OF A CASCADE IMPACTOR TO CRITICAL IMPACTOR NOZZLE DIMENSIONS: THEORETICAL CONSIDERATIONS
We first derive a quantitative relationship between the particle size-related critical quality attribute (psr-CQA) of the OIP and the (often presumed to be known) impactor nozzle diameters and the measured mass of drug product on each stage. We thereby show that the requirements for the quality of the impactor nozzles can be directly related to the batch release criteria for an OIP.
Suppose the aerosol entering the impactor has a particle size distribution with any shape whatsoever and denoted by R*(dp). Then, the fraction collected on the “nth” component of the impactor, denoted by fn, can be written:
Here, R(x) is the fractional particle size distribution:
The denominator of Eq. (2) is the total mass captured in all the components of the impactor.
For the special case wherein all of the particle collection efficiency curves of the impactor components are perfectly ideal and therefore described by the Heaviside step function, as in Eqs. (7) and (8) of Roberts [28], Eq. 1 becomes simply:
Here, the quantity D50,n represents the aerodynamic diameter for each stage at which the collection efficiency is 50%. For n = 1, we use D50,n-1 as the 50% efficiency diameter of the first size-fractionating component of the cascade impactor, and we give it the symbol D50,0.
It is well known that the D50 values are in turn directly related to the effective diameter of the N nozzles associated with each stage (\( \overset{\sim }{W_0} \)), through the relationship [28]:
in which St50 is the Stokes’s number corresponding to the size, D50, (St1/2 = 0.49 for round nozzles [3]), μ is the air viscosity, C is the Cunningham slip correction factor that is close to unity for particles in the size range produced by OIPs, ρp is the particle density, and QT is the volumetric flow rate entering a given impactor stage. \( \overset{\sim }{W_0} \) is therefore a quantity that depends on the measured diameter of each nozzle on each stage, a process that has been outlined in more detail in the section developing the understanding between the role of critical impactor components in establishing the size-fractionating capability of the impactor.
Therefore, when the psr-CQAs depend exclusively on the values of fn, it follows that the impactor nozzle diameters described by \( \overset{\sim }{W_0} \) for each stage, and the shape of the APSD, are related quantitatively. Equation (3), then, represents the intertwining of the batch release psr-CQAs and the impactor quality. Indeed, a simple application of error analysis principles [29] to Eq. (3) yields an expression for the sensitivity of the psr-CQA to the uncertainty in the D50 value of the two stages that together determine the magnitude of the API mass in the appropriate size range that is captured on a given stage:
Here, R(D50,n-1) and R(D50,n) are the values of the size distribution at the D50 value of stage n-1 and n, respectively. We have made use of the fact that the derivative of an integral is the integrand evaluated at the limits of the integral in order to derive Eq. (5). Because the particle size distribution R(dp) is the slope of the cumulative particle size distribution, this equation states that the accuracy of the D50 values required to meet a given range for fn depends on the slope of the cumulative size distribution at the end points of any given stage’s particle size range. Equation (5) then holds the key to understanding what constitutes necessary impactor specifications. In particular, we note that there is no reference in this equation to the new impactor stage nozzle diameter specifications offered by the manufacturer, and further that this equation assumes nothing about the shape of the APSD. It is therefore generally applicable.
APPLYING THE CONCEPT OF CRITICAL IMPACTOR STAGE NOZZLE DIMENSIONS IN PRACTICE: A DPI TESTED WITH THE NGI AT 60 L/MIN
We acknowledge that the concepts introduced herein are complex to assimilate, and therefore provide the following example as an illustration. It should be noted at the outset that similar considerations would apply to the aerodynamic particle size analysis of an aerosol from any of the other OIP classes and with any multi-stage cascade impactor.
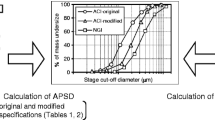
Consider a DPI discharged into an NGI apparatus, in accordance with pharmacopeial methodology [7]. The components of this apparatus from which API will likely be recovered include the induction port, the pre-separator, and all eight cups (Fig. 2). An archival NGI and its pre-separator manufactured with nozzle diameters close to nominal values have been calibrated with standard monodisperse particles, as previously mentioned. This process thereby provided reference D50 values for all apparatuses whose nozzle sizes remain within the manufacturer’s specification [19]. The pre-separator has its own aerodynamic size-fractionating stage consisting of a plate with six nozzles, and therefore the pre-separator is the first size-fractionating component (Fig. 3). For the purposes of this example, we have chosen a hypothetical API deposition profile of the mass of drug product recovered from the components of the impactor that we believe from experience to be representative of aerosols from this class of OIP (Table I). The precise flow rate at which the NGI is operated is unimportant for the purpose of this example, although this variable would in practice be tightly controlled [30].

NGI assembled with pre-separator for the APSD determination of a DPI-generated aerosol in accordance with the pharmacopeial methodology [7]

NGI pre-separator; its single size-fractionating stage comprises six nozzles, each 12.80 ± 0.05 mm in diameter [8]
We assume that if this hypothetical product is in late-stage clinical trials or early in the manufacturing of a commercial batch, the clinical outcomes and therefore the therapeutic safety and efficacy would be based on inhalers that have displayed a deposition profile very similar to that given here. With these representative data, we consider it likely that the drug manufacturer would propose, or the FDA would have already approved, psr-CQAs in accord with “stage groupings” such as given in Table I, in accord with the pertinent FDA draft guidance [5]. Manufacturers with an existing and approved drug product will have the CQAs and their acceptable range already established as a result of FDA approval. Based on our experience of the variability of replicate OIP APSD determinations, we also propose that a reasonable quality control tolerance for the mass in each grouping be ± 10% of the expected value. This degree of control is somewhat tighter than seen in the published monograph specifications [22,23,24,25], discussed by Byron et al. [29]. However, we assume that a safety margin for variability would be applied in practice for batch release testing. We note that the magnitude of this range strongly influences the necessary and sufficient quality attributes of the nozzles of the cascade impactor.
At this stage of the example, we observe that stakeholders may be tempted to assign size-related descriptive names, such as “coarse,” “fine,” and “extra-fine” to these stage groups. However, we counsel against this practice, given the guidance from the FDA that the number of such groupings, including the non-sized mass fraction may be either 3 or 4, advising that sponsors should effectively propose the acceptance criteria on a product-by-product basis, presumably including the size ranges applicable to the groupings [5]. It therefore follows that the particle size ranges associated with each grouping must be regarded as approximate; the values given in Table I are therefore simply the appropriate stage D50 values at the upper and lower end of each chosen grouping for this particular example (see red collection efficiency curves in Fig. 1 for the critical stages). Note that if the stage efficiency curves were actually abrupt step-functions (Eq. (3)), then these ranges are the particle sizes that would actually be found in these groupings. In this context, Roberts and Mitchell [31] have shown theoretically that for log-normally distributed model aerosols sized by either the ACI or NGI and having APSDs in the size range of typical aerosols from commercially available OIPs, the mass on each stage, when considering the full stage efficiency curve, deviates only by a few percent from that predicted by a step-function. Particles captured in the induction port can in principle be any size, but there appears to be no interference with the pre-separator [32].
Returning to the considerations outlined in the previous section in which the concept of critical and non-critical impactor stages was introduced, we remind the reader that arranging the mass of API recovered from components into four groups places quality constraints on only three sets of nozzles in the impactor (Fig. 1). Stated another way, a typical stage grouping suggested by the pertinent FDA draft guidance related to OIP product quality [5] places constraints on only some of the stage nozzles of the cascade impactor. In our example, it follows that the quality constraints on the magnitude of ISM determined by the NGI are limited to the following critical attributes of the impactor apparatus:
- a)
The pre-separator D50 value—which is the upper bound of group 2
- b)
The stage 2 D50 value—which is the lower bound of group 2 and also the upper bound of group 3
- c)
The stage 5 D50 value—which is the lower bound of group 3 and also the upper bound of group 4
Figure 4 displays the stage groupings and the D50 values of each stage of the NGI for the example case, highlighting in bold and enlarged font these three values that control all four stage groupings. It should be noted that, as well as determining the amounts of API mass contained in the three groupings that contribute to the ISM, the magnitude of the non-sized mass fraction, comprising group 1, is controlled in part by the location of the D50 value for the pre-separator.

Identification of key nozzle pieces for meeting OIP APSD CQAs based on combining API mass contributing to ISM recovered from components of NGI with pre-separator into four stage groupings: critical stage D50 values are highlighted by larger font size, and the half-ring elements in the table below represent upper and lower bound sizes associated with each impactor stage
Although we have focused this far on the critical stages that control the mass of API assigned to each grouping of the sized mass fraction, there is a tacit understanding previously mentioned that the intermediate “non-critical” stages should at least function as viable size fractionators. We therefore propose, as a sufficient and measurable criterion, that the jet-to-plate distance for these stages be within manufacturer specifications [28]. This criterion gives users a wide latitude, and one that is unlikely to be violated when these non-key impactor nozzle pieces are maintained in a manner similar to those whose D50 values are critical to defining the API mass assigned to the stage groupings that form the psr-CQA for the OIP.
Expressing these stage groupings in accord with Eq. 3, we have the following descriptions for the groups in the example contributing to ISM:
The important quantities here, related to impactor quality, are D50,0, D50,2, and D50,5. The simple relationship of these three quantities to the fractional collections in each size grouping can be best seen by rearranging these equations as follows:
Equation (9) indicates that all of the API recovered from the eight cups of the NGI consists of all particles smaller than the D50 value for the pre-separator. Equation (10) shows that all of the API in cup numbers 3 through 8 consists of particles smaller than the D50 size of stage 2. Finally, Eq. (11) signifies that all of the API in cup numbers 6, 7, and 8 consists of particles smaller than the D50 value for stage 5.
There are several consequences as the result of this analysis:
- 1.
The nozzles of stage 5 are the only ones deserving attention to verify they have remained within specification.
The question may be asked why this outcome is the case. In response, the six nozzles on the pre-separator are so large (each having a nominal diameter of 12.8 mm (8)), that they are never likely to become occluded with unwanted micrometer-sized particulate matter, even with simply the absolute minimum of care. The same is true of the six nozzles of stage 2 that are each 4.88 mm nominal diameter (8). No used pre-separator nozzles nor used stage-two nozzles failed to pass the quality expectations of a new pre-separator or new stage 2 during the many years one of us (DLR) was in the business of making new NGIs and inspecting new and used impactor nozzles. However, there are 152 nozzles, each nominally much smaller at 0.608 mm in diameter for stage 5 (8). Anecdotally, this nozzle piece can become occluded, and certainly needs careful attention in routine use. Even regularly cleaned, in-use stage 5 nozzle pieces have been known to fail optical inspection in a (typically) annual stage mensuration. Importantly, note also that this result holds regardless of the size distribution of the therapeutic drug particles because its validity is an outcome of the impactor hardware performance.
- 2.
The quality requirements for the stage 5 nozzles depend on the SLOPE of the cumulative APSD at the D50 value of stage 5.
This outcome is obtained by applying the general result (Eq. (5)) to Eq. 11 to find:
The intuitive meaning of Eq. (12) is quite satisfying; namely, if the drug product quality needs to be in a given range (denoted by the allowable uncertainty in f4), then the required quality of stage 5 (denoted by the allowable uncertainty in D50,5) depends on whether there is much API mass in particles of a size close to the dividing line between capture by stage 5 or by stage 6. The value R(D50,5) is simply the slope of the cumulative size distribution at D50,5, and D50,5 is the dividing size between assignment of API mass to group 3 or group 4. So, another way to view Eq. (12) is the following interpretation: “if there is not much movement of the size distribution exactly at the particle size D50,5, then the ability of the impactor as a size-fractionator to maintain a constant particle size division of material between groups 3 and 4 is non-critical.”
So now we ask “how does one calculate quantitatively the necessary range of D50,5 so as to satisfy the batch release criteria associated with f4 (Table I; 1.8 to 2.2%, \( {\sigma}_{f_4}^2 \) = 0.01). After all, the slope of the cumulative size distribution right at the D50 value of stage 5 is normally unknown. In response, we observe that any numerical curve fit to the mass-per-stage data [33, 34] can be used to make this calculation. We comment here only on the likely range of values, and leave it for future studies to elucidate all of the implications of Eq. (12). A linear estimate of the slope of the cumulative size distribution at D50,5—R(D50,5)—yields a value of 0.03 μm−1. And since D50,5 itself is approximately 1 micron, Eq. 12 reduces to:
Equation (13) indicates that the precision required for the D50 value for stage 5 is approximately the same as the precision required for f4. The precision of this D50 value, based on manufacturer’s nozzle diameter specifications published in the United States Pharmacopeia [7], is approximately 2.4% of its nominal value. So, as a first approximation, the nozzle diameter specifications could be relaxed by a factor of four or more before risking an inability to measure the group 4 mass fraction to within the previously chosen ± 10% tolerance specification. So, it follows that the stage group definitions associated with a typical approved OIP batch release, as currently practiced, place very easy-to-meet quality constraints on the cascade impactor. Equation 13 ignores the uncertainties introduced by the uncertainty in the D50 values of neighboring stages, uncertainties that assuredly affect the precision with which one can estimate the slope of the cumulative size distribution. These sorts of considerations will be necessary for tackling the entire impactor specification problem.
However, the approach posed here may well enable a simple application of pressure drop principles to the monitoring of impactor quality. With only a small adaptation to the lid of the NGI, one can provide pressure taps associated with each stage (Fig. 5), and it is then possible to monitor the pressure drop across the nozzle plate of each stage. This measurement is valuable because the pressure drop (ΔPstage x) across an impactor stage “x” at a fixed flow rate (Q) can be described well by a Bernoulli-style equation [35]:
where At is the total area of the nozzles for stage “x”, ρa is the air density, and K is the discharge coefficient (determined experimentally and being a fixed value for a given nozzle geometry). Multi-month monitoring of stage pressure drop of NGIs equipped with pressure taps has since shown that the analytical power of such monitoring is sufficient to detect the influence of debris accumulation in nozzles associated with routine use in-service, provided the pressure at the entry of the apparatus is maintained at a constant reference value while measurements of pressure drop are being made [36].

Next-generation impactor with lid modified to enable pressure drop across selected stage nozzle plates to be monitored before each measurement as a system suitability test
For the typical four groups of particles assigned by the FDA, we maintain that the user therefore would need to follow the pressure drop at only one stage (stage 5, taking our example). This stage has a pressure drop of approximately 500 Pa at a flow rate of 60 L/min, measured easily with common pressure transducers, especially to the precision implied by Eq. (13). The practice of following pressure drop in-use would thereby provide assurance of impactor aerodynamic performance each and every test, eliminating the possibility of discovering an analytical problem only at the time of an annual optical inspection, or, worse, not discovering a problem and inappropriately releasing drug product to the consumer.
We believe that the foregoing considerations would substantially simplify the means of ensuring impactor quality but would otherwise result in only minor changes to the procedures currently employed in the laboratory for inhaler APSD determination. There can be advantages to focusing a specific set of impactors to batch release testing of one and only one inhaler product, but that is not a requirement. Rather, the considerations described here relate to the physical properties of the impactor itself and not to the size-properties of the aerosol being sampled. Although not addressed in this article, similar considerations could apply to the use of an impactor in the testing of nasal products by cascade impactor. However, it should be noted that stage grouping into as many as three sized portions, the very small quantities of API that typically comprise the portion of the dose contained in particles small enough to be sized in this way (typically < 15 μm aerodynamic diameter) [37], is likely to be impractical, given the sensitivity of the analytical equipment used to quantify API mass.
We look forward to the day when impactor users are no longer satisfied with knowing only once per year that their impactors are within specifications. Given the implications arising from this analysis of the situation, the common practice of once-per-year optical inspection seems to be untenable for batch release testing of registered drug products, however appropriate it may be in a research and development environment.
CONCLUDING REMARKS
Periodic stage nozzle mensuration provides a valid check of the size-fractionating performance of these critical components of a cascade impactor, providing ultimately a link from the stage D50 size to the international length standard [12]. However, specific guidance is currently lacking on when and how frequently this check needs to be carried out. Users generally undertake the procedure at fixed time intervals, often annually without regard for the condition of the stage nozzles. The present assessment has shown that the aerodynamic size-fractionating performance of just three stages of the NGI (including its pre-separator when used), whose D50 values mark the boundaries of each of the API mass groupings, are important for a typical four-grouping specification associated with OIP quality assessment. Furthermore, the nozzle diameter specifications for the most critical stage having the smallest nozzle sizes could be relaxed by a factor of four or more before risking an inability to measure the mass fraction of API in the group containing the finest particles (group 4) to a specification within ± 10% of nominal. We therefore conclude that users should consider letting the specification for APSD performance of an OIP in terms of accepted stage groupings drive the frequency that stage mensuration is undertaken.
References
Mitchell J, Newman S, Chan H-K. In vitro and in vivo aspects of cascade impactor tests and inhaler performance: a review. AAPS PharmSciTech. 2007;8(4):110. https://doi.org/10.1208/pt0804110 Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2750696/ Accessed September 27th 2018.
Hinds WC. Aerosol technology properties, behavior, and measurement of airborne particles. 2nd ed. New York: Wiley; 1999. p. 134–8.
Marple VA, Liu BYH. Characteristics of laminar jet impactors. Environ Sci Technol. 1974;8(7):648–54.
Dechraksa J, Suwandecha T, Maliwan K, Srichana T. The comparison of fluid dynamics parameters in an Andersen cascade impactor equipped with and without a preseparator. AAPS PharmSciTech. 2014;15(3):792–801.
United States Food and Drug Administration. Draft guidance for industry: metered dose inhaler (MDI) and dry powder inhaler (DPI) products—quality considerations. Silver Spring, MD, USA. 2018. available at: https://www.fda.gov/downloads/drugs/guidances/ucm070573.pdf , visited September 28, 2018.
Nichols SC, Mitchell JP. An assessment of the comparative efficiency of abbreviated versus full resolution cascade impactor measurements: a survey of European Pharmaceutical Aerosol Group (EPAG) members. Drug delivery to the Lungs-24. Edinburgh: The Aerosol Society; 2013. p. 237–40.
US Pharmacopeial Convention. United States Pharmacopeia 41/National Formulary 36, Chapter <601> Aerosols, nasal sprays, metered-dose inhalers, and dry powder inhalers. Rockville. 2018.
Marple VA, Roberts DL, Romay FJ, Miller NC, Truman KG, Van Oort M, et al. Next generation pharmaceutical impactor. Part 1: design. J Aerosol Med. 2003;16(3):283–99.
Marple VA. A fundamental study of inertial impactors. PhD Dissertation, Minneapolis: University of Minnesota, 1970.
Rader DJ, Marple VA. Effect of ultra-Stokesian drag and particle interception on impactor characteristics. Aerosol Sci Technol. 1985;4(2):141–56.
Roberts DL, Mitchell JP. The Next Generation Impactor (NGI™)—manufacturing control: Part 1—nozzles. Inhalation. 2016;10(2):12–9.
Nichols SC, Mitchell JP. Stimulus to revision: a rational approach to cascade impactor mensuration in a good cascade impactor practice (GCIP) environment. Pharm Forum. 2014;40(1) on line at: https://www.uspnf.com/pharmacopeial-forum, visited September 28, 2018.
Roberts DL, Romay FJ. Relationship of stage mensuration data to the performance of new and used cascade impactors. J Aerosol Med. 2005;18(4):396–413.
Mitchell JP, Nagel MW. Cascade impactors for the size characterization of aerosols from medical inhalers: their uses and limitations. J Aerosol Med. 2003;16(4):341–77.
McRobbie DW, Pritchard S, Quest RA. Studies of the human oropharyngeal airspaces using magnetic resonance imaging. I. Validation of a three-dimensional MRI method for producing ex vivo virtual and physical casts of the oropharyngeal airways during inspiration. J Aerosol Med. 2003;16(4):401–15.
Zhang Y, Finlay WH, Matida EA. Particle deposition measurements and numerical simulation in a highly-idealized mouth-throat. J Aerosol Sci. 2004;35(7):789–803.
Dunbar CA, Hickey AJ, Holzner P. Dispersion and characterization of pharmaceutical dry powder aerosols. KONA Powder and Particle Journal. 1998;16:7–45.
Hickey AJ. Complexity in pharmaceutical powders for inhalation: a perspective. KONA-Powder and Particle. 2018;35:3–13.
Marple VA, Olson BA, Santhanakrishnan K, Mitchell JP, Murray SC, Hudson-Curtis BL. Next generation pharmaceutical impactor. Part II: archival calibration. J Aerosol Med. 2003;16(3):301–24.
Mitchell JP, Sandell D, Suggett J, Christopher JD, Leiner S, Walfish S, et al. Stimulus to revision: proposals for data interpretation in the context of determination of aerodynamic particle size distribution profile for orally inhaled products. Pharm Forum. 2017;43(3) on line at: https://www.uspnf.com/pharmacopeial-forum , visited September 28, 2018.
United States Food and Drug Administration. Guidance for industry: Q8(R2)—pharmaceutical development. 2009. available at: https://www.fda.gov/downloads/drugs/guidances/ucm073507.pdf , visited September 28, 2018.
United States Pharmacopeial Convention. Product monograph for fluticasone propionate and salmeterol inhalation powder. Rockville, USP41-NF36; 2018. Available at: https://online.uspnf.com/uspnf/document/GUID-A54661A3-DF23-400A-8763-0213D19A10C6_1_en-US, visited October 15, 2018
United States Pharmacopeial Convention. Product monograph for fluticasone propionate inhalation aerosol. Rockville: USP41-NF36; 2018. Available at: https://online.uspnf.com/uspnf/document/GUID-39375AC5-C31B-4C74-AB80-75FD5D95A6A0_1_en-US, visited October 15, 2018
United States Pharmacopeial Convention. Product monograph for fluticasone propionate and salmeterol inhalation aerosol. Rockville: USP41-NF36; 2018. Available at: https://online.uspnf.com/uspnf/document/GUID-5BD2B30C-5CC9-4003-8ED1-59E4FF6B0CAF_1_en-US, visited October 15, 2018
United States Pharmacopeial Convention. Product monograph for fluticasone propionate inhalation powder. Rockville: USP41-NF36; 2018. Available at: https://online.uspnf.com/uspnf/document/GUID-A54661A3-DF23-400A-8763-0213D19A10C6_1_en-US, visited October 15, 2018
Nasr MM, Ross DL, Miller NC. Effect of drug load and plate coating on the particle size distribution of a commercial albuterol metered dose inhaler (MDI) determined using the Andersen and Marple-Miller cascade impactors. Pharm Res. 1997;14:1437–43.
Dunbar C, Kataya A, Tiangbe T. Reducing bounce effects in the Andersen cascade impactor. Int J Pharm. 2005;301:25–32.
Roberts DL. Theory of multi-nozzle impactor stages and the interpretation of stage mensuration data. Aerosol Sci Technol. 2009;43(11):1119–29.
Byron PR, Weers JG, Clark AR, Sandell D, Mitchell JP. Achieving deposition equivalence: the state of the art. In: Dalby RN, Peart J, Suman JD, Young PM, Traini D, editors. Respiratory drug delivery Europe 2017. River Grove: Davis Horwood Publishing LLC; 2017. p. 101–18.
Olsson B, Asking L. Methods of setting and measuring flow rates in pharmaceutical impactor experiments. Pharm Forum. 2003;29(3):879–84.
Roberts DL, Mitchell JP. The effect of non-ideal impactor stage collection efficiency curves on the interpretation of the size of inhaler-generated aerosols. AAPS PharmSciTech. 2013;14(2):497–510.
Zhou Y, Sun J, Cheng Y-S. Comparison of deposition in the USP and physical mouth-throat models with solid and liquid particles. J Aerosol Med Pulmon Drug Deliv. 2011;24(6):277–84.
Twomey S. Comparison of constrained linear inversion and an iterative nonlinear algorithm applied to the indirect estimation of particle size distributions. J Comput Phys. 1975;18:188–200.
Picknett RG. A new method of determining aerosol size distributions from multistage sampler data. J Aerosol Sci. 1972;3:185–98.
Nichols SC, Mitchell JP, Shelton CM, Roberts DL. Good cascade impactor practice (GCIP) and considerations for “in-use” specifications. AAPS PharmSciTech. 2013;14(1):375–90.
Roberts DL, Maidment M, Copley MA. Improved protocol for relating impactor stage pressure drop to the suitability for routine use. Drug delivery to the lungs. Edinburgh: The Aerosol Society; 2017. p. 94–7.
Williams G, Blatchford C, Mitchell JP. Evaluation of nasal inlet ports having simplified geometry for the pharmacopeial assessment of mass fraction of dose likely to penetrate beyond the nasopharynx: a preliminary investigation. AAPS PharmSciTechnol. 2018; 19(8):3723–3733
Author information
Authors and Affiliations
Corresponding author
Additional information
Guest Editors: Philip J. Kuehl and Stephen W. Stein
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Roberts, D.L., Mitchell, J.P. Measurement of Aerodynamic Particle Size Distribution of Orally Inhaled Products by Cascade Impactor: How to Let the Product Specification Drive the Quality Requirements of the Cascade Impactor. AAPS PharmSciTech 20, 57 (2019). https://doi.org/10.1208/s12249-018-1276-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12249-018-1276-9