
Abstract
A survey conducted by the Therapeutic Product Immunogenicity (TPI) community within the American Association of Pharmaceutical Scientists (AAPS) posed questions to the participants on their immunogenicity risk assessment strategies prior to clinical development. The survey was conducted in 2 phases spanning 5 years, and queried information about in silico algorithms and in vitro assay formats for immunogenicity risk assessments and how the data were used to inform early developability effort in discovery, chemistry, manufacturing and control (CMC), and non-clinical stages of development. The key findings representing the trends from a majority of the participants included the use of high throughput in silico algorithms, human immune cell-based assays, and proteomics based outputs, as well as specialized assays when therapeutic mechanism of action could impact risk assessment. Additional insights into the CMC-related risks could also be gathered with the same tools to inform future process development and de-risk critical quality attributes with uncertain and unknown risks. The use of the outputs beyond supporting early development activities was also noted with participants utilizing the risk assessments to drive their clinical strategy and streamline bioanalysis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With the recent advent of novel and next generation complex biotherapeutics that may be immune modulatory, immunogenicity risk assessment during early and late stage development has become a common exercise. One of the risk factors evaluated during such early assessment is the potential for such biotherapeutics to be immunogenic in the clinic. With the awareness that the causes of immunogenicity can be multifactorial and can span from early discovery to preclinical and clinical development, risk factors have been identified through focused preclinical assessments and validated by studies of approved biotherapeutics. The identification of such risk factors requires specific in silico, in vitro, and/or in vivo tools. In 2016, the Immunogenicity Prediction Action Program Area (IPAPA) working group members from American Association of Pharmaceutical Scientists (AAPS) and the Non-Clinical Immunogenicity Risk Assessment working group members from European Immunogenicity Platform (EIP) conducted a survey (phase 1 survey) to better understand the current use and application of such tools and assays. The outcome of the survey results was intended to establish “best practices” to standardize and harmonize the outputs of these risk assessment assays and their applications during drug development.
Most individuals responding to the initial survey belonged to pharmaceutical or biotechnology companies (58.6%) followed by immunogenicity analysis and immune monitoring vendors (13.8%), contract research organizations (CRO), students/trainees/fellows, consultants, regulatory affairs, and academia (contributing approximately ~ 20%). The applications of such assays ranged from discovery through post-marketing activities and the survey respondents included scientists performing the assays and generating the relevant immune activation data, as well as those who used the data to support writing of risk assessment strategy documents and guide bioanalytical strategies during development.
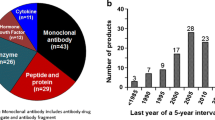
The first survey showed that 70% of the member companies were using some type of predictive assays preclinically (Fig. 1a). Preclinical in vitro immunogenicity assays were used as tools to serve variety of purposes, including protein engineering strategies for deimmunization, contributing to lead drug candidate selection as part of developability, and development of clinical immunogenicity assay strategy (Fig. 1b). However, there was no alignment on the methods used or data interpretation and criteria used for reporting of predicted risks. Some key gaps were identified related to the use of these assays and the lack of endorsement and application during preclinical drug development (Fig. 2). The biggest gap was related to the translatability and predictive value of the preclinical risk assessment data in clinic (75.9%) followed by lack of standardization and benchmarking (48.3%) and high variability (48.3%) for these assays. The cost or return on investment (30%) and the lack of high throughput assays (20.7%), all of which may impact the critical developability timelines was also cited as potential cause for lack of endorsement to adopt these approaches.

In vitro immunogenicity risk assessment assays employed in pharmaceutical industry. a Type of assays used and b purpose are indicated. MAPPs, MHC-associated peptide proteomics; PBMC, peripheral blood mononuclear cells; DC, dendritic cells

Gaps or barriers to broader implementation of immunogenicity screening from the first survey conducted in 2016
The findings from this first survey led to a focused effort in the AAPS soon after the first survey was completed to develop a “best practice” and “harmonized” approach for these risk assessment tools. The biopharmaceutical development community, working collaboratively as part of AAPS IPAPA working group, currently known as the Therapeutic Product Immunogenicity (TPI) community, initiated an effort to address one of the cited gaps related to standardization and benchmarking of such assays. As part of this effort, an additional granular survey (phase 2 survey) where information on assay set up, components, and conditions was solicited from the members. The intent with this second phase was to better understand the assay variability and factors that contribute to the assay variability across labs. Some key questions posed were around the donors and their variability based on baseline responses (underlying immune status) and genetic makeup (human leukocyte antigen, HLA), use of relevant standard positive and negative controls for the assays at different phases of immune response (innate and adaptive), criteria for a positive or negative response, and reference ranges or any streamlined and best practices around presenting the dataset in a standardized approach to facilitate comparisons.
Survey Method and Data Presentation
This survey was conducted by email in two phases among the membership of the AAPS IPAPA working group (currently referred to as AAPS TPI community) and the EIP. The phase 1 survey was conducted in 2016 and was designed to assess interest in predictive tools in the pharmaceutical industry. The phase 2 survey was conducted in 2018–2021 and focused primarily on assay methods under each risk assessment strategy and their potential application to improve the developability and discovery/development process. The participants for the phase 2 survey included large pharmaceuticals, biotechnology companies, and academic institutions.
Results
The immunogenicity risk assessment strategy provides a roadmap to identify risks at different development stages of a biotherapeutic by using in silico algorithms as well as cell-based in vitro assays. Such assessments are being increasingly employed early in development to understand potential intrinsic and extrinsic risk factors related to structure and pharmacology, post-translational modifications during process development and liabilities acquired during manufacturing, formulation, and handling (device and storage-related factors). In addition, patient population and disease state may further exacerbate risks. The outlined risks and many more being identified for novel modalities like multi-domain biotherapeutics, cell therapies, and nucleic acid-based therapies have brought forth the need to understand which tools can help de-risk such liabilities upfront to ensure quality by design (QbD). Such efforts require platforms that can be implemented through discovery to development and beyond in an integrated approach.
A survey conducted by the AAPS TPI community probed the use of immunogenicity risk assessment tools and their applications and the survey findings are summarized below.
In Silico Algorithms
The survey participants provided their input on the nature of algorithms used to predict the intrinsic sequence-based risks based on non-self epitope content, lack of sequence alignment to self, lack of cross reactivity to T-cell repertoires, etc. The information on the algorithms used and the data obtained through such tools were mined. The BLAST tool that aligned the sequence of interest with germline was the most used (almost 90%) followed by experimental confirmation by MHC-associated peptide proteomics (MAPPs) (60%), and algorithms trained on peptide-MHC-based interactions (IEDB, The Immune Epitope Database, other commercially available tools as well as tools internally developed by sponsors) (Fig. 3a).

In silico risk assessment tools being used in the pharmaceutical industry (a) and how the in silico data and information are applied and interpreted (b). IEDB, The Immune Epitope Database; MHC, major histocompatibility complex; TCR, T cell receptor; MAPPs, MHC-associated peptide proteomics; HLA, human lymphocyte antigen
There was a > 90% consensus among all survey participants on the use of the data from these tools for selection of the most optimal candidate for further development through candidate ranking based on affinity of their peptides to MHC peptide binding groove and promiscuity of HLA alleles (Fig. 3b). A similar high response was seen for use of the tools to further optimize/re-engineer the sequence. The information related to understanding the anchor points within the HLA pocket and cross-reactivity to T-cell repertoire also scored high in the survey with about 80% of responders considering that as important information to gather. However, only 30% of the participants were using the in silico information to understand clinical immunogenicity.
In Vitro Cell-Based Assays
The survey participants provided their input on the use of in vitro assays during drug development. The DC (dendritic cell):T cell format T cell proliferation/activation assays were the most used assays (> 70% responders) followed by innate activation assays, MAPPs, non-depleted or depleted peripheral blood mononuclear cells (PBMC) format T cell proliferation/activation assays, whole blood assay, and DC internalization assay.
PBMC Format T Cell Proliferation/Activation Assays
T cell proliferation assays can use one of two common formats, PBMC format, or DC:T format. In the PBMC format, the test article is directly added to the PBMC cell culture and CD4 + T cell activation or proliferation is measured on day 7–10. This assay format is relative straight forward and substantially less labor intensive than a DC: T cell assay format. One consideration for this assay format should be that the therapeutic mechanism of action can have an impact on T cell proliferation. However, the PBMC format can also circumvent this interference by testing peptides identified by MAPPs rather than the intact biotherapeutic (1).
Four organizations provided information about the PBMC format (Table I). PBMCs were harvested from whole blood or buffy coat by gradient. As quality control, cell viability was checked. An isotype control or medium treatment was used as negative control, and T cell proliferation was studied by FACS using CFSE staining or cytokine enzyme-linked immunosorbent spot (ELISpot). Nonetheless, harmonization is needed for many other assay parameters, including number of cells, number of donors, depletion of CD8 + T cells, sample concentration, and incubation duration. One major gap that was identified was the lack of standard reference materials and controls (Table I).
DC:T Format T Cell Proliferation/Activation Assays
A modification of the PBMC assay is the DC-T cell assay where monocyte-derived dendritic cells (MoDC) are pulsed with biotherapeutic followed by the maturation of the dendritic cells to upregulate HLA. After the removal of the biotherapeutic from the media, these dendricit cells are incubated with their autologous PBMC’s for 7–10 days. Read out of T cell activation can be done by flow cytometry through activation markers, cytokine released in the supernatant, or CSFE dilution.
Ten respondents to this survey reported the use of DC:T cell assay format as the primary method to assess the immunogenicity risk of biotherapeutics during preclinical drug development. In general, assay parameters for this format were remarkably similar. Bead-based monocyte isolation, donor selection based on HLA DRB*1 alleles, and DC differentiation protocol are nearly identical across surveyed organizations (Table II).
As summarized in Table II, most organizations used 40–50 PBMC donors, to ensure coverage of the diverse HLA alleles in the human population as well as to minimize assay-to-assay variability incurred from donor-to-donor variation. The organizations that used a smaller number of donors (10,11,12,13,14,15,16,17,18,19,20) used this format in combination with the PBMC assay format. The DC maturation protocols used both PGE (prostaglandin E) or TNFα interchangeably with the exception for biotherapeutics where TNFα was the target and could suppress the maturation and upregulation of HLA on the DC. The number of PBMC used in the assay showed a relative larger range from 3*105 to 1.6*106 cells/well. The frequency of naïve antigen specific CD4 + T cells has been shown to be in the 1:10,000–1,000,000 range (2). Hence, amplifying the number of such antigen-specific cells in the assay is needed to represent the in vivo situation (3). CD8 + T cells were depleted from the PBMC by 75% of the responders to improve CD4 T cell activation assay background for immunogenicity risk assessment of biotherapeutics (1). Test article concentrations used to pulse the immature DC varied widely (5–450 µg/mL) which were optimized based on impact on assay performance and need to minimize reagent consumption. Lastly, most of the participants (75%) used CD4 + T cell proliferation monitored through CFSE dilution as the assay readout while a minority used secreted cytokine measurements as a readout as well. Multiplexed assessment of cytokine profiles, while more complex, enabled further characterization of the response and mechanisms (4).
For T cell assays, positive controls were usually monoclonal antibodies that have shown a clear immunogenic profile in the clinic in order to establish translational correlation. Bococizumab, ATR-107 (Anti IL-21R), and anti-integrin A33 are being used by various organizations. KLH as a highly immunogenic protein or PADRE as a peptide control is also used (5). Limited lab to lab assay results for these positive controls have shown excellent reproducibility even with the differences in assay format as well as the variation in PBMC derived from diverse human donors (Fig. 4). Batch to batch variations for positive controls have been reported (anecdotally), particularly when these control antibodies are produced in small batches.

DC-T cell assay positive control performance. KLH, keyhole limpet hemocyanin
DC Internalization Assay
Internalization by antigen presenting cells (APC) is necessary to initiate CD4 + T cell dependent anti-drug antibody responses. DCs are professional and potent antigen presenting cells and often considered the primary APC responsible for propagation of long-term immune response. Therefore, studying DC internalization helps understand the immunogenicity risk (6,7,8). Two companies responded in the survey (Table III). Immature DCs (iDC) were generated using standard protocols (9). Briefly, PBMCs were isolated from fresh leukapheresis or whole blood using density gradient, followed by selection of CD14 + monocytes. CD14 + monocytes were cultured with 10% FBS medium and induced to iDC using GM-CSF and IL-4. The purity of monocytes and viability and phenotype of iDC were monitored as part of quality control. Internalization was analyzed by FACS and microscopic imaging with the latter for visualization of intracellular trafficking, i.e., colocalization with endosome and lysosome. Mean/median fluorescence intensity (MFI) or percentage of fluorescence positive cells was utilized to quantify internalization and enable ranking of molecules. An isotype matched antibody could serve as a negative control; a well characterized proprietary antibody with an established immunogenic potential could be used as a positive control. Multiple donors (3,4,5,6,7,8,9,10) were usually used. Study concentrations (2–50 µg/mL) and durations (1–24 h) varied, which is not unexpected as conditions must be optimized for each format.
Unlike other assays in which samples can be tested directly, fluorescent labels are required to study internalization and intracellular trafficking. Although details were not provided in the survey, this is where the major distinction resides according to publications (6,7,8). Internalization may be studied with a regular fluorescence tag (e.g., Alexa Fluor 647), a pH sensitive dye (e.g., pHrodo), or Förster Resonance Energy Transfer (FRET) pair. It is noted here that different detection methods provide different information about internalization pathways and/or destinations. In addition, test articles can be directly labeled or a labeled second probe (e.g., anti-Fc) can be used.
Innate Activation Assay
Activation signals (cytokines and co-stimulation molecules) from innate immune cells can prime the adaptive phase immune response by engaging the immune cells (T and B cells) in the primary and secondary lymphoid organs, which is a prerequisite for T cell activation (10). A biotherapeutic’s potential to activate innate immune cells, including DCs and monocytes, presents as a risk factor for mounting an immune response in the clinic. Studying innate activation is particularly important for molecules whose mechanism of action may require targeting immune cell surface molecules. Such direct engagement with immune cells can cause immune activation. Innate immune responses can also be triggered through danger signals, i.e., damage associated molecular patterns (DAMP) or pathogen associated molecular patterns (PAMP). Danger signals do not necessarily come from the molecule itself; it could come from product and process-related attributes, including aggregates and microbial contaminants (11, 12). Innate activation assays are commonly integrated into immunogenicity assessment platforms. However, assay formats and parameters used vary based on the nature of innate response modulator (Table IV).
Several organizations use multiple innate activation assays and different test concentrations in different assays. Many different cells and cell lines were used, including total PBMC, CD14 + monocytes, MoDC, Raw Blue cells, THP1-Xblue cells, and innate receptor (e.g., TLR) transfected cell lines. Cell sources for PBMC (and monocytes) included whole blood, leukapheresis, and buffy coat from normal human donors. Cell lines may be purchased directly from ATCC. Cell numbers varied from 0.2 million to 2.0 million per test article. A wide range of sample concentrations were used, ranging from 2 to 250 µg/mL. These were selected based on the assay performance but not to mimic the actual concentration of the in vivo dose. When PBMC, primary monocytes, or MoDC were used, most companies used more than 10 donors but 3–6 donors were deemed sufficient by two companies. Despite these discrepancies, there were also consensus with regard to medium (10% FBS RPMI), replicate number (duplicate or triplicate), treatment duration (24–48 h), readout (activation marker by FACS and cytokines by multiplex cytokine assay), and positive criteria (simulation index and percentage of positive donors).
The major gap with innate activation assays is the lack of standardized biologically relevant positive controls. Currently, TLR4 ligand (e.g., LPS) and neo-antigen proteins (keyhole limpet hemocyanin) were employed as positive controls. While they can serve as “technical” controls to confirm assay performance, they are not biologically relevant as they do not reflect the mechanisms and properties of test articles (biotherapeutic) or relevant residual impurities that mimic PAMPs. Establishing biologically relevant positive controls would facilitate assay harmonization and consensus around data comparison.
It is noted here that we do not recommend a particular assay format, rather a fit-for-purpose assay should be adapted based on the modality and MOA of the test articles. Innate activation assays are gaining more interest due to the emergence of novel modalities. For instance, it is well documented that Adeno-associated virus (AAV)-based gene therapies could activate innate immunity through interactions with TLR2 (capsid) and TLR9 (genome) (13). Therefore, a TLR-transfected cell line may be a more relevant mode for novel modalities. Similarly, residuals from lentivirus, Cas, and AAV used for editing and knock in or out genes of interest in engineered chimeric antigen receptor T cells could also pose a risk and would require cells that can evaluate innate response activation through diverse TLRs.
Whole Blood Assay
The most prevalent use of whole blood based assays has been to predict cytokine release syndrome (CRS)-related events. Four companies responded in the survey with high level of consensus to the use of such assays for understanding risks of CRS (Table V). The assay entails use of fresh whole blood from more than 10 donors. After incubation with test article at 10–100 µg/mL for 1–2 days, the concentrations of proinflammatory cytokines, including IL-1β, IL-6, IFN-γ, and TNF-α, from the supernatant were determined using multiplex cytokine assays (Luminex or MSD-ELISA). Medium, buffer, or isotype control were used as negative control. Some good positive controls include alemtuzumab, muromonab-CD3, and TGN1412, which had shown high CRS rates in the clinic (14,15,16,17,18). It is noteworthy that these three antibodies had been qualified as suitable controls by an international collaborative project (18). Stimulation index over negative control and percentage of positive donors were reported and used as thresholds. The survey found that the whole blood assay could also be adopted for evaluating the risk due to product-related deviations of critical quality attributes and other residuals/contaminants generated during manufacturing, shipping/handling, and device and administration-related stresses. The next generation of biotherapeutics like cell and gene therapies will encounter much more of these innate response modulating impurities. Similar to the immune modulatory therapeutic proteins, engagement of immune cells by such attributes may activate downstream signaling (14, 15, 17, 19). However, to repurpose the whole blood assay for immunogenicity risk assessment of biotherapeutics and associated produce and process-related attributes, fit-for-purpose positive controls and analytes shall be established and qualified.
MAPPs
In vitro HLA elution assays or MAPPs assays can elucidate the processing and MHC presentation of a biotherapeutic and thereby provide insights into which peptides are “visible” to the adaptive immune system (20, 21). In this assay, antigen-presenting cells are isolated and pulsed with a biotherapeutic followed by cell lysis, HLA/peptide complexes isolation, and LC/MS identification of the HLA-associated peptides.
Survey data shows that all participating organizations use MoDC isolated from PBMCs as APC, use a GM-CSF + IL-4 protocol to generate iDC, and use either LPS or TNFα to mature iDC and upregulate class II MHC expression (Table VI). In order to represent the HLA variability in the human population, 10–25 PBMC donors were used per assay run. This is considerably fewer than the number of PBMC donors that were used for in vitro T cell proliferation assays (10–50 donors). The low number of donors in such assays is likely due to limitations associated with the time of processing and presentation associated with large numbers of monocytes (2–10 million) per test article needed for this assay. A large number of DC is needed to make sure to capture the unique peptides from biotherapeutics. During this assay, a large number of endogenous peptides are also presented on MHC class II which need to be separated out from biotherapeutic-generated peptides. The total number of identified peptides was similar at 5000–7000 unique peptides across survey participants (22).
The assay parameter with the biggest range identified in this survey was the pulsing concentration of the biotherapeutic to the iDC, ranging from 15 to 100 µg/mL (Table VI). It remains unclear from this survey how this specific ratio of concentration to cell number effects assay sensitivity. For many laboratories, obtaining sufficient quantities of high-quality test material for using MAPPs during the discovery phase of biotherapeutic can pose a challenge, and therefore optimization of pulsing concentration can potentially increase the utility of this assay.
Discussion
Within the pharmaceutical industry, preclinical immunogenicity risk assessment tools and assays have been widely adapted and implemented to inform the selection and design of biotherapeutic molecules with a lower probability to induce clinical immunogenicity risk. The most common application of the tools is to rank order and optimize candidate molecules during early stages of development. The outputs from such risk assessments have also been used to develop clinical immunogenicity assessment strategy and included in the Integrative Summary of Immunogenicity (ISI) to help formulate and/or justify bioanalytical strategy. Therefore, the risk assessment assays must be robust, reproducible, and fit-for-purpose to inform decision making, especially when data is used to develop phase-appropriate clinical immunogenicity assessment strategy. For instance, for a molecule with no or low foreign epitope content in a sequence, a relatively low DC internalization, favorable critical quality attributes that would not contribute to innate activation, lack of neoepitopes identified by MAPPs, and minimal T cell activation, the clinical ADA assay development and validation and clinical sample analysis can be staged or gated until phase 2 trial begins. To support such rationale to streamline immunogenicity testing, there should be a level of confidence in the predictive assays which should be at least analytically qualified before use.
Survey results show that in silico immunogenicity tools are widely used in drug discovery for candidate selection. However, only 30% of the responders indicated that they are used to understand clinical immunogenicity. The more recent development and integration of orthogonal in silico methods combining HLA complex binding and stability, antigen processing and presentation, tolerance mechanisms, and systems biology models make it likely that these methods will see greater utility in assessing and understanding clinical immunogenicity. The deleterious impact of clinical immunogenicity as observed for recombinant protein-based therapies like FVIII in hemophilia and enzyme replacement therapies in Pompe disease led to deimmunization of the immunogenic epitopes from such proteins through targeted mutations to remove immunogenic epitopes (23, 24). The deimmunization strategy would benefit the next generation of protein-based biologics by avoiding such liabilities identified through clinical experience.
Survey results showed that a panel of routinely used in vitro immunogenicity assays. Differences were noted, but similar assay procedures and parameters were used by different organizations to establish acceptance criteria and identifying positive responses. The cross-organization assay performance data was not sufficient to draw conclusions. Two major gaps, namely lack of assay harmonization and lack of biologically relevant reference materials as assay controls, were identified. These main findings are consistent with those in the recent publication from EIP (5). Innate activation assay (n = 10) and DC:T cell activation assay (n = 10) were used as examples here. For innate activation assays, cell type, cell density, and sample concentration are different across respondents. LPS is widely used as a technical positive control, but it may not be biologically relevant or fit-for-purpose. For the DC:T cell assay, while parameters like number of donors, concentration of pulsing antigen, and ratio of pulsed DC to PBMC (or T cells) are very similar across participants, the differences are mainly attributed to the number of PBMC required for the assay setup for co-cultures. KLH is the most common positive control. In addition, clinically immunogenic antibodies, like anti-PCSK9 (bococizumab) (25), anti-IL21R (ATR-107) (7, 26), and anti-integrin A33 (27), are also used as positive controls. KLH triggered positive T cell responses in 88% donors (average of responses from 9 different organizations). Bococizumab elicited positive T cell responses in 59% donors (average of responses from 3 different organizations). Despite relatively small sample sizes, the data are encouraging considering each organization follows its own assay procedures and uses different positive control preparations. It is understandable that small changes in assay protocols may impact assay readout. In addition, assays are susceptible to batch-to-batch variability of control materials. Therefore, a harmonized assay protocol and a common panel of reference materials (ideally composed of high, moderate, low immunogenicity molecules) would greatly facilitate cross-organization comparison of assay variability and performance. Industry efforts are currently underway to produce common set standards for in vitro immunogenicity assay.
Assay readouts can also be influenced by engagement of immune modulatory targets and other downstream pathways susceptible to molecular MOA. For instance, check point inhibitors, including PD-1 antagonist antibodies, are likely to enhance T-effector cell responses through removal of the immune suppressive inhibitory effects. To eliminate the potential interference of specific cells, the in vitro assay setups must be modified to enable accurate risk assessment. Approaches to circumvent MOA interference in T cell activation assay include the use of DC: T-cell format or testing specific domains of the biotherapeutic like MAPP-derived peptides instead of the intact molecule that may retain the functional activity to engage with the cell surface receptors (1, 5). Likewise, an agonist antibody that targets a DC-associated cell surface antigen is likely to generate a positive innate activation signal. While that MOA shall be considered a risk, different types of cells, for instance, engineered THP1 cells, that do not express the target, can be used to study non-target related innate activation signals.
None of the survey participants analyzed HLA class I presented peptides as the vast majority of biotherapeutics in development were monoclonal antibodies and/or recombinant proteins where immunogenicity is mediated through an HLA class II-restricted CD4 + T cell driven anti-drug antibody response. With the increased popularity of novel modalities such as gene therapy and cellular therapies involving intracellularly expressed proteins as well as viral proteins, it is likely that the drug product developers and associated laboratories will adapt their MAPPs assays to incorporate HLA class I. Furthermore, none of the participants used other cell types, for instance B cells, in addition to MoDC as APC. Differential expression of cathepsins by different cell types make it likely that other cell types could show a different peptide repertoire, B cells in particular could be involved in processing and presenting IV dosed biotherapeutics (28). The in vitro assays and the cell types from healthy human donors used by survey participants may be adapted to support similar assessments using patient-derived cells exposed to the biologics where recall and memory responses can be evaluated and correlated to humoral responses. Such patient-derived responses would bridge the gap between the in vitro assays using naïve donors that are limited to capturing Teff responses and humanized mice models where humoral responses have been captured against biologics (29).
The preclinical immunogenicity assays may not require stringent validation requirements. Rather fit-for-purpose assay qualification can be performed (30, 31). The probability of immunogenicity risk using such assays can be demonstrated using a large set of molecules with available clinical immunogenicity data and improve the prediction accuracy by continuous monitoring and updates from clinical data as they become available. Assays must demonstrate an acceptable level of reproducibility. Assay data can be recorded to monitor assay performance and variability, and to establish assay control ranges. These data can also be readily available upon request by FDA if preclinical immunogenicity data are used to select candidate molecules and/or justify clinical immunogenicity strategy.
For peptides, proteins, and antibodies, CD4 + T cell dependent antibody responses have been the focus of immunogenicity assessment (9, 32). Therefore, preclinical assays that interrogate risk at each step of CD4 + T cell dependent pathway, namely innate activation, APC internalization and presentation, and CD4 + T cell activation, are implemented to assess immunogenicity risk (9, 32). Some preclinical assays can be adapted to novel modalities, including AAV, siRNA, mRNA, and CAR-T-based therapies (5). However, novel modalities may also possess new immune activation features and mechanisms, which may only be assessed with new tools and assays. One great example is AAV-based gene therapies. The unmethylated CpG motifs in the therapeutic genome can activate immune cells through Toll-like receptor 9 (TLR-9) and cause undesired immune responses (33, 34). Modification or reduction of CpG motifs may mitigate such risks (35). Assays that can detect innate activation by CpG may facilitate such efforts. Innate cells (primary cells or cell line) that have been used for proteins and antibodies and are known to respond to CpG can be adapted for AAV. Alternatively, TLR9-transfected cells can be employed for such purpose. AAV can trigger cytotoxic CD8 + T cell responses that are directed against the capsid and/or transgene product (36, 37). Applications of other tools and assays, for instance, in silico tools that can predict MHC-I-associated peptide proteomics and CD8 + T cell activation assay, are needed to assess CD8 + T cell response risk preclinically.
The risk assessment outputs generated by the surveyed tools above show the application beyond rank ordering and optimization of the candidates in discovery and development. With the validation of in silico-derived epitope predictions with corresponding human-derived in vitro assays both from naïve human donors and patients dosed with biologics, the translation to clinical outcome may be possible. Particularly, knowledge of high MHC class I and class II binders can help stratify the patients based on the risks prior to enrolling and ensure a close monitoring of such subjects in clinic for immune mediated adverse events and impact on safety and efficacy. The reverse translation of information from such subjects and epitopes eluted from patient’s immune cells could help to optimize the next generation of biologics by removing such liabilities. The recent guidance recommends for a risk assessment strategy to be provided at the time of new IND applications and an ongoing evaluation of risks during the different stages of clinical development (38). Risk assessment tools will be needed to mitigate identified liabilities during process development and clinical trials. Recent health authority led workshops and requests from sponsors as part of pre IND/Interact meetings suggest the need for development of qualified assays and criteria for controls and outputs need to be established robustly and harmonized.
Conclusions
The use of risk assessment tools prior to clinical development has become more prevalent in the last decade to assess developability and enable QbD initiatives. The AAPS TPI community has conducted 2 surveys to assess the use of these tools and their applications in different stages of drug discovery and development. The first survey conducted more than 5 years ago provided a better understanding of the gaps and reservations for use of such tools to predict immunogenicity in the clinic. The second survey was able to pose more granular and in-depth questions on the type of tools employed and their applications in understanding risks at the different stages of development. The trends that emerge include the use of a multi-tiered approach to risk to address limitations of one approach over the next. Specifically, the outputs from algorithm-based risk assessments that are considered conservative can be complemented with specialized in vitro assays to further delve into processing, presentation, and MOA-related questions. To operationalize these assays, the preference is to work with assays that require minimal processing; however, specialized formats, for instance, DC:T, are preferred to address questions around MOA or pharmacology. This survey also suggests that the industry is open to harmonization of tools and their applications and embracement of the risk assessment approach to drive clinical strategy.
The surveys discussed in this manuscript were designed, conducted, and discussed over the time period of 2016–2022 within the TPI community of the AAPS and represent the state of the industry at this time. Ongoing research is likely to further develop and optimize these assays as shown in recent publications (39, 40).
References
Walsh RE, Lannan M, Wen Y, Wang X, Moreland CA, Willency J, et al. Post-hoc assessment of the immunogenicity of three antibodies reveals distinct immune stimulatory mechanisms. mAbs. 2020;12(1):1764829.
Jenkins MK, Moon JJ. The role of naive T cell precursor frequency and recruitment in dictating immune response magnitude. J Immunol. 2012;188(9):4135–40.
Delluc S, Ravot G, Maillere B. Quantitative analysis of the CD4 T-cell repertoire specific to therapeutic antibodies in healthy donors. FASEB J. 2011;25(6):2040–8.
Hamze M, Meunier S, Karle A, Gdoura A, Goudet A, Szely N, et al. Characterization of CD4 T cell epitopes of infliximab and rituximab identified from healthy donors. Front Immunol. 2017;8:500.
Ducret A, Ackaert C, Bessa J, Bunce C, Hickling T, Jawa V, et al. Assay format diversity in pre-clinical immunogenicity risk assessment: toward a possible harmonization of antigenicity assays. MAbs. 2022;14(1):1993522.
Deora A, Hegde S, Lee J, Choi CH, Chang Q, Lee C, et al. Transmembrane TNF-dependent uptake of anti-TNF antibodies. MAbs. 2017;9(4):680–95.
Xue L, Hickling T, Song R, Nowak J, Rup B. Contribution of enhanced engagement of antigen presentation machinery to the clinical immunogenicity of a human interleukin (IL)-21 receptor-blocking therapeutic antibody. Clin Exp Immunol. 2016;183(1):102–13.
Wen Y, Cahya S, Zeng W, Lin J, Wang X, Liu L, et al. Development of a FRET-based assay for analysis of mAbs internalization and processing by dendritic cells in preclinical immunogenicity risk assessment. AAPS J. 2020;22(3):68.
Jawa V, Terry F, Gokemeijer J, Mitra-Kaushik S, Roberts BJ, Tourdot S, et al. T-cell dependent immunogenicity of protein therapeutics pre-clinical assessment and mitigation–updated consensus and review 2020. Front Immunol. 2020;11(1301):1–23.
Murphy K, Casey W. Janeway’s Immunobiology. Ninthe. New York: Garland Science; 2017.
Wen Y, Jawa V. The impact of product and process related critical quality attributes on immunogenicity and adverse immunological effects of biotherapeutics. J Pharm Sci. 2021;110(3):1025–41.
Jarvi NL, Balu-Iyer SV. Immunogenicity challenges associated with subcutaneous delivery of therapeutic proteins. BioDrugs. 2021;35(2):125–46.
Colella P, Ronzitti G, Mingozzi F. Emerging issues in AAV-mediated in vivo gene therapy. Mol Ther Methods Clin Dev. 2018;8:87–104.
Grimaldi C, Finco D, Fort MM, Gliddon D, Harper K, Helms WS, et al. Cytokine release: a workshop proceedings on the state-of-the-science, current challenges and future directions. Cytokine. 2016;85:101–8.
Shimabukuro-Vornhagen A, Gödel P, Subklewe M, Stemmler HJ, Schlößer HA, Schlaak M, et al. Cytokine release syndrome. J Immunother Cancer. 2018;6(1):56.
Vessillier S, Eastwood D, Fox B, Sathish J, Sethu S, Dougall T, et al. Cytokine release assays for the prediction of therapeutic mAb safety in first-in man trials–whole blood cytokine release assays are poorly predictive for TGN1412 cytokine storm. J Immunol Methods. 2015;424:43–52.
Finco D, Grimaldi C, Fort M, Walker M, Kiessling A, Wolf B, et al. Cytokine release assays: current practices and future directions. Cytokine. 2014;66(2):143–55.
Vessillier S, Fort M, O’Donnell L, Hinton H, Nadwodny K, Piccotti J, et al. Development of the first reference antibody panel for qualification and validation of cytokine release assay platforms - report of an international collaborative study. Cytokine X. 2020;2(4): 100042.
Lee DW, Gardner R, Porter DL, Louis CU, Ahmed N, Jensen M, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Blood. 2014;124(2):188–95.
Quarmby V, Phung QT, Lill JR. MAPPs for the identification of immunogenic hotspots of biotherapeutics; an overview of the technology and its application to the biopharmaceutical arena. Expert Rev Proteomics. 2018;15(9):733–48.
Kropshofer H, Singer T. Overview of cell-based tools for pre-clinical assessment of immunogenicity of biotherapeutics. J Immunotoxicol. 2006;3(3):131–6.
Paul S, Lindestam Arlehamn CS, Scriba TJ, Dillon MB, Oseroff C, Hinz D, et al. Development and validation of a broad scheme for prediction of HLA class II restricted T cell epitopes. J Immunol Methods. 2015;422:28–34.
Zinsli LV, Stierlin N, Loessner MJ, Schmelcher M. Deimmunization of protein therapeutics - recent advances in experimental and computational epitope prediction and deletion. Comput Struct Biotechnol J. 2021;19:315–29.
Moise L, Song C, Martin WD, Tassone R, De Groot AS, Scott DW. Effect of HLA DR epitope de-immunization of factor VIII in vitro and in vivo. Clin Immunol. 2012;142(3):320–31.
Ridker PM, Tardif JC, Amarenco P, Duggan W, Glynn RJ, Jukema JW, et al. Lipid-reduction variability and antidrug-antibody formation with Bococizumab. N Engl J Med. 2017;376(16):1517–26.
Hua F, Comer GM, Stockert L, Jin B, Nowak J, Pleasic-Williams S, et al. Anti-IL21 receptor monoclonal antibody (ATR-107): safety, pharmacokinetics, and pharmacodynamic evaluation in healthy volunteers: a phase I, first-in-human study. J Clin Pharmacol. 2014;54(1):14–22.
Welt S, Ritter G, Williams C Jr, Cohen LS, John M, Jungbluth A, et al. Phase I study of anticolon cancer humanized antibody A33. Clin Cancer Res. 2003;9(4):1338–46.
Stern LJ, Santambrogio L. The melting pot of the MHC II peptidome. Curr Opin Immunol. 2016;40:70–7.
Jiskoot W, Kijanka G, Randolph TW, Carpenter JF, Koulov AV, Mahler HC, et al. Mouse models for assessing protein immunogenicity: lessons and challenges. J Pharm Sci. 2016;105(5):1567–75.
Wickramarachchi D, Steeno G, You Z, Shaik S, Lepsy C, Xue L. Fit-for-purpose validation and establishment of assay acceptance and reporting criteria of dendritic cell activation assay contributing to the assessment of immunogenicity risk. AAPS J. 2020;22:114.
Wullner D, Zhou L, Bramhall E, Kuck A, Goletz TJ, Swanson S, et al. Considerations for optimization and validation of an in vitro PBMC derived T cell assay for immunogenicity prediction of biotherapeutics. Clin Immunol. 2010;137(1):5–14.
Jawa V, Cousens LP, Awwad M, Wakshull E, Kropshofer H, De Groot AS. T-cell dependent immunogenicity of protein therapeutics: preclinical assessment and mitigation. Clin Immunol. 2013;149(3):534–55.
Bertolini TB, Shirley JL, Zolotukhin I, Li X, Kaisho T, Xiao W, et al. Effect of CpG depletion of vector genome on CD8(+) T cell responses in AAV gene therapy. Front Immunol. 2021;12: 672449.
Konkle BA, Walsh CE, Escobar MA, Josephson NC, Young G, von Drygalski A, et al. BAX 335 hemophilia B gene therapy clinical trial results: potential impact of CpG sequences on gene expression. Blood. 2021;137(6):763–74.
Wright JF. Codon modification and PAMPs in clinical AAV vectors: the tortoise or the hare? Mol Ther. 2020;28(3):701–3.
Verdera HC, Kuranda K, Mingozzi F. AAV vector immunogenicity in humans: a long journey to successful gene transfer. Mol Ther. 2020;28(3):723–46.
Mingozzi F, High KA. Immune responses to AAV vectors: overcoming barriers to successful gene therapy. Blood. 2013;122(1):23–36.
FDA (2014) Guidance for industry: immunogenicity assessment for therapeutic protein products. https://www.fda.gov/media/85017/download. Accessed on April 25, 2021.
Siegel M, Steiner G, Franssen LC, Carratu F, Herron J, Hartman K, et al. Validation of a dendritic cell and CD4+ T cell restimulation assay contributing to the immunogenicity risk evaluation of biotherapeutics. Pharmaceutics. 2022;14:2672.
Cohen S, Myneni S, Batt A, Guerrero J, Brumm J, Chung S. Immunogenicity risk assessment for biotherapeutics through in vitro detection of CD134 and CD137 on T helper cells. MAbs. 2021;13(1):1898831.
Author information
Authors and Affiliations
Contributions
Jochem G. and Shibani M–K. conceived the project and performed the survey. Jochem G., Yi W., and Vibha J. analyzed the data and wrote the manuscript. Jochem G., Shibani M–K., Theresa G., Swati G., Shan C., Alan G., Seema K., Kasper L., Karen L., Jennie L., Qui P., Robin W., Brian R., Michael S., Inderpal S., Sophie T., Mark K., Laurent M., and Sofie P. responded to the survey and provided data. All authors reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Jochem G. and Vibha J. are employees of Bristol Myers Squibb, Yi W., Robin W., and Laurent M. are employees of Eli Lilly and Company. Shibani Mitra-Kaushik is an employee of Takeda Pharmaceuticals. Theresa Goletz is an employee of GSK. Bonita Rup works as an independent consultant. Swati Gupta is employee of AbbVie. Jennie Lill and Qui Phung are employees of Genentech. Mark Kroenke is an employee of Amgen. Seema Kumar is an employee of EMD Serono. Alan Goggins is an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Karen Liao is an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA currently, and was employed by GSK at survey participation.
Disclaimer
The views and opinions expressed in this manuscript do not represent the views and opinions of their employers.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gokemeijer, J., Wen, Y., Jawa, V. et al. Survey Outcome on Immunogenicity Risk Assessment Tools for Biotherapeutics: an Insight into Consensus on Methods, Application, and Utility in Drug Development. AAPS J 25, 55 (2023). https://doi.org/10.1208/s12248-023-00820-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12248-023-00820-7