
Abstract
Developing mathematical models to predict changes in ocular bioavailability and pharmacokinetics due to differences in the physicochemical properties of complex topical ophthalmic suspension formulations is important in drug product development and regulatory assessment. Herein, we used published FDA clinical pharmacology review data, in-house, and literature rabbit pharmacokinetic data generated for dexamethasone ophthalmic suspensions to demonstrate how the mechanistic Ocular Compartmental Absorption and Transit model by GastroPlus™ can be used to characterize ocular drug pharmacokinetic performance in rabbits for suspension formulations. This model was used to describe the dose-dependent (0.01 to 0.1%) non-linear pharmacokinetic in ocular tissues and characterize the impact of viscosity (1.67 to 72.9 cP) and particle size (5.5 to 22 μm) on in vivo ocular drug absorption and disposition. Parameter sensitivity analysis (hypothetical suspension particle size: 1 to 10 μm, viscosity: 1 to 100 cP) demonstrated that the interplay between formulation properties and physiological clearance through drainage and tear turnover rates in the pre-corneal compartment drives the ocular drug bioavailability. The quick removal of drug suspended particles from the pre-corneal compartment renders the impact of particle size inconsequential relative to viscosity modification. The in vivo ocular absorption is (1) viscosity non-sensitive when the viscosity is high and the impact of viscosity on the pre-corneal residence time reaches the maximum physiological system capacity or (2) viscosity sensitive when the viscosity is below a certain limit. This study reinforces our understanding of the interplay between physiological factors and ophthalmic formulation physicochemical properties and their impact on in vivo ocular drug PK performance in rabbits.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The US Food and Drug Administration (FDA) has made a great effort to encourage generic drug development and increase generic drug access for locally acting drug products during the Generic Drug User Fee Amendments (GDUFA) period I (1). This effort has continued under GDUFA II. Ophthalmic drug products are used to treat local ocular pathologies in humans such as glaucoma, inflammation, or infection. The development of ophthalmic generic drug products faces significant challenges as the pharmacologically active moiety reaches the site of action before they enter the systemic circulation and usually produces very low to undetectable levels in the systemic circulation. Hence, the traditional bioequivalence (BE) approaches with systemic drug concentrations for orally administered drugs are usually not applicable (2).
FDA may recommend in vivo and/or in vitro testing to establish the BE of specific ocular drug products. The selection of the method, in vivo or in vitro testing, depends upon the information collected by the study, the analytical methods available, and the nature of the drug product. In general, BE testing should use the most accurate, sensitive, and reproducible approach to demonstrate equivalence. Different approaches, ranging from a combination of in vitro characterization, aqueous humor pharmacokinetic (PK) studies, and/or pharmacodynamic (PD)/clinical endpoint studies have been recommended to demonstrate BE for ophthalmic products depending on the drug product’s active pharmaceutical ingredient (API), dosage form, indication, mechanism of action, and scientific understanding of drug release and disposition in the eye (3). However, PD endpoint and PK studies in aqueous humor impose a high-development cost, limiting the development of ophthalmic generic drugs. As per the Orange Book (4), about half of the currently marketed ophthalmic drugs have a generic competitor and most of these are ophthalmic solutions, warranting further research on this area to reduce developmental and regulatory barriers.
Ophthalmic suspensions are dispersions of finely divided, relatively insoluble API forming suspended particles in an aqueous vehicle. Particle size (PS) and viscosity were identified as key formulation elements influencing ocular biodistribution of the drug substance (5). The characterization of these formulation elements along other elements such as pH or specific gravity has been recommended in three FDA product-specific BE guidance for ophthalmic suspensions as an in vitro only approach (i.e., in vivo studies not necessary for BE establishment) (6,7,8). To support the regulatory decision for ophthalmic suspension, as well as for new drug product, modeling and simulation can be used to reinforce our understanding of the interplay between all critical aspects for ocular formulation.
Physiologically based pharmacokinetic models (PBPK) were first introduced in the 1970s to support drug development from preclinical to clinical trials as they can reduce the tremendous costs and attrition rate of drug development (9). There is great potential for ocular PBPK modeling to provide insight into drug partitioning in eye tissues that are not accessible and/or are challenging to sample in humans. To our knowledge, the first physiologically based model which could describe ocular concentration-time profiles in different tissues in rabbits was developed in the late 1970s for pilocarpine disposition in pre-cornea and aqueous humor (10,11). In 1986, Hui and Robinson published a specific model for pilocarpine and fluorometholone suspensions, incorporating drug dissolution, drug pre-cornea drainage and tear flow elimination in both solid and solution phases, and passive diffusion from corneal epithelium to the aqueous humor (12). These processes were also captured in other modeling efforts (13). Tear fluid pH variation in the pre-cornea compartment was included to account for the impact of tear pH on drug solubility over time (14). Models focusing in the intravitreal administration of small molecular weight compounds and macromolecules were recently developed (15,16,17). The impact of melanin binding on ocular drug delivery was modeled by Rimpelä et al. (18). Another study modeled the relationship between aqueous humor and plasma exposure (19). Walenga et al. recently reported their study of using a five compartments model describing the tear space for bioavailability calculations (20). However, each of these studies focused on drug distribution within only a limited number of ocular tissues and addressed only limited aspects of formulation behavior. Therefore, the published ocular physiologically based models to date may not be sufficient to address the impact of formulation characteristics, such as particle size (PS), PS distribution (PSD), and viscosity on ocular drug biodistribution and systemic exposure. Therefore, through grant 5U01FD005211, the Office of Generic Drugs in the US FDA collaborated with Simulation Plus, Inc. to advance the ocular PBPK and mechanistic absorption modeling by expanding the existing knowledge base for ocular drug absorption and disposition.
The purpose of this article is to demonstrate the application of ocular PBPK and mechanistic absorption modeling within GastroPlus™ in predicting the impact of ophthalmic formulation characteristics on drug disposition in rabbit eyes using dexamethasone (Dex) suspensions as the model drug.
Dex is a lipophilic molecule prescribed for inflammatory ocular conditions. Dex ocular suspension was first approved in 1962 (product name: MAXIDEX®) by the US FDA (21). It was then made available on the market in combination with tobramycin in two products: TOBRADEX® (22) and TOBRADEX ST® (23) with different formulation characteristics. The abundance of in-house FDA and literature data on Dex in rabbit eyes makes it the ideal test drug for our research.
This study includes (1) a PK study in rabbits to investigate the Dex distribution in ocular tissues and plasma following the unilateral administration of TOBRADEX ST® in a rabbit eye; (2) the verification of the developed ocular PBPK and mechanistic absorption model in rabbits using concentration-time profiles of Dex in different ocular tissues and plasma for multiple formulations with different product characteristics; and (3) the investigation of the impact of PS, PSD, and viscosity on drug disposition in rabbit eyes.
Methods
In Vivo Rabbit Study
The study was performed at the FDA White Oak Federal Research Center after receiving approval by the White Oak Federal Research Center Animal Care and Use Committee. Chockalingam et al. recently described the design of the study in detail (24). Briefly, the rabbits were randomly divided into seven groups with six rabbits in each group. All rabbits were treated with 30 μL of TOBRADEX ST® 0.05% in a single (right) eye. After instillation, no leakage of the dosing suspension from the eye was observed. Following the administration of TOBRADEX ST®, rabbits were euthanized with intravenous administration of pentobarbital-based euthanasia solution (0.22 mL/kg IV) in an ear vein immediately followed by the blood and eye tissue collection (cornea, conjunctiva, and aqueous humor) as terminal procedures at 0.5, 1, 2, 3, 4, 6, and 8 h. With respect to the sample collection, sample preparation, and sample analysis, the authors would like to refer the reader to the recently published manuscript by Chockalingam et al. (24,25).
Model Development
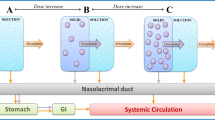
GastroPlus™ (version 9.6 Simulation Plus Inc., Lancaster, CA, USA) was used for computer simulation of Dex biodistribution in rabbit ocular tissues. Model structure integrates a mammalian two compartments model reflecting systmic disposition of Dex, an Ocular Compartmental Absorption & Transit (OCAT™) model describing ocular drug absorption and disposition (see Supplementary Materials for details), and an Advanced Compartmental Absorption & Transit (ACAT™) model to capture intestinal absorption of Dex after being ingested through nasolacrimal drainage (Fig. 1). Input parameters for the compound (Table 1) were obtained from literature or were fitted to in vivo data.

Model structure used to describe the pharmacokinetics of Dex following the unilateral administration of Dex suspensions. OCAT, Ocular Compartmental Absorption Transit; ACAT, Advanced Compartmental Absorption Transit. Please refer to the supplementary materials with respect to the OCAT model structure and equations
Published Dex plasma concentration-time profiles following the i.v. administration of 25 and 250 μg/kg to New Zealand rabbits (BW = 3 to 3.5 kg) (34) were used to define a compartmental PK structural model and parameters of the central and peripheral compartments using the PKPlus™ module within GastroPlus™. AIC criteria, data fitting, and parameter estimation precision were used to choose the best model.
The following assumptions were made for the OCAT model: (1) the administered dose is not lost from the eye by overflow (24); (2) the particles of Dex suspension do not trigger excessive lacrimation. A maximum particle diameter of 10 μm was used for the parameter sensitivity analysis because PS greater than this is considered to generate ocular irritation and discomfort (5). For model verification, Schoenwald et al.’s study used three dexamethasone suspensions with a mean PS ranging from 5.5 to 22 μm. The authors stated that Dex suspensions with a larger PS did not induce tearing in the study based on their observation (35).
PS (mean = 3.87 μm; SD = 1.46) and viscosity (ƞ = 72.9 cP) were utilized to describe the formulation characteristics of TOBRADEX ST® (30). The Lu, Frisela, and Johnson dissolution model was selected (36). Drainage rate (DR) was used to account for the viscosity difference between formulations based on the defined relationship between DR and viscosity (33). DR was set to 0.1 min−1 to account for the viscosity of 72.9 cP for TOBRADEX ST®.
Corneal epithelium and stroma permeabilities (6 E−6 cm/s) were selected based on the literature data (31,32). Conjunctiva, aqueous humor, and ICB permeabilities were optimized in GastroPlus™ by simultaneously fitting the observed ocular and plasma concentration-time profiles of Dex. Pre-cornea maximum volume was set to be 35 μL to account for the physiological tear volume (5 μL) (13) plus the administered volume of TOBRADEX ST® (30 μL). The drug in solid and solution phases in the pre-cornea is cleared through both DR and tear flow (Fig. 1).
During simulation, following the 30 μL of Dex eye drop administration, the volume of the pre-cornea compartment increased to 35 μL and gradually decreased back to the physiological volume (5 μL). The excess fluid is transported from the pre-cornea to the nasolacrimal duct. Tear dynamics can also clear solid and solution drug product away from the pre-cornea into the nasolacrimal duct. The model assumes first-order processes, given by the following equation (Fig. 1),
where DR and TF are drainage and tear flow rate constants, C is the pre-corneal drug concentration, Vt is the instantaneous pre-corneal volume, and Vphys is the baseline volume of pre-cornea (37).
Due to the lack of information on transporters which may be potentially involved in Dex transport in rabbit eye, the developed OCAT model assumes only passive distribution and does not include any active transport processes in the rabbit eye for Dex. It has been reported that there are no Dex metabolites detected in the rabbit aqueous and vitreous humor, retina, ciliary body, iris, choroid, cornea, lens, or sclera from rabbits and monkeys for up to 24 h post-dose (38). Hence, the developed OCAT model does not include the metabolic clearance for Dex in the eye.
Model Verification
The developed OCAT model was verified by describing the dose non-linear PK in ocular tissues and by characterizing the impact of viscosity and PS on in vivo drug ocular absorption and disposition. The following data sets were used for model verification (Supplementary Table 1):
-
1.
The dose non-linear PK in aqueous humor following the administration of 0.01, 0.05, and 0.1% of TOBRADEX ST® suspension as reported in NDA-50818 pharmacological/toxicology review and evaluation (39).
-
2.
Aqueous humor data following the administration of TOBRADEX® (Dex, 0.1%/tobramycin, 0.3%) with a viscosity of 1.67 cP and TOBRADEX ST® (Dex, 0.01%/tobramycin, 0.3%) with a viscosity of 72.9 cP were used to verify the model’s capacity to predict the impact of viscosity on ocular absorption and disposition. The data were also from the NDA-50818 pharmacological/toxicology review and evaluation (39).
-
3.
Schoenwald et al. investigated the effect of PS on ophthalmic bioavailability of Dex suspensions in rabbits (35). Cornea Dex concentration-time profiles for three suspensions with mean PS of 5.5, 11.5, and 22 μm (Dex, 0.1%, viscosity ~ 1 cP) were used for model verification.
It is noted that different DR values were used in the model to account for the difference in viscosity between formulations, for instance using 0.1 min−1 of DR to account for the viscosity of 72.9 cP for TOBRADEX ST®, while using 0.4 min−1 DR to account for the viscosity of 1.67 cP for TOBRADEX®, based on the relationship between viscosity and DR defined by Patton et al. (33).
Parameter Sensitivity Analysis
The impact of PS and viscosity on Dex Cmax, AUC0➔t, and Tmax in rabbit cornea, aqueous humor, and plasma were assessed using parameter sensitivity analysis (PSA) in GastroPlus™. The impact of PSD on Cmax and AUC0➔t in aqueous humor was also assessed using PSA.
Results
Dex Systemic and Ocular Pharmacokinetics in Rabbits
Dex plasma concentration data following i.v. administration in rabbits were best fitted into a two-compartment model (Supplementary Fig. 1). Across the investigated dosage range (25 to 250 μg/kg), Dex demonstrated a linear systemic PK characterized by the volume of distribution at steady state of 2.21 L/kg and the systemic clearance of 2.13 L/h.
The in-house Dex concentration-time profiles in cornea, conjunctiva, aqueous humor, and plasma following a single topical administration of 30 μL of TOBRADEX ST® 0.05% in a single rabbit eye are shown in Fig. 2 (24). Dex was rapidly absorbed, with the maximal concentration observed at around 30 mins in all the ocular tissues following the topical administration. As expected, the relative exposure was higher in the cornea following topical instillation of Dex. The Cmax in the cornea (11 μg/mL) was around 215-fold higher than that in the aqueous humor (0.051 μg/mL). The dexamethasone Cmax and AUC in aqueous humor obtained in our rabbit study are consistent with the observed values (within twofold) in NDA 50818 (39), considering the variation in drug administration, sample collection, analytical method accuracy, precision, etc. The significantly lower level of Dex in aqueous humor may be related to the fact that it is a lipophilic compound, with limited aqueous solubility. In the rabbit study conducted by the FDA, the Dex concentration as determined by Cmax is much higher in cornea (11.0 ± 4.2 μg/g) and Iris-ciliary body (0.441 ± 0.295 μg/g) compared to those in conjunctiva (0.896 ± 1.03 μg/g) and retina (0.0545 ± 0.0282 μg/g), respectively following the topical instillation of Dex (24), indicating that both corneal and conjunctival/scleral pathways contributed to the dexamethasone ocular absorption and corneal pathway is the primary route of intraocular absorption for Dex. The intraocular Dex levels were significantly higher than those in plasma, and the systemic elimination was relatively slower than the drug elimination in the cornea, conjunctiva, or aqueous humor. The developed OCAT-PBPK model simultaneously predicted the PK of Dex in the cornea, conjunctiva, aqueous humor, and plasma well, as shown in Fig. 2. The developed OCAT-PBPK model was thereafter verified by using in vivo rabbit data following the administration of Dex suspensions with different strengths, PS, or viscosity. Final model parameters values are provided in Table I.

In-house concentration-time profiles of Dex in cornea, conjunctiva, aqueous humor, and plasma following the unilateral administration of 30 μL of TOBRADEX ST® 0.05% in a rabbit eye (n = 6). Dots represent the observed data obtained in our animal study (24); lines represent the model prediction and error bars represent the standard deviation of the observed data
The FDA pharmacological/toxicology review and evaluation for TOBRADEX ST® (NDA 50818) shows a dose-dependent non-linear PK of Dex in aqueous humor was observed following the unilateral administration of three strengths of TOBRADEX ST®: 0.01, 0.05, and 0.1% (39) (Fig. 3a). About 11, 82.2, or 91.1% of the total amount of the drug is in the solid phase for TOBRADEX ST® 0.01, 0.05, or 0.1% strengths, respectively. Due to the constant nasolacrimal drainage and tears flow in the pre-cornea compartment, it was expected that a larger amount of Dex in the solid phase would be cleared through the nasolacrimal drainage and tear flow for the higher strength of TOBRADEX ST®. This mechanism accounted for the observed non-linear aqueous humor exposure in rabbits. The developed OCAT model incorporated both nasolacrimal drainage and tears flow clearance mechanisms for solid particles in the pre-cornea compartment and therefore, successfully predicted the pronounced dose non-linearity for Dex suspensions observed in aqueous humor (Fig. 3a).

a Non-linear pharmacokinetics of Dex in aqueous humor. The observed (red dot) or simulated (black triangle) Dex Cmax and AUC in aqueous humor for three doses of TOBRADEX ST® (0.01, 0.05 and 0.1%) were normalized with the observed or simulated Cmax and AUC of TOBRADEX ST® 0.01% (38); b left panel: time taken for the volume of pre-cornea returning back to the physiological volume (5 μL, black line) following the topical administration of a high viscosity (72.9 cP, solid line) and a low viscosity (1.67 cP, dash line) formulation. Right panel: observed and simulated aqueous humor Cmax and AUC0➔3 following the unilateral administration of 30 μL of TOBRADEX® 0.1% (D50 = 3 μm, ƞ = 1.67 cP) or TOBRADEX ST® 0.05% (D50 = 4 μm, ƞ = 72.9 cP) in one rabbit eye. The drainage rate was used in the OCAT model to account for the impact of viscosity (38); c the observed and simulated cornea concentration-time profiles following the unilateral administration in one rabbit eye of 30 μL of three Dex 0.1% formulations with different PS (D50 = 5.5, 11, 22 μm) (34)
Impact of Formulation Characteristics on Dex Ocular Absorption and Disposition
Viscosity
Differences in the viscosity of the instilled drop may impact the drug pre-corneal residence time and further affect the pre-corneal drug absorption and clearance. TOBRADEX® 0.1% and TOBRADEX ST® 0.05% have a viscosity of 1.67 and 72.9 cP, respectively. The higher viscosity can counteract the drug loss through drainage and tear turnover effect and further improve the ocular drug bioavailability despite initial strength difference.
Adjustment of the DR parameter in the OCAT-PBPK model to account for the viscosity change between formulations was sufficient to capture the impact of viscosity on ocular PK metrics (Fig. 3b). Model-based simulations showed the volume of pre-cornea returning to the physiological volume (5 μL) after 12 mins for low-viscosity formulations (DR = 0.4) compared to around 30 mins for the higher viscosity formulation (DR = 0.1) following the unilateral administration of 30 μL of TOBRADEX® 0.1% or TOBRADEX ST® 0.05% in a rabbit eye. The time taken for the volume of pre-cornea to return to the physiological volume may be a critical factor for ocular API absorption and disposition.
Particle Size
PS affects the dissolution rate of the particles residing in the conjunctival sac and further influences ocular bioavailability. Schoenwald et al. conducted a study in rabbits to investigate the impact of PS on the ocular bioavailability of a 0.1% Dex suspension (35). Their results showed that as the mean particle size increased from 5.75 to 11.5 and to 22 μm, the rate and extent of the drug penetration into the cornea decreased. The developed OCAT Dex model accurately captures the PS impact on in vivo Dex ocular PK performance and the predicted Dex cornea exposure increases as PS decreases (Fig. 3c). Schoenwald et al. did not provide information on the viscosities of the three formulations but did use similar formulations that excluded a viscosity-modifying agent. A DR value of 1 was assigned in the OCAT model for all three formulations to account for the impact of viscosity, which assumes that the viscosity of the three formulations would be low and similar.
Parameter Sensitivity Analysis
Viscosity and Particle Size
Figure 4 shows that the Cmax, AUC0➔t, and Tmax of Dex in the cornea, aqueous humor, and plasma as a function of PS and viscosity. The viscosities of Dex formulation in a range of 1 to 100 cP were used for sensitivity analysis, as the range includes the viscosities of TOBRADEX® 0.1% and TOBRADEX ST® 0.05%. A maximum particle diameter of 10 μm was used for the simulation because PS greater than this can give rise to ocular irritation and discomfort (5).

PSA to study the impact of mean PS (0.5 < D50 < 10 μm) and viscosity (1 < Vis < 100 cP) on Dex Cmax and AUC0➔t T/R ratios and Tmax in cornea, aqueous humor, and plasma following the unilateral administration of 30 μL ophthalmic suspension 0.05% in a rabbit eye. Gray circles represent the reference product, TOBRADEX ST®. Vis stands for viscosity
Dex ocular exposure appeared to be very sensitive to differences in formulation viscosity. A 2.5-fold decrease in Cmax and AUC in the cornea and aqueous humor was observed when viscosity decreased from 72.9 to 1.67 cP, whereas the Cmax and AUC of Dex in the cornea and aqueous humor only slightly increased when PS was reduced from 10 to 1 μm. The changes in Cmax and AUC of Dex in the plasma were not sensitive to changes in both PS and viscosity. The Tmax in cornea and aqueous humor was prolonged with the increase in viscosity. The latter may counteract the drug loss through drainage and tear turnover effect, thus prolonging the drug pre-corneal residence time. The effect of viscosity on ocular tissues Tmax reached a plateau when viscosity values were greater than 40 cP, indicating that the viscosity impact on the pre-corneal residence time reaches the maximum physiological system capacity at that point. When viscosity was lower than 40 cP, a slightly longer Tmax in cornea was predicted with the increase in PS. However, the Tmax in aqueous humor was not altered by changing the PS. The suspended particles eliminated from tear film through nasal drainage and tear turnover effect are transported to the gastrointestinal tract and then absorbed to the systemic circulation. Therefore, the plasma Tmax was significantly affected by the PS, with the larger PS resulting in a longer Tmax.
Particle Size Distribution
PS and PSD of ophthalmic suspensions are critical formulation properties that are affected by the manufacturing process. Although processing can be used to tailor the final PS and PSD, in general, the PSD of micronized ophthalmic suspension products can be described as a log-skewed distribution. As previously mentioned, the dissolution rate of the particles residing in the conjunctival sac and thus ocular bioavailability. Therefore, a parameter sensitivity analysis was conducted to investigate the impact of PSD on Dex in vivo ocular absorption and distribution.
Six hypothetical test formulations with different PSD were designed for the sensitivity analysis in silico (Table II). The test formulations have similar mean particle diameter, similar D10, but have different D90 values compared to the TOBRADEX ST® 0.05%. The simulation result showed that about a twofold increase in the D90 in the test formulations gives rise to a marginal increase in the Dex aqueous humor Cmax and AUC T/R ratio of 1.00 to 1.06. These findings suggest that the different D90 values within an acceptable range for an ophthalmic formation may not be the critical factor influencing the in vivo Dex ocular absorption.
Discussion
BE evaluation for ophthalmic generic products depends on the understanding of ocular absorption mechanism. Physicochemical properties of the ophthalmic formulation impact the ocular absorption and further influence the rate and extent to which a drug reaches the site of action. To our knowledge, this is the first article to employ a fully verified OCAT-PBPK model investigating the impact of physiochemical properties of the ophthalmic suspension on in vivo ocular drug absorption and disposition in rabbits. This model provides a better understanding of the ocular absorption mechanism and how the physiochemical properties of the ophthalmic formulation impact the ocular absorption and further influence the rate and extent to which a drug reaches the ocular site of action. In particular, the site of action of Dex is the anterior segment of the eye globe (21,22,23). Such understanding can aid in the development and regulatory assessment of ophthalmic drug suspensions.
Ophthalmic suspensions are dispersions of finely divided, relatively insoluble drug substances in an aqueous vehicle containing suitable dispersing, wetting, and preservatives agents. In this study, we focused on how PS, PSD, and viscosity, as critical formulation attributes, impact drug release, clearance, and ocular absorption. The OCAT Dex model developed within GastroPlus™ for this study successfully predicted the impact of PS and viscosity on in vivo Dex ocular PK performance after incorporation of clearance through lacrimal drainage and tear turnover in the pre-corneal compartment on both drug phases: solid and solution. Our study suggests that an increase in PSD caused by increasing the proportion of the largest suspended particles have no significant impact on ocular exposure. PS is an important factor determining the ocular bioavailability: the simulated Cmax and AUC in cornea gradually decreased with the increased PS. As PS increased from 5.5 to 11 μm and from 11 to 22 μm, Cmax decreased by 21% and 26%, respectively, and AUC decreased by 19% and 25%, respectively. The simulation results also showed that the larger the PS, the greater the amount of drug lost from the pre-corneal compartment (data not shown). Therefore, as the PS increases, both the rate and extent of drug absorbed into the eye tissues decrease. The most critical factor influencing the ocular drug bioavailability is particle clearance from the pre-corneal compartment. Indeed, the time to achieve complete dissolution of the suspended materials may be longer than the residence time of the particle in the tears. A smaller particle diameter, inducing a faster dissolution rate would then benefit the API absorption, but the reduction of the particle elimination rate from the ocular surface has a larger impact on ocular bioavailability.
The same Tmax in the cornea for Dex suspensions with PS of 5, 11, or 22 μm were predicted by using the developed OCAT model in this study, assuming that the viscosity was not impacted by altering the mean PS. This result is consistent with the previously published study in rabbits by Schoenwald et al. showing that PS does not impact the cornea Tmax, which occurred at around 15 mins for Dex suspensions with PS of 5, 11, or 22 μm (35). Hui et al. also reported that the Tmax in aqueous humor for fluorometholone suspensions with different PS were similar for all formulation (12). This is not consistent with what we usually expect about the impact of PS on Tmax for an oral dosage form, where a larger PS would generally lead to a longer Tmax due to slower dissolution rate. In the pre-corneal compartment, the loss of the drug particle is controlled by the magnitudes of drainage and tear turnover. The rate of dissolution of drug particle and the rate of API absorption through the cornea must be faster than the rate of loss of drug product from the eye surface in order to have an ocular accumulation of drug. Hence, once the dissolution rate decreases to the rate that the particles are removed from the conjunctival sac, the particles in the cul-de-sac would not be available for absorption.
Published rabbit studies (39) and our simulation results all demonstrated only a moderate increase (less than threefold) in aqueous humor concentration with a tenfold increase in Dex suspension dosage strength. This maybe because a substantial amount of drug (dissolved and undissolved) was drained away before being absorbed into the cornea. The larger amount of undissolved drug present in the pre-cornea compartment leads to a larger amount of undissolved drug cleared through the drainage and tear turnover effect. Hence, the ocular suspension drug concentration does not reflect the drug available to be absorbed. In contrast, the drug concentration in ocular solutions reflects the drug concentration in the solution that is immediately available for corneal absorption. For example, a linear increase in aqueous humor concentration was observed with the increase in pilocarpine solution dosage strength (from 5 × 10−4 to 10−2 M) (40). Although the proportional increase in aqueous humor exposure cannot be achieved through increasing the dosing concertation of ophthalmic suspensions, the undesired systemic exposure appeared to be greatly increased and potentially leading to systemic safety concerns (41).
To prolong the pre-corneal residence time, attempts have been made to increase the viscosity of Dex suspension. Indeed, TOBRADEX ST® (tobramycin/dexamethasone ophthalmic suspension 0.3%/0.05%, 72.9 cP) has a higher viscosity and lower Dex concentration compared to TOBRADEX® (tobramycin/dexamethasone ophthalmic suspension 0.3%/0.1%, 1.67 cP), but are pharmacokinetically relatively similar. The higher viscosity can counteract the drug loss through drainage and tear turnover effect and further improve the ocular drug bioavailability. Based on simulations conducted using the developed ocular PBPK model, when the viscosity of Dex ophthalmic suspension is greater than 40 cP, the impact of viscosity on the pre-corneal residence time reaches the maximum physiological system capacity and thus further increase in viscosity would no longer improve the ocular drug bioavailability. When the viscosity is lower than 40 cP, then the ocular drug exposure is reduced rapidly with the decrease in viscosity. The parameter sensitivity analysis demonstrated that plasma PK metrics are not sensitive to the change in PS and viscosity of the formulation compared to the aqueous humor PK metrics. As such, plasma PK does not appear to be a reliable surrogate reflecting the change of the rate and extent of Dex absorption at the ocular site of action.
The limitations of the current ocular PBPK modeling approach include the inability to accurately incorporate certain physiological/biological processes and capture their impact on ocular drug disposition. For instance, the impact of the blinking rate on drug retention dynamics at the surface of the eye, which differs among species, is not captured into the platform used here. OCAT-PBPK models are not capable yet to perform a pure prediction for a new API incorporated in a new formulation. This study shows how the platform can be used to predict the impact of key formulation attributes on ocular bioavailability once the OCAT is optimized and verified using preclinical data. In addition, it would be more of a challenge to model drug disposition in the posterior ocular tissues (e.g., retina, choroid, vitreous humor) over anterior ocular tissues (e.g., cornea and conjunctiva) due to the lack of in vitro information regarding permeability of these tissues. Finally, the modeling platform does not provide the capability of describing the impact of disease on ocular drug disposition.
In conclusion, we have successfully developed and verified an OCAT model for Dex and have investigated the impact of drug product strength, PS, PSD, and viscosity on in vivo ocular exposure for ophthalmic suspensions in rabbits. This tool may support drug development and provide a better understanding of the impact of formulation modifications on the in vivo performance of ophthalmic drug products. Expanding the application of the current developed OCAT model to additional ophthalmic dosage forms, such as ophthalmic ointments, and developing the extrapolation from rabbit to human model have been initiated as part of FDA ongoing research.
References
Center for Drug Evaluation and Research. Generic drug user fee amendments [Internet]. [cited 2018 Dec 14]. Available from: https://www.fda.gov/ForIndustry/UserFees/GenericDrugUserFees/default.htm. Accessed 30 Apr 2019.
US. FDA. Bioavailability and bioequivalence studies for orally administered drug products—general considerations [Internet]. 2003. Available from: https://www.fda.gov/media/87219/download. Accessed 30 Apr 2019.
Choi SH, Lionberger RA. Clinical, pharmacokinetic, and in vitro studies to support bioequivalence of ophthalmic drug products. AAPS J. 2016;18(4):1032–8. https://doi.org/10.1208/s12248-016-9932-z.
Orange book: approved drug products with therapeutic equivalence evaluations [Internet]. [cited 2018 Dec 14]. Available from: https://www.accessdata.fda.gov/scripts/cder/ob/. Accessed 30 Apr 2019.
Ali Y, Lehmussaari K. Industrial perspective in ocular drug delivery. Adv Drug Deliv Rev. 2006 Nov 15;58(11):1258–68.
US. FDA. Draft Guidance on Dexamethasone; Tobramycin [Internet]. 2016. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/psg/Dexamethasone Tobramycin_ophthalmic suspension NDA 50818 RV Feb 2019.pdf.. Accessed 30 Apr 2019.
US. FDA. Draft guidance on Nepafenac [Internet]. 2016. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/psg/Nepafenac_ophthalmic suspension 0.1_RLD 0021862_RV12-16.pdf. Accessed 30 Apr 2019.
US. FDA. Draft guidance on Loteprednol Etabonate [Internet]. 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/psg/Loteprednol Etabonate_draft_Ophthalmic drops susp_RLD 020583_RCO2-18.pdf. Accessed 30 Apr 2019.
Sager JE, Yu J, Ragueneau-Majlessi I, Isoherranen N. Physiologically based pharmacokinetic (PBPK) modeling and simulation approaches: a systematic Review of published models, applications, and model verification. Drug Metab Dispos. 2015;43(11):1823–37.
Sieg JW, Robinson JR. Mechanistic studies on transcorneal permeation of pilocarpine. J Pharm Sci. 1976;65(12):1816–22.
Himmelstein KJ, Guvenir I, Patton TF. Preliminary pharmacokinetic model of pilocarpine uptake and distribution in the eye. J Pharm Sci. 1978;67(5):603–6.
Hui HW, Robinson JR. Effect of particle dissolution rate on ocular drug bioavailability. J Pharm Sci. 1986;75(3):280–7.
Worakul N, Robinson JR. Ocular pharmacokinetics/pharmacodynamics. Eur J Pharm Biopharm. 1997;44(1):71–83.
Deng F, Ranta V-P, Kidron H, Urtti A. General pharmacokinetic model for topically administered ocular drug dosage forms. Pharm Res. 2016;33(11):2680–90. https://doi.org/10.1007/s11095-016-1993-2.
del Amo EM, Vellonen K-S, Kidron H, Urtti A. Intravitreal clearance and volume of distribution of compounds in rabbits: in silico prediction and pharmacokinetic simulations for drug development. Eur J Pharm Biopharm. 2015;95(Pt B):215–26.
Lamminsalo M, Taskinen E, Karvinen T, Subrizi A, Murtomäki L, Urtti A, et al. Extended pharmacokinetic model of the rabbit eye for intravitreal and intracameral injections of macromolecules: quantitative analysis of anterior and posterior elimination pathways. Pharm Res. 2018;35(8):153.
Hutton-Smith LA, Gaffney EA, Byrne HM, Maini PK, Gadkar K, Mazer NA. Ocular pharmacokinetics of therapeutic antibodies given by intravitreal injection: estimation of retinal permeabilities using a 3-compartment semi-mechanistic model. Mol Pharm. 2017;14(8):2690–6. https://doi.org/10.1021/acs.molpharmaceut.7b00164.
Rimpelä A-K, Reinisalo M, Hellinen L, Grazhdankin E, Kidron H, Urtti A, et al. Implications of melanin binding in ocular drug delivery. Adv Drug Deliv Rev. 2018;126:23–43.
Grass GM, Lee VH. A model to predict aqueous humor and plasma pharmacokinetics of ocularly applied drugs. Invest Ophthalmol Vis Sci. 1993;34(7):2251–9.
Walenga RL, Babiskin AH, Zhang X, Absar M, Zhao L, Lionberger RA. Impact of vehicle physicochemical properties on modeling-based predictions of cyclosporine ophthalmic emulsion bioavailability and tear film breakup time. J Pharm Sci. 2019;108(1):620–9.
US. FDA. MAXIDEX®- dexamethasone ophthalmic suspension label [Internet]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/013422s045lbl.pdf. Accessed 30 Apr 2019.
US. FDA. TOBRADEX® (tobramycin and dexamethasone ophthalmic suspension) label [Internet]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2003/50592slr032_tobradex_lbl.pdf. Accessed 30 Apr 2019.
US. FDA. TOBRADEX® ST (tobramycin / dexamethasone ophthalmic suspension) label [Internet]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/050818lbl.pdf. Accessed 30 Apr 2019.
Chockalingam A, Xu L, Stewart S, Le Merdy M, Tsakalozou E, Fan J, et al. Protocol for evaluation of topical ophthalmic drug products in different compartments of fresh eye tissues in a rabbit model. J Pharmacol Toxicol Methods [Internet] 2018. [cited 2018 Dec 17]; Available from: http://www.sciencedirect.com/science/article/pii/S105687191830697X.
Matta MK, Narayanasamy S, Thomas CD, Xu L, Stewart S, Chockalingam A, et al. A sensitive UPLC-APCI-MS/MS method for the determination of dexamethasone and its application in an ocular tissue distribution study in rabbits following topical administration. Anal Methods. 2018 May 24;10(20):2307–16.
Dexamethasone [Internet]. [cited 2018 Dec 14]. Available from: https://www.drugbank.ca/drugs/DB01234. Accessed 30 Apr 2019.
Obach RS. Prediction of human clearance of twenty-nine drugs from hepatic microsomal intrinsic clearance data: an examination of in vitro half-life approach and nonspecific binding to microsomes. Drug Metab Dispos Biol Fate Chem. 1999;27(11):1350–9.
Yamashita S, Furubayashi T, Kataoka M, Sakane T, Sezaki H, Tokuda H. Optimized conditions for prediction of intestinal drug permeability using Caco-2 cells. Eur J Pharm Sci. 2000;10(3):195–204.
Barry BW, El Eini DI. Solubilization of hydrocortisone, dexamethasone, testosterone and progesterone by long-chain polyoxyethylene surfactants. J Pharm Pharmacol. 1976;28(3):210–8.
Choi Stephanie, Wu Yang, Kozak Darby, Zheng J. Physicochemical characterization of Tobradex and Tobradex ST under physiological conditions. Baltimore; 2017.
Prausnitz MR, Noonan JS. Permeability of cornea, sclera, and conjunctiva: a literature analysis for drug delivery to the eye. J Pharm Sci. 1998;87(12):1479–88.
Hahne M, Zorn-Kruppa M, Guzman G, Brandner JM, Haltner-Ukomado E, Wätzig H, et al. Prevalidation of a human cornea construct as an alternative to animal corneas for in vitro drug absorption studies. J Pharm Sci. 2012;101(8):2976–88. https://doi.org/10.1002/jps.23190.
Patton TF, Robinson JR. Ocular evaluation of polyvinyl alcohol vehicle in rabbits. J Pharm Sci. 1975;64(8):1312–6.
Hosseini K, Matsushima D, Johnson J, Widera G, Nyam K, Kim L, et al. Pharmacokinetic study of dexamethasone disodium phosphate using intravitreal, subconjunctival, and intravenous delivery routes in rabbits. J Ocul Pharmacol Ther. 2008;24(3):301–8.
Schoenwald RD, Stewart P. Effect of particle size on ophthalmic bioavailability of dexamethasone suspensions in rabbits. J Pharm Sci. 1980;69(4):391–4.
Lu AT, Frisella ME, Johnson KC. Dissolution modeling: factors affecting the dissolution rates of polydisperse powders. Pharm Res. 1993;10(9):1308–14.
SimulationPlus. GastroPlus 9.6 manual. 2018. https://doi.org/10.17226/25305.
TGA. Australian Public Assessment report for dexamethasone [Internet]. 2016. Available from: https://www.tga.gov.au/sites/default/files/auspar-dexamethasone-161025.docx. Accessed 30 Apr 2019.
US. FDA. Pharmacology Review(s) NDA 50-818 [Internet]. 2009. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/050818s000pharmr.pdf. Accessed 30 Apr 2019.
Makoid MC, Robinson JR. Pharmacokinetics of topically applied pilocarpine in the albino rabbit eye. J Pharm Sci. 1979;68(4):435–43.
Farkouh A, Frigo P, Czejka M. Systemic side effects of eye drops: a pharmacokinetic perspective. Clin Ophthalmol. 2016;10:2433–41.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclaimer
This article reflects the views of the authors and should not be construed to represent FDA’s views or policies.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Le Merdy, M., Fan, J., Bolger, M.B. et al. Application of Mechanistic Ocular Absorption Modeling and Simulation to Understand the Impact of Formulation Properties on Ophthalmic Bioavailability in Rabbits: a Case Study Using Dexamethasone Suspension. AAPS J 21, 65 (2019). https://doi.org/10.1208/s12248-019-0334-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12248-019-0334-x