
Abstract
Background
Step width is a spatial variable in the frontal plane, defined as the mediolateral distance between the heel (forefoot during sprinting) of bilateral feet at initial contact. Variations in step width may impact the lower limb biomechanics. This systematic review aimed to synthesize the published findings to determine the influence of acute changes in step width on locomotion biomechanics and provide implications for injury prevention and enhanced sports performance.
Methods
Literature was identified, selected, and appraised in accordance with the methods of a systematic review. Four electronic databases (Web of Science, MEDLINE via PubMed, Scopus, and ScienceDirect) were searched up until May 2023 with the development of inclusion criteria based on the PICO model. Study quality was assessed using the Downs and Black checklist and the measured parameters were summarized.
Results
Twenty-three articles and 399 participants were included in the systematic review. The average quality score of the 23 studies included was 9.39 (out of 14). Step width changed the kinematics and kinetics in the sagittal, frontal, and transverse planes of the lower limb, such as peak rearfoot eversion angle and moment, peak hip adduction angle and moment, knee flexion moment, peak knee internal rotation angle, as well as knee external rotation moment. Alteration of step width has the potential to change the stability and posture during locomotion, and evidence exists for the immediate biomechanical effects of variations in step width to alter proximal kinematics and cues to impact loading variables.
Conclusion
Short-term changes in step width during walking, running, and sprinting influenced multiple lower extremity biomechanics. Narrower step width may result in poor balance and higher impact loading on the lower extremities during walking and running and may limit an athlete’s sprint performance. Increasing step width may be beneficial for injury rehabilitation, i.e., for patients with patellofemoral pain syndrome, iliotibial band syndrome or tibial bone stress injury. Wider steps increase the supporting base and typically enhance balance control, which in turn could reduce the risks of falling during daily activities. Altering the step width is thus proposed as a simple and non-invasive treatment method in clinical practice.
Key Points
Short-term changes in step width during gait could influence multiple lower extremity biomechanics.
Increasing step width may be beneficial for specific injury rehabilitation.
Wider steps increase the supporting base and typically enhance balance control to reduce the falling risks.
AbstractSection Graphical abstract
Similar content being viewed by others


Background
Human locomotion depends heavily on spatial and temporal factors. Modifying spatial or temporal factors during walking and running can change gait patterns and the associated biomechanics of the lower extremities [1]. Therefore, gait modifications via changes in spatiotemporal parameters could affect several biomechanical factors associated with running-related injuries [2,3,4]. As reported, optimizing spatiotemporal variables may impact energy expenditure and exercise performance [5, 6], which would produce an optimal economy during walking and running activities [7]. In addition, the change of spatiotemporal variables during walking will also be a challenge to the gait balance at all ages [8, 9]. Among spatiotemporal variables like step frequency (cadence), step length, step width, and contact time, step width is often under-investigated. However, we contend that it may influence the mechanics of lower extremity joints [10].
Step width is a spatial variable in the frontal plane, defined as the mediolateral distance between the heels of bilateral feet at initial contact [11]. Variations in step width and the contributing factors are complex and diverse. As per the findings of previous research, factors such as obesity, sex, age, foot shape and posture, footwear and external conditions have been found to affect the step width [12,13,14,15,16,17,18,19,20,21,22,23,24]. Footwear, ground conditions and other external factors would also affect step width [25,26,27,28,29]. For example, obesity could lead to a wider step in all ages [17, 18, 24]. In the context of aging, there is a tendency for step width to increase in the elderly [15, 16]. Functional differences in gait are inherent to sex differences, and females have exhibited a narrower step width compared to males [12, 14, 21]. Pregnancy can also be associated with different step widths in females [13, 19, 20]. Furthermore, Shin et al. [23] found that step width was significantly lower in flatfoot patients compared to symptom-free feet. Previous research reported that shod running widens the step width compared to barefoot running [26, 29]. Additionally, wearing footwear with varying soles and instep flexibility may result in biomechanical variations [28, 29].
Variations in step width may impact the biomechanics in all three planes, and in turn, the function of its constituent components [30]. In the frontal plane, previous research of running reported that a change in step width can alter the rearfoot kinematics [31]. Rearfoot eversion angle peaks and excursion were increased in normal and cross-over running but not during wider step conditions [31]. The kinematics and joint kinetics in the proximal joints (i.e. the knee and hip) are affected by the substantial alterations in step width [11, 32,33,34,35,36]. As the step width narrows in gait, the peak knee abduction moment and impulse decrease [11]. In contrast, the peak knee adduction moment and angular impulse increase [32], along with hip adduction and range of motion (ROM) in hip adduction [34, 35, 37]. The hip adduction moment also increases [36]. In addition to the frontal plane, recent studies have indicated that the step width also influences the biomechanics in the sagittal and transverse planes [33, 37]. Therefore, in our endeavour to better manage overuse injuries, step width is a crucial spatial parameter that warrants exploration in the monitoring and modification of human gait.
The above findings suggest that step width variations and alterations show biomechanical influences. To the best of our knowledge, a systematic review of the actively changing step width in walking, running, and sprinting biomechanics is lacking. Hence, this systematic review aimed to synthesize the published findings to determine the influence of acute changes in step width on locomotion biomechanics, provide implications for injury prevention, and enhance sports performance.
Methods
The protocol of this systematic review was conducted in accordance with the PRISMA 2020 Guidelines Reporting project for the checklist employed in the current study [38], and was registered at the International Prospective Register of Systematic Reviews (CRD42023445165).
Search Strategy
We conducted a literature search of the following databases: Web of Science, MEDLINE via PubMed, Scopus, and ScienceDirect. On May 1st of 2023, two researchers (Y.W. and H.J.) independently performed the screening of titles, abstracts, and keywords in these online electronic databases to identify potential studies and searched again on February 1st of 2024, to identify potential new articles between the two search dates. Keywords (MeSH or non-MeSH terms) according to three groups were used in combination with the Boolean indicator “AND” and “OR”. Search terms included ((Step-width OR Step width) AND (run OR walk OR sprint) AND (gait OR biomechanic OR kinetic OR kinematic)). An English language limit was applied. All screened literature was imported into the reference management software (Endnote® version X7, Thomson Reuters, Philadelphia, PA, USA), where duplicate references were removed.
Eligibility Criteria
The PICO (Patients, Intervention, Comparator, and Outcome) model was used to determine the inclusion and exclusion criteria for the literature in the current systematic review.
Inclusion Criteria
We included full-text original research of which the journal paper was peer-reviewed and published in English. This systematic review included the research design in previous studies with the repeated measures experiments, randomized controlled trial (RCT), pre- and post- test design, and pre- and post- test control group.
(1) The population included comprised healthy or pathological adults over the age of 18, without constraints on sex or ethnicity. (2) The study’s intervention targeted substantial differences in step width during walking, running and sprinting. (3) The study had to report an acute comparison of different step widths in level running or walking. (4) The reported outcomes included various biomechanical measures with different step widths, such as spatiotemporal parameters, kinematics, kinetics, electromyography, plantar pressure, etc.
Exclusion Criteria
Abstracts, case studies, editorials, reviews, and meta-analyses were excluded. Studies with individuals under the age of 18 were excluded. Studies carried out on stairs or sloping surfaces, without step width intervention and biomechanical outcomes were excluded.
Data Extraction
After this search process, two reviewers (Y.W. and Q.M.) independently extracted the study characteristics, including the author, date, country, population (sex and age), intervention, motion type (gait pattern), footwear condition, comparisons, outcome (i.e., spatiotemporal parameters, kinematics, kinetics, electromyography, plantar pressure, etc.), results and conclusion. Owing to the lack of comparable data and high-quality studies identified, the meta-analysis was not performed in this systematic review. As a result, the resulting data will be presented descriptively in the tables.
Quality Assessment
The quality of the associated studies was determined using the modified Downs and Black checklist with 13 of the 27 items from the Downs and Black quality assessment checklist being used following our previous review on walking and running [39,40,41]. The 13 items in the Quality Assessment Tool (Table 1) might have received the following answers from the reviewers: “Yes,” “No,” or “Cannot Determine.” Any question to which a reviewer responded “Yes” received a score of “1”. Any other response was given a “0”. Thus, the maximum quality score was 14. Zandbergen et al. [42] and Hooper et al. [43] have provided multiple quality labels based on the quality score. A study was considered to be of “Poor” quality if it received a score between 0 and 7, “Fair” quality if receiving a score between 8 and 9, “Good” quality if receiving a score between 10 and 12, and “Excellent” quality if receiving a score of 13 or 14. In this case, the tool is appropriate because it is suitable for all types of quantitative research designs [44]. Each study’s quality was evaluated separately by two researchers (Y.W. and H.J.), and the quality assessment disagreements were addressed until a consensus was reached. If consensus was not reached, a third reviewer (Q.M.) made the final decision.
Results
Search Results
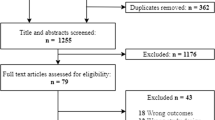
The primary search resulted in 2981 articles from the electronic databases. After deleting 1121 duplicate articles based on the title and abstract, 1860 articles were examined and 1821 were removed. The full texts of the remaining 39 articles were examined. Twenty-three articles met the inclusion criteria and were ultimately included in the systematic review. The flow diagram of this systematic review is shown in Fig. 1.

Flow diagram of the systematic review study selection process
Quality Assessment Results
The average quality score of the 23 articles included was 9.39 out of 14. Among these articles, 14 studies were ranked as “Good” with scores ranging from 10 to 12 [9, 11, 30, 33, 35,36,37, 45,46,47,48,49,50,51,52,53]. Six studies were ranked as “Fair” with scores of 8 or 9 [8, 31, 34, 46,47,48,49,50,51,52,53,54,55,56]. and 3 studies were considered as “Poor” with scores ranging from 0 to 7 [32, 54, 55]. None of the included studies reached the level of “Excellent”. Table 1 lists all the scores from the quality evaluation.
Study Characteristics
The current review classified 23 studies into 3 categories according to the motion type of research, specifically the walking activity (Table 2), running activity (Table 3) and sprinting activity (Table 4). Each table provided a full overview of the characteristics of the research subjects included in this systematic review. The 23 studies included 399 participants. There was a total of 213 males and 148 females included in 22 studies, and only one study did not report the sex [33]. The mean age of the adult population was 27.32 (± 10.53) years. Two articles only included males [45, 47], and in one of them Nagano et al. [47] included young as well as old participants.
All 23 articles included in this systematic review compared the biomechanical differences from altered step widths in walking, running or sprinting activities. Of the 23 studies, 17 were conducted during walking, 6 were conducted during running and 2 were conducted during sprinting. Fourteen of the 23 studies compared a narrow step width, the preferred (habitual) step width and a wide step width. Four of the 23 studies compared the preferred step width to a greater width. Finally, five of the 23 studies compared the preferred step width to a narrower width.
Biomechanical Effects of Altering Step Width
All 23 studies included in this systematic review compared the biomechanical differences from altered step widths.
Spatiotemporal Changes Following a Change in Step Width
Three of the included papers assessed spatiotemporal parameters after altering step width [46, 47, 56]. Walking with wider and narrower step widths significantly increased step width variability compared to control condition [46, 47, 56]. Both narrow and wide walk steps were associated with increased mean stride time and decrease in stride time variability [46]. In addition, narrow steps increased average step length and step length variability whereas wide steps decreased average step length and conversely increased the step length variability [46].
Kinematic Changes Following a Change in Step Width
Thirteen of the included articles assessed kinematic parameters when altering step width. A change in step width led to changes of trunk kinematics [53], and also to change in lower extremity joint kinematics [11, 31, 34, 35, 37].
During running, narrow step width increased the peak rearfoot eversion [31], but wider step width condition reduced peak rearfoot eversion angles compared with the narrow and preferred conditions [11, 31]. Knee internal rotation varied depending on step width and was higher in the narrow steps than in the normal condition; however, no statistically significant changes were discovered between the preferred and wide conditions [11, 37]. In the hip joint, a wide step width reduced average hip adduction angle [11, 37].
During walking, the kinematics of the hip joint showed the same changes as running when changing the step width but displayed a smaller range of motion of hip adduction than either narrow or normal step width conditions in locomotion biomechanics [34, 35].
Center of mass (COM) position was also associated with changes in step width during walking. Variability of COM and variability of COM velocity increased in decreased step width conditions to narrow-base condition [9, 47, 55, 56]. Arvin et al. also discovered that increasing the step width resulted in more COM variability than the preferred step width [9]. Mediolateral (ML)-COM kinematics deviation scaled with step width, less ML-COM displacement in the narrow condition [8, 45, 51, 53], as well as narrow step width condition, presented with lower ML-COM velocity [9]. Additionally, the margin of stability (MOS) from anterior–posterior (AP-MOS) and mediolateral (ML-MOS) directions were also affected by the step width conditions [8, 9, 52]. Walking with narrow steps decreased ML-MOS significantly, while walking with wide steps increased AP-MOS and decreased ML-MOS significantly [8, 52]. Further, Young et al. (2012) found that wide step width was linked to increased AP-MOS and ML-MOS variability [8]. However, Arvin et al. failed to observe a difference in the ML-MOS’s variability with different step widths [9]. In addition, during sprinting, COM can also be affected by step width; narrower steps reduce COM propulsion and particularly support [54].
Kinetic Changes Following a Change in Step Width
Ten of the included papers assessed kinetics parameters after altering step width. Previous studies found that step width could alter the kinetics of the hip joint, knee joint, ankle, subtalar joint (STJ) and rearfoot [11, 30, 32, 33, 36].
In running, when the step width changed from wide to narrow, the peak rearfoot inversion moment increased [11]. The narrow step-width condition had a larger peak rearfoot inversion moment than the wide step width condition, while the preferred step width had a larger peak rearfoot inversion moment than the wide steps [11]. Peak knee abduction moment and impulse were smaller in the preferred and wider step conditions compared to the narrow step condition during running, and were also smaller in the wider step condition compared to the preferred step width [11].
In walking, step width had an impact on the knee kinetics in all three planes [11, 30, 32, 33, 35, 36]. In the sagittal plane, peak knee flexion moments increased in wider step width with toe-in compared to normal gait [33], and knee extension moment was larger with increased step width [35]. In the frontal plane, wider step resulted in decreased peak knee adduction moment and knee adduction moment angular impulse [32, 33, 36]. In the transversal plane, peak knee external rotation moments were greater in larger step width with toe-in compared to normal gait [33]. In the hip joint, increased step width during walking reduced peak hip adduction moment [36]. Furthermore, the tibia was mainly loaded when the step width was narrower, and iliotibial band strain and strain rate showed a linear increasing trend as the step width narrowed [37, 48].
Peak STJ moments and propulsion were lowered when walking at larger step widths than preferred during initial contact, but knee and hip energy absorption increased at the initial contact [30].
As step width increases during walking, the medial ground reaction force (GRF) and eccentricity of the net GRF were increased [35, 52]. During sprinting, the vertical and forward GRF peaks were higher in the natural control condition compared to the narrow-width conditions [54].
EMG Changes Following a Change in Step Width
Five of the included articles assessed muscle activation via EMG following an alteration in step width. Lower extremity muscle activity was susceptible to step width alterations. More specifically, the activities of gluteus medius and gluteus minimus increased as step width increased in walking [49, 50]. On the contrary, peak longissimus activation and bilateral longissimus co-activation both decreased at wider step widths [53]. Furthermore, the peak activation duration in narrow walking conditions associated with the dominant leg stance was delayed compared to normal walking, but occurred earlier in synergies associated with non-dominant leg stance [55].
Under the narrow condition, when the first step of the sprint was taken, the soleus, gastrocnemius, rectus femoris, vasti, gluteus maximus, gluteus medius, biceps femoris, and adductors contributed less to propulsion and support [54].
Discussion
The aim of the current study was to systematically synthesize literature that investigated the gait changes induced by step width alterations from a biomechanical perspective. In the included 23 articles, a total of 399 healthy adults performed walking (n = 17/23), running (n = 4/23) or sprinting (n = 2/23) under different step width conditions and multiple biomechanical aspects were analyzed, including the joint kinematics, joint kinetics, spatiotemporal parameters, and EMG (muscle activities). The average score of the methodological quality was 9.39 out of 14, which indicates a “Fair” level of quality according to the Downs and Black quality assessment.
A major finding from this review was that step width alteration affected the joint kinematics and kinetics in all three planes of movement, such as peak rearfoot eversion angle and moment [11, 31], peak hip adduction angle and moment [11, 34,35,36,37], knee flexion moment [33], peak knee internal rotation angle as well as knee external rotation moment [11, 33, 37]. Another finding was that step width alterations do affect the stability and posture during walking, running and sprinting, and are expressed as the transformation of COM and MOS locations in anterior–posterior and mediolateral directions [8, 9, 47, 51, 53, 55, 56]. It was specifically reported that the muscle activity, GRF, spatiotemporal parameters, tibial stress, iliotibial band strain, and strain rate would be affected by different step width conditions [35, 37, 47,48,49, 52,53,54,55]. The study outcomes will be discussed in three categories, covering daily activities, clinical treatment, and athletic training.
Daily Activities
During daily activities, the strategies to prevent sports injuries and falls, especially among the elderly, have long been a focus of particular concern. One primary objective of human daily activity is to maintain stability and prevent falling. Adjusting the posture during gait occurs to actively control the COM variability and maintain trunk stability; further experiments showed that increasing step width increased trunk lean and, as a result, increased COM displacement and reduced knee abduction moment across the stance phase [57,58,59,60]. Narrow step width that reduced the support base during walking increased the need for active postural control and presented a greater challenge for stability [61, 62]. This finding also agreed with observations from the current systematic review, showing that the COM displacement variability increased in decreased step width and narrow steps [47, 55, 56]. Similarly, this finding was consistent with studies of MOS that found that walking with narrower steps exhibited poorer stability, as evidenced by reduced ML-MOS [9, 52], when paired with greater ML-MOS variability [8, 9], in particular in the elderly [9]. Therefore, narrow step widths should be avoided as much as possible to reduce the risk of balance loss and falling.
Clinical Treatment
Under the scenarios of clinical treatment, gait retraining for osteoarthritis (OA) individuals with an increased step width may be a suitable, noninvasive therapeutic option [32, 33, 36]. Reduced initial peak knee adduction moment and knee adduction moment angular impulse during gait were the results of wider step width [32]. The finding that gait adjustment could improve knee biomechanics related to knee OA was consistent with reports by Bennett et al. [33], investigating that peak knee adduction moment and impulse decreased in a wider step width with toe-in compared to normal walking. Furthermore, improvements also occurred in the hip joint as increased step width during gait reduced the peak hip adduction moment, making an effective compensatory mechanism to relieve hip OA as well as loading in the hip joint [36].
Altering step width during level walking and ascending and descending stairs would change lower limb biomechanics [63,64,65,66]. Although the stairs-related gait studies were not included in this systematic review, non-horizontal movements of stairs played important roles in improving daily activities for patients with knee OA. Previous investigations demonstrated that increased step width while descending stairs resulted in lower peak knee adduction angles and moments, which may suggest that lowering medial compartment knee loads might thus potentially reduce knee pain [63, 67]. However, while analyzing OA patients, the findings were the opposite, i.e. increased step width could not decrease internal knee abduction moments peak or knee pain [64]. When participants ascended the stairs, Paquette et al. [65] and Yocum et al. [66] found that increasing step width reduced knee extension and abduction ROM, peak knee abduction moments, knee abduction moment impulse, and GRF in the frontal plane. Consequently, increased step width would probably be an effective and easy gait modification for reducing joint loads and arthralgia in both OA individuals and healthy persons [32, 33, 36, 63,64,65,66]. This finding may have positive clinical significance to prevent disease progression.
Previous studies reported that symptomatic runners, such as those who suffer from patellofemoral pain (PFP) and iliotibial band syndrome (ITBS), exhibited different lower limb biomechanics [68,69,70,71,72,73,74]. In the prospective studies, peak hip adduction angles and knee internal rotation were found to be higher in runners who later suffered from ITBS [69, 72]. Knee internal abduction moment and impulse were also larger in runners with PFP [68, 73]. Nevertheless, the connection between peak hip adduction angle and PFP has been disputed with no consensus achieved [70, 71, 73, 74]. As for the variations in step width, it was found that the maximum knee internal rotation angle was greater during narrow step width compared to preferred step width [11, 37]. Consistent with the above literature, it was found that participants with narrower steps demonstrated that narrow step width in gait showed similar lower limb biomechanics in patients with ITBS [11, 34, 35, 37]. Specifically, the narrower step width displayed a higher average hip adduction angle compared to both normal and narrow step widths [34, 35]. On the other hand, both PFP runners and participants with narrow steps in gait showed greater peak knee abduction moment and impulse [11, 33, 35]. As a result, the biomechanics of asymptomatic runners were comparable to runners with lower limb injuries while running with small step widths. Additionally, runners with ITBS showed greater peak rearfoot inversion moments compared to asymptomatic runners [72]. Brindle et al. identified that the rearfoot inversion moment peak was reduced as step width increased from narrow to preferred and wide [11]. Based on these findings, while running with a wider step and avoiding narrower steps, the biomechanical parameters changed in the opposite way to runners with lower extremity disorders. Hence, the injury risks of runners with inappropriate frontal plane biomechanics may be reduced by raising the preferred step width.
OA patients and patients suffering from ITBS and tibial injuries may benefit from altering step width during running gait [30, 37, 48]. In addition to indirectly improving biomechanical parameters associated with ITBS [11, 34, 35, 37], the increased step width also directly and linearly reduced iliotibial band (ITB) strain and ITB strain rate during running [37]. Wider steps may be advantageous for the treatment and prevention of ITBS. A linearly increased step width could decrease tension on the tibia surface [48] and reduce the STJ moments during stance, thus reducing the work for the musculoskeletal system. The tibialis posterior tendon may experience less strain and stress as a result of the reduced STJ loading [30]. In summary, a wider step width may benefit runners with major general running-related musculoskeletal injuries (i.e. posterior tibial tendinopathy and tibial bone stress injuries) and runners who participated in ultra-marathon races with the most common running-related musculoskeletal injury (ITBS).
Sports Training
In sports training, especially during sprinting, the competition results and athletic performance may be affected by restricted starting step width and position [51, 54]. Compared to the natural sprint style, a restricted step width would decrease mediolateral propulsive impulse and first-step stance toe-off anterior velocity [51]. The natural sprint style in the first step exhibited greater mediolateral motion of the CoM, representing larger lateral external forces during the block and initial stance phases [51]. Furthermore, competitive sprinters with limited step width showed reduced extremity muscle contribution to propulsion and support, suggesting that narrower steps may suppress the muscles across the ankle and knee for maximal performance at sprinting start [54]. These findings suggested that the development of driving force during the first stance of the acceleration phase may be best achieved with a wider step width.
However, prior research demonstrated unequivocally that increased step width would raise metabolic expenditure during running and walking [5, 75, 76]. There was a U-shaped relationship between energy cost and step width [5]. Walking with a wider step width led to greater mechanical work by lower limb muscles to redirect the COM, which influenced the energy demand [75]. As per the biomechanical and physiological responses to increased step width, it could be inferred that step width may affect the running economy. Such work reported that lower vertical GRF, lower peak medial-lateral GRF, and lower anterior-posterior GRF were economic factors [77,78,79,80]. Greater lower limb muscular activity was also associated with running economy [80]. The obvious relationship between muscular activity and running economy derived from the fact that muscles required oxygen to activate, and greater lower limb muscular activity was expected to necessitate higher oxygen consumption and lead to a lower running economy [78, 80, 81]. Based on the investigations of step width, Sample et al. [35] and Wang et al. [54] found that medial GRF and vertical GRF increased with step width, and the muscle activation of soleus, gastrocnemius, rectus femoris, vasti, gluteus maximus, gluteus medius, biceps femoris, and adductors was increased with wider steps during running [54]. Hence, changes in biomechanical and physiological parameters from wider step width could imply reduced running and walking economy [82, 83]. Future studies should focus on the strategy of adjusting step widths during sprinting to achieve higher driving force at the start and higher running economy during distance running.
Limitations
Although the inclusion and exclusion criteria for this systematic review were strictly adhered to, there are still a few limitations that should be noted. Firstly, due to the lack of comparable data, this article did not carry out a meta-analysis of the research and data obtained. Secondly, step width was a crucial spatiotemporal variable with various internal (BMI, foot type, sex, age) and external (footwear, environment, activity level) factors that can contribute to the variations in biomechanical alteration during walking, running, and sprinting activities. Related variables have not been extensively deciphered and examined due to limited data and evidence in this review. Future research should take these potential confounding factors into account, develop well-designed experimental setups, and explore the effect of long-term changes in step width on gait biomechanics and the impact of gait retraining aiming to alter step width.
Conclusion
In summary, short-term changes in step width during walking, running and sprinting influenced multiple measures of lower extremity biomechanics. A narrower step width may result in poor balance and higher impact loading in the lower extremities during walking and running and may limit an athlete’s sprint performance. A wider step width may be beneficial in injury management, i.e., for patients with patellofemoral pain syndrome, iliotibial band syndrome or tibial bone stress injury, to re-distribute load. Wider steps increase the supporting base and typically enhance balance control, which in turn could reduce the risks of falling during daily activities. Our synthesis of published research related to biomechanics warrants consideration in the risk reduction of lower limb injuries and in the risk of falling during locomotion. Altering the step width is proposed as a simple and non-invasive treatment method in clinical practice.
Data Availability
The original datasets during this study are available upon request from the corresponding authors.
Abbreviations
- AP:
-
Anterior-Posterior
- COM:
-
Center of Mass
- EMG:
-
Electromyography
- GRF:
-
Ground Reaction Force
- ITBS:
-
Iliotibial Band Syndrome
- ML:
-
Mediolateral
- MOS:
-
Margin of Stability
- OA:
-
Osteoarthritis
- PFP:
-
Patellofemoral Pain
- PICO Model:
-
Patients, Intervention, Comparator, and Outcome model
- RCT:
-
Randomized Controlled Trial
- ROM:
-
Range of Motion
- STJ:
-
Subtalar Joint
References
Napier C, Cochrane CK, Taunton JE, Hunt MA. Gait modifications to change lower extremity gait biomechanics in runners: a systematic review. Br J Sports Med. 2015;49:1382–8. https://doi.org/10.1136/bjsports-2014-094393.
Schubert AG, Kempf J, Heiderscheit BC. Influence of stride frequency and length on running mechanics. Sports Health: Multidisciplinary Approach. 2013;6:210–7. https://doi.org/10.1177/1941738113508544.
Barton CJ, Bonanno DR, Carr J, Neal BS, Malliaras P, Franklyn-Miller A, Menz HB. Running retraining to treat lower limb injuries: a mixed-methods study of current evidence synthesised with expert opinion. Br J Sports Med. 2016;50:513–26. https://doi.org/10.1136/bjsports-2015-095278.
Willwacher S, Kurz M, Robbin J, Thelen M, Hamill J, Kelly L, Mai P. Running-related biomechanical risk factors for overuse injuries in Distance runners: a systematic review considering Injury specificity and the potentials for Future Research. Sports Med. 2022;52:1863–77. https://doi.org/10.1007/s40279-022-01666-3.
Arellano CJ, Kram R. The effects of step width and arm swing on energetic cost and lateral balance during running. J Biomech. 2011;44:1291–5. https://doi.org/10.1016/j.jbiomech.2011.01.002.
Gomez-Molina J, Ogueta-Alday A, Stickley C, Camara J, Cabrejas-Ugartondo J, Garcia-Lopez J. Differences in Spatiotemporal Parameters between Trained Runners and untrained participants. J Strength Cond Res. 2017;31:2169–75. https://doi.org/10.1519/JSC.0000000000001679.
de Ruiter CJ, Verdijk PW, Werker W, Zuidema MJ, de Haan A. Stride frequency in relation to oxygen consumption in experienced and novice runners. Eur J Sport Sci. 2014;14:251–8. https://doi.org/10.1080/17461391.2013.783627.
Young PMM, Dingwell JB. Voluntary changes in step width and step length during human walking affect dynamic margins of stability. Gait Posture. 2012;36:219–24. https://doi.org/10.1016/j.gaitpost.2012.02.020.
Arvin M, Mazaheri M, Hoozemans MJM, Pijnappels M, Burger BJ, Verschueren SMP, van Dieen JH. Effects of narrow base gait on mediolateral balance control in young and older adults. J Biomech. 2016;49:1264–7. https://doi.org/10.1016/j.jbiomech.2016.03.011.
Abram SJ, Selinger JC, Donelan JM. Energy optimization is a major objective in the real-time control of step width in human walking. J Biomech. 2019;91:85–91. https://doi.org/10.1016/j.jbiomech.2019.05.010.
Brindle RA, Milner CE, Zhang S, Fitzhugh EC. Changing step width alters lower extremity biomechanics during running. Gait Posture. 2014;39:124–8. https://doi.org/10.1016/j.gaitpost.2013.06.010.
Cho SH, Park JM, Kwon OY. Gender differences in three dimensional gait analysis data from 98 healthy Korean adults. Clin Biomech (Bristol Avon). 2004;19:145–52. https://doi.org/10.1016/j.clinbiomech.2003.10.003.
Lymbery JK, Gilleard W. The stance phase of walking during late pregnancy - temporospatial and ground reaction force variables. J Am Podiatr Med Assoc. 2005;95:247–53. https://doi.org/10.7547/0950247.
Spees VJ, Duren DL, Siervogel RM. The influence of Thigh Circumference and Waist-to-hip ratio on step Width in a large sample of women. Med Sci Sports Exerc. 2005;37(S156–S157). https://doi.org/10.1249/00005768-200505001-00839.
Dean JC, Alexander NB, Kuo AD. The effect of lateral stabilization on walking in young and old adults. IEEE Trans Bio Med Eng. 2007;54:1919–26. https://doi.org/10.1109/tbme.2007.901031.
Schrager MA, Kelly VE, Price R, Ferrucci L, Shumway-Cook A. The effects of age on medio-lateral stability during normal and narrow base walking. Gait Posture. 2008;28:466–71. https://doi.org/10.1016/j.gaitpost.2008.02.009.
Vartiainen P, Bragge T, Lyytinen T, Hakkarainen M, Karjalainen PA, Arokoski JP. Kinematic and kinetic changes in obese gait in bariatric surgery-induced weight loss. J Biomech. 2012;45:1769–74. https://doi.org/10.1016/j.jbiomech.2012.05.002.
Wu X, Lockhart TE, Yeoh HT. Effects of obesity on slip-induced fall risks among young male adults. J Biomech. 2012;45:1042–7. https://doi.org/10.1016/j.jbiomech.2011.12.021.
Gilleard WL. Trunk motion and gait characteristics of pregnant women when walking: report of a longitudinal study with a control group. BMC Pregnancy Childbirth. 2013;13:71. https://doi.org/10.1186/1471-2393-13-71.
Bertuit J, Feipel V, Rooze M. Temporal and spatial parameters of gait during pregnancy. Acta Bioeng Biomech. 2015;17:93–101.
Ro DH, Lee DY, Moon G, Lee S, Seo SG, Kim SH, Park IW, Lee MC. Sex differences in knee joint loading: cross-sectional study in geriatric population. J Orthop Research: Official Publication Orthop Res Soc. 2017;35:1283–9. https://doi.org/10.1002/jor.23374.
Mei Q, Gu Y, Xiang L, Baker JS, Fernandez J. Foot Pronation contributes to altered Lower Extremity Loading after Long Distance running. Front Physiol. 2019;10:573. https://doi.org/10.3389/fphys.2019.00573.
Shin HS, Lee JH, Kim EJ, Kyung MG, Yoo HJ, Lee DY. Flatfoot deformity affected the kinematics of the foot and ankle in proportion to the severity of deformity. Gait Posture. 2019;72:123–8. https://doi.org/10.1016/j.gaitpost.2019.06.002.
Summa S, De Peppo F, Petrarca M, Caccamo R, Carbonetti R, Castelli E, Ottavio Adorisio D. Gait changes after weight loss on adolescent with severe obesity after sleeve gastrectomy. Surg Obes Relat Diseases: Official J Am Soc Bariatr Surg. 2019;15:374–81. https://doi.org/10.1016/j.soard.2019.01.007.
Thies SB, Richardson JK, Demott T, Ashton-Miller JA. Influence of an irregular surface and low light on the step variability of patients with peripheral neuropathy during level gait. Gait Posture. 2005;22:40–5. https://doi.org/10.1016/j.gaitpost.2004.06.006.
Hollander K, Riebe D, Campe S, Braumann KM, Zech A. Effects of footwear on treadmill running biomechanics in preadolescent children. Gait Posture. 2014;40:381–5. https://doi.org/10.1016/j.gaitpost.2014.05.006.
Kent JA, Sommerfeld JH, Mukherjee M, Takahashi KZ, Stergiou N. Locomotor patterns change over time during walking on an uneven surface. J Exp Biol. 2019;222. https://doi.org/10.1242/jeb.202093.
Ozdinc S, Ulucam E. Effects of Masai Barefoot Technology Footwear Compared with Barefoot and Oxford Footwear on Gait. J Am Podiatr Med Assoc. 2021;111. https://doi.org/10.7547/17-175.
Wang Y, Jiang H, Yu L, Gao Z, Liu W, Mei Q, Gu Y. Understanding the role of children’s footwear on children’s feet and Gait Development: a systematic scoping review. Healthcare. 2023;11. https://doi.org/10.3390/healthcare11101418.
Maharaj JN, Murry LE, Cresswell AG, Lichtwark GA. Increasing step width reduces the requirements for subtalar joint moments and powers. J Biomech. 2019;92:29–34. https://doi.org/10.1016/j.jbiomech.2019.05.021.
Pohl MB, Messenger N, Buckley JG. Changes in foot and lower limb coupling due to systematic variations in step width. Clin Biomech (Bristol Avon). 2006;21:175–83. https://doi.org/10.1016/j.clinbiomech.2005.09.005.
Favre J, Erhart-Hledik JC, Chehab EF, Andriacchi TP. General scheme to reduce the knee adduction moment by modifying a combination of gait variables. J Orthop Research: Official Publication Orthop Res Soc. 2016;34:1547–56. https://doi.org/10.1002/jor.23151.
Bennett HJ, Shen G, Cates HE, Zhang S. Effects of toe-in and toe-in with wider step width on level walking knee biomechanics in varus, valgus, and neutral knee alignments. Knee. 2017;24:1326–34. https://doi.org/10.1016/j.knee.2017.08.058.
Kikel M, Gecelter R, Thompson NE. Is step width decoupled from pelvic motion in human evolution? Sci Rep. 2020;10(7806). https://doi.org/10.1038/s41598-020-64799-3.
Sample DW, Thorsen TA, Weinhandl JT, Strohacker KA, Zhang S. Effects of increased step-width on knee biomechanics during inclined and declined walking. J Appl Biomech. 2020;1–6. https://doi.org/10.1123/jab.2019-0298.
Stief F, Holder J, Feja Z, Lotfolahpour A, Meurer A, Wilke J. Impact of subject-specific step width modification on the knee and hip adduction moments during gait. Gait Posture. 2021;89:161–8. https://doi.org/10.1016/j.gaitpost.2021.07.008.
Meardon SA, Campbell S, Derrick TR. Step width alters iliotibial band strain during running. Sports Biomech. 2012;11:464–72. https://doi.org/10.1080/14763141.2012.699547.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84. https://doi.org/10.1136/jech.52.6.377.
Hollander K, Heidt C, BC VDZ, Braumann KM, Zech A. Long-Term effects of Habitual Barefoot running and walking: a systematic review. Medicine and science in sports and exercise 2017, 49, 752–62, https://doi.org/10.1249/MSS.0000000000001141.
Hollander K, Zech A, Rahlf AL, Orendurff MS, Stebbins J, Heidt C. The relationship between static and dynamic foot posture and running biomechanics: a systematic review and meta-analysis. Gait Posture. 2019;72:109–22. https://doi.org/10.1016/j.gaitpost.2019.05.031.
Zandbergen MA, Marotta L, Bulthuis R, Buurke JH, Veltink PH, Reenalda J. Effects of level running-induced fatigue on running kinematics: a systematic review and meta-analysis. Gait Posture. 2023;99:60–75. https://doi.org/10.1016/j.gaitpost.2022.09.089.
Hooper P, Jutai JW, Strong G, Russell-Minda E. Age-related macular degeneration and low-vision rehabilitation: a systematic review. Can J Ophthalmol. 2008;43:180–7. https://doi.org/10.3129/i08-001.
Farrah K, Young K, Tunis MC, Zhao L. Risk of bias tools in systematic reviews of health interventions: an analysis of PROSPERO-registered protocols. Syst Rev. 2019;8:280. https://doi.org/10.1186/s13643-019-1172-8.
Singer JC, Prentice SD, McIlroy WE. Dynamic stability control during volitional stepping: a focus on the restabilisation phase at movement termination. Gait Posture. 2012;35:106–10. https://doi.org/10.1016/j.gaitpost.2011.08.018.
Young PMM, Dingwell JB. Voluntarily changing step length or step width affects dynamic stability of human walking. Gait Posture. 2012;35:472–7. https://doi.org/10.1016/j.gaitpost.2011.11.010.
Nagano H, Begg R, Sparrow WA. Ageing effects on medio-lateral balance during walking with increased and decreased step width. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference 2013, 2013, 7467–7470, https://doi.org/10.1109/embc.2013.6611285.
Meardon SA, Derrick TR. Effect of step width manipulation on tibial stress during running. J Biomech. 2014;47:2738–44. https://doi.org/10.1016/j.jbiomech.2014.04.047.
Kubinski SN, McQueen CA, Sittloh KA, Dean JC. Walking with wider steps increases stance phase gluteus medius activity. Gait Posture. 2015;41:130–5. https://doi.org/10.1016/j.gaitpost.2014.09.013.
Bajelan S, Nagano H, Sparrow T, Begg RK. Effects of wide step walking on swing phase hip muscle forces and spatio-temporal gait parameters. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference 2017, 2017, 954–957, https://doi.org/10.1109/embc.2017.8036983.
Sandamas P, Gutierrez-Farewik EM, Arndt A. The effect of a reduced first step width on starting block and first stance power and impulses during an athletic sprint start. J Sports Sci. 2019;37:1046–54. https://doi.org/10.1080/02640414.2018.1541161.
Rawal YR, Singer JC. The influence of net ground reaction force orientation on mediolateral stability during walking. Gait Posture. 2021;90:73–9. https://doi.org/10.1016/j.gaitpost.2021.08.009.
Shih HS, Gordon J, Kulig K. Trunk control during gait: walking with wide and narrow step widths present distinct challenges. J Biomech. 2021;114:110135. https://doi.org/10.1016/j.jbiomech.2020.110135.
Wang R, de Martín L, Sandamas P, Arndt A, Gutierrez-Farewik EM. The Effect of Step Width on muscle contributions to body Mass Center Acceleration during the first stance of sprinting. Front Bioeng Biotechnol. 2021;9:636960. https://doi.org/10.3389/fbioe.2021.636960.
Alizadehsaravi L, Bruijn SM, Muijres W, Koster RAJ, van Dieen JH. Improvement in gait stability in older adults after ten sessions of standing balance training. PLoS ONE. 2022;17. https://doi.org/10.1371/journal.pone.0242115.
Magnani RM, van Dieën JH, Bruijn SM. Effects of vestibular stimulation on gait stability when walking at different step widths. Exp Brain Res. 2023;241:49–58. https://doi.org/10.1007/s00221-022-06488-3.
Arvin M, van Dieen JH, Bruijn SM. Effects of constrained trunk movement on frontal plane gait kinematics. J Biomech. 2016;49:3085–9. https://doi.org/10.1016/j.jbiomech.2016.07.015.
Rebula JR, Ojeda LV, Adamczyk PG, Kuo AD. The stabilizing properties of foot yaw in human walking. J Biomech. 2017;53:1–8. https://doi.org/10.1016/j.jbiomech.2016.11.059.
Anderson J, King S, Przybyla A, Ranganath L, Barton G. Reduction of frontal plane knee load caused by lateral trunk lean depends on step width. Gait Posture. 2018;61:483–7. https://doi.org/10.1016/j.gaitpost.2018.02.022.
Best AN, Martin JP, Li Q, Wu AR. Stepping behaviour contributes little to balance control against continuous mediolateral trunk perturbations. J Exp Biol. 2019;222. https://doi.org/10.1242/jeb.212787.
Donelan JM, Shipman DW, Kram R, Kuo AD. Mechanical and metabolic requirements for active lateral stabilization in human walking. J Biomech. 2004;37:827–35. https://doi.org/10.1016/j.jbiomech.2003.06.002.
Perry JA, Srinivasan M. Walking with wider steps changes foot placement control, increases kinematic variability and does not improve linear stability. Royal Soc open Sci. 2017;4:160627. https://doi.org/10.1098/rsos.160627.
Paquette MR, Zhang S, Milner CE, Fairbrother JT, Reinbolt JA. Effects of increased step width on frontal plane knee biomechanics in healthy older adults during stair descent. Knee. 2014;21:821–6. https://doi.org/10.1016/j.knee.2014.03.006.
Paquette MR, Zhang S, Milner CE, Klipple G. Does increasing step width alter knee biomechanics in medial compartment knee osteoarthritis patients during stair descent? Knee. 2014;21:676–82. https://doi.org/10.1016/j.knee.2014.02.020.
Paquette MR, Klipple G, Zhang S. Greater Step Widths reduce internal knee abduction moments in medial compartment knee osteoarthritis patients during stair ascent. J Appl Biomech. 2015;31:229–36. https://doi.org/10.1123/jab.2014-0166.
Yocum D, Weinhandl JT, Fairbrother JT, Zhang S. Wide step width reduces knee abduction moment of obese adults during stair negotiation. J Biomech. 2018;75:138–46. https://doi.org/10.1016/j.jbiomech.2018.05.002.
Thompson NE, O’Neill MC, Holowka NB, Demes B. Step width and frontal plane trunk motion in bipedal chimpanzee and human walking. J Hum Evol. 2018;125:27–37. https://doi.org/10.1016/j.jhevol.2018.09.006.
Stefanyshyn DJ, Stergiou P, Lun VM, Meeuwisse WH, Worobets JT. Knee angular impulse as a predictor of patellofemoral pain in runners. Am J Sports Med. 2006;34:1844–51. https://doi.org/10.1177/0363546506288753.
Noehren B, Davis I, Hamill J. ASB clinical biomechanics award winner 2006 prospective study of the biomechanical factors associated with iliotibial band syndrome. Clin Biomech (Bristol Avon). 2007;22:951–6. https://doi.org/10.1016/j.clinbiomech.2007.07.001.
Willson JD, Davis IS. Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands. Clin Biomech (Bristol Avon). 2008;23:203–11. https://doi.org/10.1016/j.clinbiomech.2007.08.025.
Souza RB, Powers CM. Predictors of hip internal rotation during running: an evaluation of hip strength and femoral structure in women with and without patellofemoral pain. Am J Sports Med. 2009;37:579–87. https://doi.org/10.1177/0363546508326711.
Ferber R, Noehren B, Hamill J, Davis IS. Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. J Orthop Sports Phys Ther. 2010;40:52–8. https://doi.org/10.2519/jospt.2010.3028.
Dierks TA, Manal KT, Hamill J, Davis I. Lower extremity kinematics in runners with patellofemoral pain during a prolonged run. Med Sci Sports Exerc. 2011;43:693–700. https://doi.org/10.1249/MSS.0b013e3181f744f5.
Noehren B, Pohl MB, Sanchez Z, Cunningham T, Lattermann C. Proximal and distal kinematics in female runners with patellofemoral pain. Clin Biomech (Bristol Avon). 2012;27:366–71. https://doi.org/10.1016/j.clinbiomech.2011.10.005.
Donelan JM, Kram R, Kuo AD. Mechanical and metabolic determinants of the preferred step width in human walking. Proc Biol Sci. 2001;268:1985–92. https://doi.org/10.1098/rspb.2001.1761.
Shorter KA, Wu A, Kuo AD. The high cost of swing leg circumduction during human walking. Gait Posture. 2017;54:265–70. https://doi.org/10.1016/j.gaitpost.2017.03.021.
Williams KR, Cavanagh PR. Relationship between distance running mechanics, running economy, and performance. J Appl Physiol (Bethesda Md : 1985). 1987;63:1236–45. https://doi.org/10.1152/jappl.1987.63.3.1236.
Kyrolainen H, Belli A, Komi PV. Biomechanical factors affecting running economy. Medicine and science in sports and exercise 2001, 33, 1330–7, https://doi.org/10.1097/00005768-200108000-00014.
Moore IS, Jones AM, Dixon SJ. Mechanisms for improved running economy in beginner runners. Med Sci Sports Exerc. 2012;44:1756–63. https://doi.org/10.1249/MSS.0b013e318255a727.
Moore IS. Is there an economical running technique? A review of modifiable biomechanical factors affecting running economy. Sports Med. 2016;46:793–807. https://doi.org/10.1007/s40279-016-0474-4.
Abe D, Muraki S, Yanagawa K, Fukuoka Y, Niihata S. Changes in EMG characteristics and metabolic energy cost during 90-min prolonged running. Gait Posture. 2007;26:607–10. https://doi.org/10.1016/j.gaitpost.2006.12.014.
Molitor SL, Neptune RR. Lower-limb joint quasi-stiffness in the frontal and sagittal planes during walking at different step widths. J Biomech. 2024;162:111897. https://doi.org/10.1016/j.jbiomech.2023.111897.
Bruijn SM, van Dieen JH. Control of human gait stability through foot placement. J R Soc Interface. 2018;15. https://doi.org/10.1098/rsif.2017.0816.
Acknowledgements
Not applicable.
Funding
This study was sponsored by the National Natural Science Foundation of China (No. 12202216), Ningbo Natural Science Foundation (2023J128), the “Mechanics+” Interdisciplinary Top Innovative Youth Fund Project of Ningbo University (GC2024006), the Key R&D Program of Zhejiang Province China (2021C03130), Zhejiang Province Science Fund for Distinguished Young Scholars (LR22A020002), Ningbo University Teaching and Research project (JYXM2023051), SRIP project of Ningbo University (2023SRIP501, 2023SRIP502, 2023SRIP510) and K. C. Wong Magna Fund in Ningbo University.
Author information
Authors and Affiliations
Contributions
Conceptualization: YW, QM, HJ, JF and YG; methodology: YW, QM, HJ, KH and PVB; data analyses: YW, QM and JH; writing—original draft preparation: YW, QM, JH, KH and PVB; writing—review and editing: QM, KH, PVB, JF and YG. All authors approved the final manuscript for publication.
Corresponding authors
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing Interests
None to be declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, Y., Mei, Q., Jiang, H. et al. The Biomechanical Influence of Step Width on Typical Locomotor Activities: A Systematic Review. Sports Med - Open 10, 83 (2024). https://doi.org/10.1186/s40798-024-00750-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-024-00750-4