
Abstract
Background
Inorganic nitrate (NO3−) supplementation is purported to benefit short-term exercise performance, but it is unclear whether NO3− improves longer-term exercise training responses (such as improvements in VO2peak or time to exhaustion (TTE)) versus exercise training alone. The purpose of this systematic review and meta-analysis was to determine the effects of NO3− supplementation combined with exercise training on VO2peak and TTE, and to identify potential factors that may impact outcomes.
Methods
Electronic databases (PubMed, Medscape, and Web of Science) were searched for articles published through June 2022 with article inclusion determined a priori as: (1) randomized placebo-controlled trials, (2) exercise training lasted at least three weeks, (3) treatment groups received identical exercise training, (4) treatment groups had matched VO2peak at baseline. Study quality was assessed using the Cochrane Risk-of-Bias 2 tool. Standardized mean difference (SMD) with 95% confidence intervals (CI) were calculated using restricted maximum likelihood estimation between pre- and post-training differences in outcomes. Moderator subgroup and meta-regression analyses were completed to determine whether the overall effect was influenced by age, sex, NO3− dosage, baseline VO2peak, health status, NO3− administration route, and training conditions.
Results
Nine studies consisting of eleven trials were included: n = 228 (72 females); age = 37.7 ± 21 years; VO2peak: 40 ± 18 ml/kg/min. NO3− supplementation did not enhance exercise training with respect to VO2peak (SMD: 0.18; 95% CI: -0.09, 0.44; p = 0.19) or TTE (SMD: 0.08; 95% CI: − 0.21, 0.37; p = 0.58). No significant moderators were revealed on either outcome. Subset analysis on healthy participants who consumed beetroot juice (BRJ) revealed stronger trends for NO3− improving VO2peak (p = 0.08) compared with TTE (p = 0.19), with no significant moderators. Sunset funnel plot revealed low statistical power in all trials.
Conclusions
NO3− supplementation combined with exercise training may not enhance exercise outcomes such as VO2peak or TTE. A trend for greater improvement in VO2peak in healthy participants supplemented with BRJ may exist (p = 0.08). Overall, future studies in this area need increased sample sizes, more unified methodologies, longer training interventions, and examination of sex as a biological variable to strengthen conclusions.
Key Points
-
Despite the increased use and study of NO3− supplementation, most of these data have shown benefits during acute supplementation on exercise rather than a benefit to chronic training outcomes.
-
This systematic review and meta-analysis revealed non-significant improvements in VO2peak or time to exhaustion after exercise training with NO3- supplementation compared to exercise alone. A trend for improvement was found for improvements in healthy participants taking beetroot juice supplementation.
-
These results suggest that NO3- may not have an impact on improving longer term training outcomes, but studies in this area suffer from low sample sizes and inconsistent study designs.
Similar content being viewed by others


Background
Inorganic nitrate (NO3−) is found in high abundance in various green leafy vegetables and roots. Although NO3− itself is thought to be relatively inert, it is converted via entero-salivary bacterial reduction in the oral cavity and gut to nitrite (NO2−) [1, 2]. Subsequently, NO2− can be converted to nitric oxide (NO) in conditions of low oxygen tension and mildly acidic pH in a process facilitated by deoxyhemoglobin and enzymes such as xanthine oxidase [3]. Therefore, exercise at a relatively high-intensity results in conditions favorable for increased reduction of NO2− to NO. NO has been shown to play a potentially beneficial role in several physiological processes linked to exercise performance, including increased blood flow and O2 delivery [4, 5], increased microvascular PO2 [6], improved muscular contractility [7, 8], and reduced O2 cost of exercise [9,10,11] by enhancing mitochondrial function [12]. This suggests a potential for enhanced exercise training benefits, as NO may increase acute exercise responses which may in turn accumulate into an increased training response. Contrarily, these acute findings are equivocal, and it is possible that factors such as the decreased exercise-induced muscle perturbations found after NO3− supplementation [13] may result in lessened adaptation in response to exercise training.
The role of exogenous NO3− supplementation in human exercise performance has generated a great deal of academic interest in the last decade [14]. Several high-quality meta-analyses have been performed, and most recently an expert consensus paper using the modified Delphi technique concluded that acute and chronic NO3− supplementation was likely safe up to 16 mmol/day when consumed over several weeks, and that it is likely to produce ergogenic benefits during acute exercise in individuals with lower and more moderate aerobic fitness (i.e., those with VO2peak > 60 ml/kg/min have shown generally less benefit) [15]. Despite this, whether NO3− supplementation causes acute improvements in factors such as exercise endurance in each exercise training session, subsequently resulting in an accumulated larger training volume and greater adaptation for outcomes such as VO2peak, remains unclear.
VO2peak is considered the criterion measure of cardiorespiratory adaptation to exercise training [16, 17]. VO2peak improves with exercise training via multifaceted improvements in oxygen delivery (e.g., stroke volume, blood volume) and oxygen utilization (e.g., a-vO2 difference), and is a predictor of both endurance capacity and mortality/morbidity [18]. Although VO2peak primarily quantifies aerobic fitness, there is considerable variability in the endurance capacity of individuals with similar VO2peak [19]. More practical measures such as exercise time-to-exhaustion (TTE) may better represent competitive endurance performance (as this is likely to be more closely related to the percent of VO2peak associated with the lactate threshold and/or the lactate turn point) and offer additional insight into exercise training adaptations. As such, many exercise training studies evaluate changes to both VO2peak and TTE in a relatively consistent manner, making comparison across studies possible.
The purpose of this systematic review and meta-analysis is to explore whether NO3− supplementation can provide additional benefits when combined with chronic exercise training, and to determine whether factors such as baseline fitness, sex, health status, NO3− dosage, route of NO3− administration, and training conditions may moderate the effects of NO3− on training outcomes.
Methods
This systematic review and meta-analysis was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [20] but was not pre-registered. Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia) was used for title, abstract, and full-text screening.
Literature Search
Electronic databases (PubMed, Medscape, and Web of Science) were searched by two authors in tandem, ACH and JOZ, with articles published from inception of the databases through June 2022 included. The search used the following terms: (((((("Dietary nitrate") OR ("Inorganic nitrate")) AND (Training)) NOT (Acute)) NOT (Rat)) NOT (rodent)) NOT (mouse)). Reference lists of all relevant studies along with reviews and book chapters were also examined. Articles were limited to randomized controlled trials (RCTs) in the English language.
Article Selection
For this meta-analysis, the term ‘article’ is used synonymously with ‘study’, and ‘trial’ is the unit included in the meta-analysis. Articles sometimes contained multiple eligible trials that comprised an intervention group and a comparable control.
First, the titles and abstracts of the articles were screened for eligibility. The following criteria were determined a priori for article inclusion: (1) the study was a RCT, (2) exercise training (i.e., repeated bouts of exercise multiple times per week) lasted at least 3 weeks, (3) the placebo and NO3− group received identical exercise training, (4) the placebo and NO3− had matched VO2peak at baseline. Full texts were reviewed of the remaining articles to determine eligibility. Two authors (ACH and JOZ) independently completed the study selection.
Data Extraction and Bias Assessment
Articles meeting inclusion criteria had the following data extracted and systematically organized: (1) author and publication year; (2) continuous variables: change in VO2peak, change in time to exhaustion, sample size, baseline VO2peak, age, body weight (kg), duration of training intervention, and NO3− dosage both in mmol and in mmol/kg/day; (3) categorical variables: sex, route of NO3− administration, environmental oxygenation during training, training intensity, health status, training modality, and whether an acute dose of NO3− was taken prior to the final post-training testing. If NO3− mmol/kg/day data were not provided, they were manually calculated based on mmol and mean kg data. If data were not available in the articles, authors were contacted for data.
Study quality was assessed using the Cochrane risk-of-bias tool for randomized trials (RoB 2) for both outcomes which includes the following domains: randomization, deviations from interventions, missing outcome data, measurement of outcome data, and results [21]. In each domain are signaling questions, where the risk of bias calculated from each domain is generated from an algorithm. Each study is scored as either “low risk”, “high risk” or “some concern” of bias based on the answers to the signaling questions. Two authors (ACH and JOZ) independently answered the signaling questions. Additionally, the Grading of Recommendations Assessment, Development and Evaluation (GRADE) using GRADEPro was performed to assess the certainty of evidence for the outcomes and sensitivity analyses. Certainty of evidence for each outcome was assessed using the following scale: “high,” “moderate,” “low,” or “very low” certainty. Certainty of each outcome was downgraded due to (1) risk of bias/study limitations, (2) inconsistency in results, (3) indirectness of results, (4) imprecision, or (5) reporting/publication bias. Two authors (ACH and CP) independently assessed the certainty of evidence.
Statistical Analysis
The meta-analysis and subgroup analysis was performed using Open Meta-Analyst, whereas funnel plots, Cook’s distance, studentized residuals, and sunset plots [22] were calculated and plotted using ‘metafor’ [23] in RStudio (Version 1.3.1073). Data were considered statistically significant a priori at p < 0.05 and data are presented as standardized mean difference (SMD).
A random effects model with restricted maximum likelihood estimation was utilized. The SMD of both VO2peak and TTE between the NO3− groups and the placebo groups of each trial were utilized in the model to determine the pooled effect. SMD was utilized due to inconsistent reporting of VO2peak in absolute or relative units. The SMDs are expressed as Hedges' g to account for any bias due to small sample sizes within trials. The Hedges' g values are interpreted as follows: ≤ 0.2, 0.2, 0.5, and 0.8 are considered to represent trivial, small, moderate, and large effect sizes, respectively [24].
The robustness of the pooled results was examined via funnel plots for small study effects. Sensitivity analysis was performed using Cook's distance and studentized residuals to identify potentially influential or outlying trials, respectively [25]. If a study was identified as being potentially influential or outlying, the robustness of the overall analysis was tested by removing the identified trial(s). A second sensitivity analysis was performed on only studies administering NO3− in the form of beetroot juice (BRJ) in healthy participants only. Statistical heterogeneity of the overall model was assessed with using Cochrane’s Q and I2, where < 25% indicates low risk of heterogeneity, 25–75% indicates moderate risk of heterogeneity, and > 75% indicates considerable risk of heterogeneity [26]. A sunset funnel plot was used to visualize the statistical power of each trial [27].
Moderator analysis was performed to determine whether the following subgroups impacted pooled effects: sex, health status, route of NO3− administration, and whether participants trained under normoxic or hypoxic conditions. While training intensity and modality were of interest, the included trials that had healthy populations all trained both at a high intensity while cycling, whereas all trials included that had clinical populations trained at a moderate intensity on a treadmill. Because of this, subgroup analysis for health status was the same subgroup for exercise intensity and modality. Meta-regressions were also performed to determine whether the following continuous variables impacted pool effects: age, weight, baseline VO2peak, NO3− dosage in mmol per day, and NO3− dosage in mmol/kg/day. The regression coefficient (ß) is reported along with 95% confidence intervals (CI).
Results
Literature Search
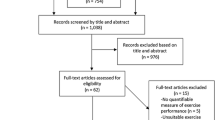
The PRISMA flow diagram outlining the literature search is presented in Fig. 1. In total, 144 references were imported for screening, with 47 duplicates removed leaving 97 studies screened against title and abstract. Following screening of titles and abstracts (ACH and JOZ), 84 studies were excluded leaving 13 studies assessed for full-text eligibility. Of these, 4 studies were excluded, leaving 9 studies [28,29,30,31,32,33,34,35,36] which met inclusion criteria containing 11 eligible trials. The trial participant and supplement characteristics are shown in Table 1, while the trial exercise training characteristics are shown in Table 2.

Flowchart of article and trial selection
Risk of Bias
Both outcomes produced similar results on the RoB analysis. Of the 9 included studies, 7 were considered to have a low risk of bias, with 2 having some concern due to the nature of their single-blinded supplement design [33] or lack of explicit mentioning of double-blinding [31] (Additional file 1: Figure S1).
Pooled Effects
The overall model indicated that NO3− supplementation did not improve exercise training responses on VO2peak beyond exercise alone (n = 11 trials, SMD = 0.18; 95% confidence interval (CI): − 0.09, 0.44; p = 0.19; Fig. 2). There was no significant statistical heterogeneity present within this analysis (Q = 6.7, df = 10, p = 0.76, I2 = 0%, p = 0.76). Sensitivity analysis identified one trial [31] as potentially outlying/influential (Additional file 1: Figure S2), but removal of this trial had no significant effect on the observed effect. For the secondary outcome, the overall model indicated that NO3− supplementation did not improve exercise training responses on TTE beyond exercise alone (n = 9 trials, SMD = 0.08; 95% CI: − 0.21, 0.37; p = 0.58, Fig. 3). There was no significant statistical heterogeneity present within this analysis (Q = 3.7; df = 8; p = 0.88; I2 = 0%, p = 0.88).

Forest plot of VO2peak. [32a] Heart failure trial. [32b] Hypertension trial. [35a] Beetroot juice trial. [35b] Potassium nitrate trial

Forest Plot of Time to Exhaustion (TTE). [32a] Heart failure trial. [32b] Hypertension trial. [35a] Beetroot juice trial. [35b] Potassium nitrate trial
Outliers, Influence, and Power
Examination of studentized residuals for trials included in the VO2peak model were analyzed, revealing no indication of outliers in this model. One study was deemed influential according to Cook’s distance for VO2peak [31]. Removal of this study did not change the lack of significant effect of NO3− supplementation on training for the pooled outcome for VO2peak, although it did greatly reduce the effect size (SMD = 0.08; 95% CI: − 0.19, 0.36; p = 0.55). This study had large improvements in VO2peak in the NO3− group compared to the placebo group, but this study was identified as having “some concerns” in the risk of bias assessment due to the potential single-blinded nature of the study design. Visual inspection of the funnel plot for VO2peak also revealed that the one study that was detected as influential by Cook’s distance also had a large effect size (Additional file 1: Figure S2), although neither the rank correlation nor the regression test indicated any funnel plot asymmetry (p = 0.76 and p = 0.96, respectively). All other studies removed during sensitivity analysis had no substantial effect on the overall model.
Examination of studentized residuals for studies included in the TTE model were analyzed, revealing no indication of outliers in this model. According to Cook’s distance, none of the studies were considered influential. Visual inspection of the funnel plot for TTE did not reveal any asymmetry (Additional file 1: Figure S3), and neither the rank correlation nor the regression test indicated any funnel plot asymmetry (p = 0.76 and p = 0.85, respectively). All studies removed during sensitivity analysis had no substantial effect on the overall model.
Examination of the sunset funnel plot (Additional file 1: Figure S4) shows that at the pre-determined α = 0.05, the median power of all trials included in this meta-analysis was 6.7%, with an average effect size of 0.68 and 1.07 required for statistical power levels of 33% and 66%, respectively.
Subgroup Analysis
Moderator subgroup analyses for VO2peak and TTE are shown in Tables 3 and 4, respectively. Subgroup analyses showed no significant moderation of sex, health status, route of NO3− administration, level of training oxygenation, or the presence of an acute NO3− dose prior to post-testing on either VO2peak or TTE (all p > 0.05). Similarly, all meta-regressions performed did not reveal baseline VO2peak, age, body weight, duration of training intervention, NO3− dose, or NO3− dose normalized to bodyweight to be significant moderators on either VO2peak or TTE (Table 5; all p > 0.05).
Sensitivity Analysis
As there is evidence in the literature suggesting that BRJ may provide more favorable benefits than other forms of NO3− supplementation, a separate model was performed including only healthy participants who consumed NO3− via BRJ (Additional file 1: Figure S5). Although this model revealed a trend for BRJ benefiting VO2peak improvement beyond exercise training alone (SMD = 0.35; 95% CI: − 0.04, 0.75; p = 0.08), removal of the study previously identified as being influential [31] eliminated the observed trend (SMD = 0.16; 95% CI: − 0.01, 0.88; p = 0.46). Moderator analysis on this subset of data did not reveal any significant moderators (Additional file 1: Table S1; all p > 0.05). The sensitivity analysis model performed with TTE as an outcome showed no significant effect of NO3− consumed as BRJ in healthy participants (SMD = 0.26; 95% CI: − 0.13, 0.65; p = 0.19) (Additional file 1: Figure S6). Moderator analysis on this subset did not reveal any significant moderators (Additional file 1: Table S2).
GRADE Assessment
Using the GRADE Assessment, all outcomes ranged from “low” to “high” certainty of evidence (Additional file 1: Figure S7). VO2peak for the overall pooled effects, as well as the sensitivity analysis for TTE in healthy participants consuming BRJ, were both downgraded to “moderate” certainty because of a potentially influential study and risk of publication bias. Sensitivity analysis on the outcome of VO2peak in healthy participants consuming BRJ was downgraded to “low” because of both a potentially influential study and because two studies (of five total) with the largest effect were not described as double-blinded.
Discussion
Overall model
The use of inorganic NO3− supplementation to improve physical function and exercise performance has increased over the last decade. To date, data demonstrating the benefits of acute and short-term NO3− supplementation on exercise performance are equivocal, but the consensus is that NO3− likely confers an overall small beneficial effect in individuals with low to moderate fitness. A summary of these data can be found in several meta-analyses and a recent expert consensus [15, 37,38,39,40]. Given that most athletes and clinical populations engaged in NO3− supplementation are likely involved in chronic exercise training/rehabilitation to improve function/performance, it is important to examine the outcomes from exercise training and NO3− supplementation in combination compared with training alone.
The results of this meta-analysis suggest that the addition of NO3− supplementation to exercise training does not enhance VO2peak or TTE beyond normal exercise training responses (Figs. 2 and 3, respectively), although it is important to note the limited number of studies and small sample sizes associated with studies in this area. As visualized in the sunset funnel plot (Additional file 1: Figure S4), existing studies are not sufficiently powered to detect the trivial-small effect observed in this meta-analysis. Further, while the present data suggest trivial improvements in VO2peak, these data are heavily influenced by a trial that was potentially single-blinded [31]. Removal of this study further weakened the effects of NO3− supplementation. The limited existing data suggest that any improvement in VO2peak and TTE observed after NO3− supplementation were likely trivial, and that more studies with longer training durations and with larger sample sizes are needed.
Subgroup Data
It has been hypothesized that NO3− supplementation may produce greater benefits in hypoxic or low oxygen conditions [41], as well as in individuals with lower VO2peak at baseline [42] who may have greater capacity to improve, in clinical populations with inhibited endogenous NO production via endothelial nitric oxide synthase (eNOS) [43], and in biological males (although this may be partly due to a lack of studies in females) [37]. Furthermore, evidence suggests that NO3− may be most effective when delivered in more moderate doses (both absolute mmol and mmol/kg) [44,45,46], and when delivered in the form of beetroot juice rather than another form such as a nitrate salt [47, 48]. Accordingly, we sought a priori to determine the potential influence of these variables on the exercise training responses to NO3− via a subgroup moderation. These results showed that there were no statistically significant moderators (Tables 2, 3, and 4).
General Discussion
While these moderator variables have been proposed to predict acute exercise responses to NO3− supplementation, it is possible that these acute changes are not large enough to result in an accumulated fitness benefit over time. Additionally, each moderator variable has considerations that may have impacted the lack of significant findings. For example, one moderator variable was baseline VO2peak, as those who are less aerobically fit initially have a lower VO2peak and may be more likely to have limitations in their baseline endogenous production of NO [49, 50]. Theoretically, these individuals will have greater responses to training and to NO3− supplementation, but this was not the case. For example, the study with the highest improvement in VO2peak following NO3− supplementation compared to control (∆ 5.5 vs. 3.0 ml/kg/min, respectively), was also the group with the highest baseline fitness (~ 60 mL/kg/min) [31], whereas the study group that experienced the largest difference in TTE following NO3− supplementation compared to control (∆ -2 vs. -95 s, respectively), had the second highest baseline fitness (~ 56 mL/kg/min) [33]. Further, the VO2peak improvements were low in the clinical populations, averaging only 0.55 ml/kg/min across all conditions, although this may be due to the more moderate exercise intensity used in these studies compared to the healthy population studies which all employed high intensity or sprint interval training [51].
While data have also suggested that moderate absolute doses of NO3− have generally shown similar benefits to larger doses in exercise responses [45], there is increasing scientific interest in the effects of NO3− dose normalized relative to body mass [44, 52]. Because of this, a moderator analysis was performed for dose of NO3− expressed both as mmol/day as well as mmol/kg/day, but neither were shown to be significant predictors of outcomes (Table 5). Finally, biological sex has also been proposed as a factor impacting the beneficial effects of NO3−, suggesting a potential lack of impact in females compared to males [37, 53, 54], although there is a paucity of data examining the impact of NO3− in females. Indeed, none of the studies involved in this meta-analysis assessed only females, and those that included both sexes [32, 34,35,36] did not explore sex-differences in responses. Whether NO3– dose should be normalized to bodyweight has key implications in females due to the typically lower body mass compared to males and higher basal NO2− levels [55]. As there appears to be a possible hormesis response to NO3− supplementation in which an optimal dose outperforms a low or a high dose [46], it seems plausible that females are at risk of exceeding an optimal dose of NO3− if given the same absolute dose shown to benefit males. Thus, the normalization of the dose of NO3− to bodyweight, especially in females, merits further exploration.
Despite the lack of significant moderators, a trend was seen in improvement of VO2peak in the BRJ subgroup (p = 0.10; Table 3). This was perhaps due to the presence of biologically active polyphenols, antioxidants, etc. that are found in BRJ [56] that may facilitate conversion of NO2− to NO [57,58,59,60]. Indeed, BRJ has been shown to improve plasma NO3−, submaximal VO2, and TTE all to a greater extent than equimolar sodium nitrate [47, 48]. While not reaching statistical significance, this meta-analysis suggests that BRJ may offer greater physiological outcomes than other forms of NO3− for improving the responses to exercise training. Further, trials included in this meta-analysis (all of which used BRJ) that included participants with clinical conditions had varying severity of disease (hypertension, peripheral arterial disease, and heart failure). These trials reported poor fitness improvements in the training interventions (NO3−: 0.75 ml/kg/min vs. placebo: 0.93 ml/kg/min average improvements; data not shown). While this was potentially due to the maladaptive and continually worsening pathology of some of these diseases, inclusion of these clinical populations in the meta-analysis may have weakened an overall training effect of the combined interventions. This prompted an additional sensitivity analysis in which a meta-analysis was performed on only studies using BRJ in healthy participants. This analysis revealed a stronger trend for improvement with BRJ supplementation in VO2peak (p = 0.08; Additional file 1: Figure S5) compared with TTE (p = 0.19; Additional file 1: Figure S6). Further subgroup and meta-regression analysis revealed that there were no significant moderators (Additional file 1: Tables S1 and S2). While this subgroup involved only 5 trials (total n = 103), 1 of which was identified as being potentially influential (Fig. 2), this finding may suggest that NO3− when administered in the form of BRJ could potentially improve exercise training responses to VO2peak in healthy participants. While these data are underpowered as they stand, and any potential improvements in VO2peak appear to be small, this suggests that additional research is needed to determine if BRJ supplementation may serve as an ergogenic aid in healthy individuals. While many collegiate and professional athletes are taking supplemental NO3− (often via BRJ) in hopes of performance enhancement, existing data suggest these recommendations may be speculative and premature in nature.
Why chronic NO3− supplementation does not appear to clearly improve exercise training benefits despite acute benefits on exercise is unknown. It appears plausible that improvements of each acute exercise bout throughout a training intervention would accumulate into a greater improvement in responses. VO2peak is improved with exercise training by factors such as increases in stroke volume, arterio-venous oxygen extraction, and oxygen carrying capacity. Given the shorter duration of training in many of these studies, many training-induced improvements in VO2peak are attributed to improvements in blood volume and the associated improvement in venous return and stroke volume [61, 62]. To our knowledge, there are no studies examining the effects of NO3− supplementation on blood volume in humans. It is also possible that exercise training outcomes were not improved in this analysis because the adaptations induced by exercise training alone far exceed enhancements seen by simply supplementing with NO3−. Ultimately, more studies are needed to address these gaps in knowledge.
Limitations
A major limitation of this meta-analysis is the low number of trials (n = 11) and the small sample sizes of trials included (average n = 20 per trial, 10 per group). The authors feel that this is important to point out as it highlights the need for more and larger studies addressing the ability of NO3− supplementation to augment exercise training responses. This also applies to the subgroup analyses performed in this meta-analysis, as the subgroups will have less statistical power than the entire model. Of the 9 studies, 11 total trials were included in the meta-analysis as two of the studies had multiple study populations as well as a placebo group (BRJ and potassium nitrate (KNO3) [35]; heart failure and hypertension [32]). We recognize that including multiple trials from one study may contribute to analytical issues such as “double counting.” Because the placebo groups were the only groups with trials used twice, and these groups experienced expected training responses, this appears unlikely to have impacted the outcomes. Further, the NO3− normalized to bodyweight data for each trial was calculated based on absolute values of NO3− supplemented and mean bodyweight for the study. Although this is meant for exploratory purposes, caution should be warranted interpreting these data as they present risk of error due to the method of calculation. This meta-analysis was not pre-registered, although all outcomes and subgroup analyses were determined a priori.
Additionally, the inclusion criteria included a minimum of 3 weeks of exercise training with an average training time of 5 weeks (only 1 study beyond 6 weeks [36]). This relatively short duration is less likely to induce large changes in VO2peak [63, 64] and thus may not be sufficient to provide an accurate representation of potential differences between treatments. On average, VO2peak improved 4.0% and 6.4% for placebo and NO3− supplemented groups after exercise training, respectively. It is possible that larger improvements as well as larger disparities between supplemented groups would be seen with longer supplementation and training time. Despite this, duration of training intervention was not a statistically significant moderator for any outcomes. The lack of additional exercise measures that are known to impact performance, such as lactate threshold, is another limitation to the results. However, large inconsistencies between studies (i.e., lactate samples taken during submaximal vs maximal workloads) did not allow for accurate analyses of these data. Additionally, NO3− combined with exercise training may have an impact on measures of cardiovascular health which was not explored in this meta-analysis.
Finally, a limitation not of this meta-analysis, but rather of the trials themselves, is that the majority of the studies that observed exercise training with NO3− supplementation also provided an acute dose of NO3− prior to post-training testing [31,32,33,34,35]. This makes it impossible to determine whether any differences in training responses stemmed from the chronic training alongside NO3−, or whether the acute effects of NO3− were simply the cause of any observed differences. Indeed, subgroup analysis showed this to be a significant moderator in the BRJ and healthy subset of data (Additional file 1: Table S1), and studies which included acute supplementation overall showed a general trend for greater improvements. Future studies in this field should abstain from an acute NO3− dose prior to post-testing to determine a true training difference.
Conclusions
The results of this systematic review and meta-analysis suggest that, based on the limited data available, NO3− supplementation in addition to exercise training does not appear to improve VO2peak or time to exhaustion above and beyond that of exercise training alone. Additionally, there were no statistically significant moderators observed (i.e., sex, health status, training oxygenation, route of NO3− administration, baseline VO2peak, age, bodyweight, or NO3− dose). A subset of studies revealed a trend for improvement in VO2peak beyond exercise alone (p = 0.08) in healthy participants using BRJ as the mode of NO3− administration, although these improvements were greatly impacted by a trial that was deemed influential and concerning in terms of bias. Ultimately, more studies with longer training duration, larger sample sizes, and the addition of examining sex as a biological variable are needed to determine whether NO3− supplementation can improve exercise training responses, regarding VO2peak and TTE, compared to exercise training alone. Because of this, caution is warranted for individuals supplementing with NO3− in hopes of greater exercise training responses as the current data suggest trivial and non-significant improvements in these outcomes.
Availability of Data and Materials
Available upon reasonable request.
Abbreviations
- VO2peak :
-
Volume of oxygen uptake during peak exercise
- NO3 − :
-
Nitrate
- NO2 − :
-
Nitrite
- NO:
-
Nitric oxide
- TTE:
-
Time to exhaustion
- SMD:
-
Standardized mean difference
- CI:
-
Confidence interval
- O2 :
-
Oxygen
- PO2 :
-
Partial pressure of oxygen
- a-vO2 :
-
Arterial-venous oxygen
- RCT:
-
Randomized controlled trial
- kg:
-
Kilogram
- ß:
-
Regression coefficient
- RoB:
-
Risk of bias
- eNOS:
-
Endothelial nitric oxide synthase
- KNO3 :
-
Potassium nitrate
- BRJ:
-
Beetroot juice
References
Kocha CD, Gladwina MT, Freeman BA, et al. Enterosalivary nitrate metabolism and the microbiome: intersection of microbial metabolism, nitric oxide and diet in cardiac and pulmonary vascular health. Free Radic Biol Med. 2017;105:48–67. https://doi.org/10.1016/j.freeradbiomed.2016.12.015.
Woessner M, Smoliga JM, Tarzia B, et al. A stepwise reduction in plasma and salivary nitrite with increasing strengths of mouthwash following a dietary nitrate load. Nitric Oxide Biol Chem. 2016;54:1–7. https://doi.org/10.1016/j.niox.2016.01.002.
OrtizdeZevallos J, Woessner MN, Kelley EE. Skeletal muscle as a reservoir for nitrate and nitrite: the role of xanthine oxidase reductase (XOR). Nitric Oxide. 2022. https://doi.org/10.1016/j.niox.2022.10.004.
Richards JC, Racine ML, Hearon CM, et al. Acute ingestion of dietary nitrate increases muscle blood flow via local vasodilation during handgrip exercise in young adults. Physiol Rep. 2018;6:1–12. https://doi.org/10.14814/phy2.13572.
Kruse NT, Ueda K, Hughes WE, et al. Eight weeks of nitrate supplementation improves blood flow and reduces the exaggerated pressor response during forearm exercise in peripheral artery disease. Am J Physiol Heart Circu Physiol. 2018;315:H101–8. https://doi.org/10.1152/ajpheart.00015.2018.
Ferguson SK, Hirai DM, Copp SW, et al. Impact of dietary nitrate supplementation via beetroot juice on exercising muscle vascular control in rats. J Physiol. 2013;591:547–57. https://doi.org/10.1113/jphysiol.2012.243121.
Coggan AR, Leibowitz JL, Kadkhodayan A, et al. Effect of acute dietary nitrate intake on maximal knee extensor speed and power in healthy men and women. Nitric Oxide. 2015;48:16–21. https://doi.org/10.1016/j.gde.2016.03.011.
Coggan AR, Leibowitz JL, Spearie CA, et al. Acute dietary nitrate intake improves muscle contractile function in patients with heart failure: a double-blind, placebo-controlled, randomized trial. Circ Heart Fail. 2015;8:914–20. https://doi.org/10.1161/CIRCHEARTFAILURE.115.002141.
Larsen FJ, Weitzberg E, Lundberg JO, et al. Effects of dietary nitrate on oxygen cost during exercise. Acta Physiol. 2007;191:59–66. https://doi.org/10.1111/j.1748-1716.2007.01713.x.
Vanhatalo A, Bailey SJ, Blackwell JR, et al. Acute and chronic effects of dietary nitrate supplementation on blood pressure and the physiological responses to moderate-intensity and incremental exercise. Am J Physiol Regul Integr Comp Physiol. 2010;299:R1121–31. https://doi.org/10.1152/ajpregu.00206.2010.
Lansley KE, Winyard PG, Fulford J, et al. Dietary nitrate supplementation reduces the O2 cost of walking and running: a placebo-controlled study. J Appl Physiol. 2011;110:591–600. https://doi.org/10.1152/japplphysiol.01070.2010.
Larsen FJ, Schiffer TA, Borniquel S, et al. Dietary inorganic nitrate improves mitochondrial efficiency in humans. Cell Metab. 2011;13:149–59. https://doi.org/10.1016/j.cmet.2011.01.004.
Jones L, Bailey SJ, Rowland SN, et al. The effect of nitrate-rich beetroot juice on markers of exercise-induced muscle damage: a systematic review and meta-analysis of human intervention trials. J Diet Suppl. 2021. https://doi.org/10.1080/19390211.2021.1939472.
Shannon OM, Grisotto G, Babateen A, et al. Knowledge and beliefs about dietary inorganic nitrate among UK-based nutrition professionals: development and application of the KINDS online questionnaire. BMJ Open. 2019;9:e030719. https://doi.org/10.1136/bmjopen-2019-030719.
Shannon OM, Allen JD, Bescos R, et al. Dietary inorganic nitrate as an ergogenic aid: an expert consensus derived via the modified delphi technique. Sports Med. 2022. https://doi.org/10.1007/s40279-022-01701-3.
Mitchell JH, Sproule BJ, Chapman CB. The physiological meaning of the maximal oxygen intake test. J Clin Investig. 1958;37:538–47.
Snell PG, Stray-Gundersen J, Levine BD, et al. Maximal oxygen uptake as a parametric measure of cardiorespiratory capacity. Med Sci Sports Exerc. 2007;39:103–7.
Mandsager K, Harb S, Cremer P, et al. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. 2018;1:e183605. https://doi.org/10.1001/jamanetworkopen.2018.3605.
Coyle EF, Coggan AR, Hopper MK, et al. Determinants of endurance in well-trained cyclists. J Appl Physiol. 1988;64:2622–30. https://doi.org/10.1152/jappl.1988.64.6.2622.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Higgins JPT, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928–d5928. https://doi.org/10.1136/bmj.d5928.
Kossmeier M, Tran US, Voracek M. metaviz: forest plots, funnel plots, and visual funnel plot inference for meta-analysis. R Package Version 0.3. 0. 2020;
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Soft. 2010. https://doi.org/10.18637/jss.v036.i03.
Cohen J. Statistical power analysis for the behavioural sciences. London: Routledge; 1988.
Viechtbauer W, Cheung MWL. Outlier and influence diagnostics for meta-analysis. Res Synth Method. 2010;1:112–25. https://doi.org/10.1002/jrsm.11.
Higgins JPT. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. https://doi.org/10.1136/bmj.327.7414.557.
Kossmeier M, Tran US, Voracek M. Power-enhanced funnel plots for meta-analysis: the sunset funnel plot. Zeitschrift für Psychologie. 2020;228:43–9. https://doi.org/10.1027/2151-2604/a000392.
De Smet S, Van Thienen R, Deldicque L, et al. Nitrate intake promotes shift in muscle fiber type composition during sprint interval training in hypoxia. Front Physiol. 2016. https://doi.org/10.3389/fphys.2016.00233.
Finkel A, Röhrich MA, Maassen N, et al. Long-term effects of NO3– on the relationship between oxygen uptake and power after three weeks of supplemented HIHVT. J Appl Physiol. 2018;125:1997–2007. https://doi.org/10.1152/japplphysiol.00176.2018.
Muggeridge DJ, Sculthorpe N, James PE, et al. The effects of dietary nitrate supplementation on the adaptations to sprint interval training in previously untrained males. J Sci Med Sport. 2017;20:92–7. https://doi.org/10.1016/j.jsams.2016.04.014.
Puype J, Ramaekers M, Van Thienen R, et al. No effect of dietary nitrate supplementation on endurance training in hypoxia: nitrate intake and hypoxic training. Scand J Med Sci Sports. 2015;25:234–41. https://doi.org/10.1111/sms.12199.
Shaltout HA, Eggebeen J, Marsh AP, et al. Effects of supervised exercise and dietary nitrate in older adults with controlled hypertension and/or heart failure with preserved ejection fraction. Nitric Oxide. 2017;69:78–90.
Sousa A, Viana JL, Milheiro J, et al. Dietary nitrate supplementation is not helpful for endurance performance at simulated altitude even when combined with intermittent normobaric hypoxic training. Front Physiol. 2022;13:839996. https://doi.org/10.3389/fphys.2022.839996.
Thompson C, Wylie LJ, Blackwell JR, et al. Influence of dietary nitrate supplementation on physiological and muscle metabolic adaptations to sprint interval training. J Appl Physiol. 2017;122:642–52. https://doi.org/10.1152/japplphysiol.00909.2016.
Thompson C, Vanhatalo A, Kadach S, et al. Discrete physiological effects of beetroot juice and potassium nitrate supplementation following 4-wk sprint interval training. J Appl Physiol. 2018;124:1519–28. https://doi.org/10.1152/japplphysiol.00047.2018.
Woessner MN, Vanbruggen MD, Pieper CF, et al. Beet the best? Dietary inorganic nitrate to augment exercise training in lower extremity peripheral artery disease with intermittent claudication. Circ Res. 2018;123:654–9. https://doi.org/10.1016/j.physbeh.2017.03.040.
Senefeld JW, Wiggins CC, Regimbal RJ, et al. Ergogenic effect of nitrate supplementation: a systematic review and meta-analysis. Med Sci Sports Exerc. 2020;52:2250–61. https://doi.org/10.1249/MSS.0000000000002363.
Bahrami LS, Arabi SM, Feizy Z, et al. The effect of beetroot inorganic nitrate supplementation on cardiovascular risk factors: a systematic review and meta-regression of randomized controlled trials. Nitric Oxide. 2021;115:8–22. https://doi.org/10.1016/j.niox.2021.06.002.
McMahon NF, Leveritt MD, Pavey TG. The effect of dietary nitrate supplementation on endurance exercise performance in healthy adults: a systematic review and meta-analysis. Sports Med. 2017;47:735–56. https://doi.org/10.1007/s40279-016-0617-7.
Gao C, Gupta S, Adli T, et al. The effects of dietary nitrate supplementation on endurance exercise performance and cardiorespiratory measures in healthy adults: a systematic review and meta-analysis. J Int Soc Sports Nutr. 2021;18:55. https://doi.org/10.1186/s12970-021-00450-4.
Shannon OM, McGawley K, Nybäck L, et al. “Beet-ing” the mountain: a review of the physiological and performance effects of dietary nitrate supplementation at simulated and terrestrial altitude. Sports Med. 2017;47:2155–69. https://doi.org/10.1007/s40279-017-0744-9.
Porcelli S, Ramaglia M, Bellistri G, et al. Aerobic fitness affects the exercise performance responses to nitrate supplementation. Med Sci Sports Exerc. 2015;47:1643–51. https://doi.org/10.1249/MSS.0000000000000577.
Woessner MN, McIlvenna LC, Ortiz de Zevallos J, et al. Dietary nitrate supplementation in cardiovascular health: an ergogenic aid or exercise therapeutic? Am J Physiol Heart Circ Physiol. 2018;314:H195–212. https://doi.org/10.1152/ajpheart.00414.2017.
Pekas EJ, Wooden TK, Yadav SK, et al. Body mass-normalized moderate dose of dietary nitrate intake improves endothelial function and walking capacity in patients with peripheral artery disease. Am J Physiol Regul Integr Comp Physiol. 2021. https://doi.org/10.1152/ajpregu.00121.2021.
Wylie LJ, Kelly J, Bailey SJ, et al. Beetroot juice and exercise: pharmacodynamic and dose–response relationships. J Appl Physiol. 2013;115:325–36. https://doi.org/10.1152/japplphysiol.00372.2013.
Gallardo EJ, Gray DA, Hoffman RL, et al. Dose-response effect of dietary nitrate on muscle contractility and blood pressure in older subjects: a pilot study. J Gerontol Ser A. 2021;76:591–8. https://doi.org/10.1093/gerona/glaa311.
Behrens CE, Khandaker J, Karina A, et al. Acute beetroot juice supplementation improves exercise tolerance and cycling efficiency in adults with obesity. Physiol Rep. 2020;8:1–12. https://doi.org/10.14814/phy2.14574.
Flueck JL, Bogdanova A, Mettler S, et al. Is beetroot juice more effective than sodium nitrate? The effects of equimolar nitrate dosages of nitrate-rich beetroot juice and sodium nitrate on oxygen consumption during exercise. Appl Physiol Nutr Metab. 2016;41:421–9. https://doi.org/10.1139/apnm-2015-0458.
Tsukiyama Y, Ito T, Nagaoka K, et al. Effects of exercise training on nitric oxide, blood pressure and antioxidant enzymes. J Clin Biochem Nutr. 2017;60:180–6. https://doi.org/10.3164/jcbn.16-108.
Poveda JJ, Riestra A, Salas E, et al. Contribution of nitric oxide to exercise-induced changes in healthy volunteers: effects of acute exercise and long-term physical training. Eur J Clin Investig. 1997;27:967–71. https://doi.org/10.1046/j.1365-2362.1997.2220763.x.
Angadi SS, Mookadam F, Lee CD, et al. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: a pilot study. J Appl Physiol. 2015;119:753–8. https://doi.org/10.1152/japplphysiol.00518.2014.
Larsen FJ, Schiffer TA, Ekblom B, et al. Dietary nitrate reduces resting metabolic rate: a randomized, crossover study in humans. Am J Clin Nutr. 2014;99:843–50. https://doi.org/10.3945/ajcn.113.079491.
Wickham KA, McCarthy DG, Pereira JM, et al. No effect of beetroot juice supplementation on exercise economy and performance in recreationally active females despite increased torque production. Physiol Rep. 2019;7:1–14. https://doi.org/10.14814/phy2.13982.
Kapil V, Rathod KS, Khambata RS, et al. Sex differences in the nitrate-nitrite-NO • pathway: role of oral nitrate-reducing bacteria. Free Radic Biol Med. 2018;126:113–21. https://doi.org/10.1016/j.freeradbiomed.2018.07.010.
Kapil V, Milsom AB, Okorie M, et al. Inorganic nitrate supplementation lowers blood pressure in humans: role for nitrite-derived no. Hypertension. 2010;56:274–81. https://doi.org/10.1161/HYPERTENSIONAHA.110.153536.
Wootton-Beard PC, Ryan L. A beetroot juice shot is a significant and convenient source of bioaccessible antioxidants. J Funct Foods. 2011;3:329–34. https://doi.org/10.1016/j.jff.2011.05.007.
Rocha BS, Gago B, Barbosa RM, et al. Dietary polyphenols generate nitric oxide from nitrite in the stomach and induce smooth muscle relaxation. Toxicology. 2009;265:41–8. https://doi.org/10.1016/j.tox.2009.09.008.
Peri L, Pietraforte D, Scorza G, et al. Apples increase nitric oxide production by human saliva at the acidic pH of the stomach: a new biological function for polyphenols with a catechol group? Free Radic Biol Med. 2005;39:668–81. https://doi.org/10.1016/j.freeradbiomed.2005.04.021.
Carlsson S, Wiklund NP, Engstrand L, et al. Effects of pH, nitrite, and ascorbic acid on nonenzymatic nitric oxide generation and bacterial growth in urine. Nitric Oxide. 2001;5:580–6. https://doi.org/10.1006/niox.2001.0371.
Tanaka K, Hayatsu T, Negishi T, et al. Inhibition of N-nitrosation of secondary amines in vitro by tea extracts and catechins. Mutat Res Genet Toxicol Environ Mutagen. 1998;412:91–8. https://doi.org/10.1016/S1383-5718(97)00178-2.
Hellsten Y, Nyberg M. Cardiovascular adaptations to exercise training. Compr Physiol. 2016;6:1–32. https://doi.org/10.1002/cphy.c140080.
Hopper MK, Coggan AR, Coyle EF. Exercise stroke volume relative to plasma-volume expansion. J Appl Physiol. 1988;64:404–8. https://doi.org/10.1152/jappl.1988.64.1.404.
Weltman A, Seip RL, Snead D, et al. Exercise training at and above the lactate threshold in previously untrained women. Int J Sports Med. 1992;13:257–63. https://doi.org/10.1055/s-2007-1021263.
Hickson RC, Bomze HA, Holloszy JO. Linear increase in aerobic power induced by a strenuous program of endurance exercise. J Appl Physiol. 1977;42:372–6. https://doi.org/10.1152/jappl.1977.42.3.372.
Acknowledgements
Not applicable.
Funding
No sources of funding were used to assist in the preparation of this article.
Author information
Authors and Affiliations
Contributions
ACH conceptualized the study. ACH, JOZ, and KCA screened the studies and completed the risk of bias. ACH and JOZ extracted data. ACH, KCA, and CP performed statistical analysis. ACH, KCA, JOZ, CP, AW, and JDA designed the study and reviewed and revised the initial and final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Figure S1: Risk of Bias Assessment. [32a] Heart failure trial. [32b] Hypertension trial. [35a] Beetroot juice trial. [35b] Potassium nitrate trial. Figure S2: Funnel Plot for VO2peak as an outcome. Figure S3: Funnel Plot for Time to Exhaustion (TTE) as an outcome. Figure S4: The Sunset Funnel Plot. Figure S5: Sensitivity Analysis - Forest Plot of VO2peak with inclusion only of studies which observed healthy participants and with beetroot juice supplementations as the administration route of NO3−. [32a] Heart failure trial. [32b] Hypertension trial. [35a] Beetroot juice trial. [35b] Potassium nitrate trial. Table S1: Subgroup Analysis for VO2peak and Time to Exhaustion (TTE) in Studies Using Beetroot Juice (BRJ) in Healthy Subjects. Figure S6: Sensitivity Analysis - Forest Plot of Time to Exhaustion (TTE) with inclusion only of studies which observed healthy participants and with beetroot juice (BRJ) supplementations as the administration route of NO3−. [32a] Heart failure trial. [32b] Hypertension trial. [35a] BRJ trial. [35b] Potassium nitrate trial. Table S2: Meta-Regression Analysis for VO2peak and Time to Exhaustion (TTE) in Studies Using Beetroot Juice (BRJ) in Healthy Subjects. Figure S7: GRADE Assessment of included trials.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hogwood, A.C., Anderson, K.C., Ortiz de Zevallos, J. et al. Limited Effects of Inorganic Nitrate Supplementation on Exercise Training Responses: A Systematic Review and Meta-analysis. Sports Med - Open 9, 84 (2023). https://doi.org/10.1186/s40798-023-00632-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-023-00632-1