
Abstract
Background
Childhood Polyarteritis nodosa (PAN) is a systemic vasculitis with necrotizing inflammation of medium- and small-sized arteries. Disease evolution may be severe and refractory to standard treatment including prednisone, azathioprine and cyclophosphamide.
Case presentation
We present the case of a young girl with severe PAN resulting in progressive ischemia and necrosis of fingers and toes. Biological work-up revealed increased acute phase reactants and interleukin-6 levels. She was only partially controlled despite high-dose corticosteroids and cyclophosphamide infusions, and eventually achieved rapid improvement and sustained remission on tocilizumab.
Further, we review the current evidence of the interleukin-6-inhibitor tocilizumab for the treatment of PAN.
Conclusion
Tocilizumab may be an efficient therapeutic option in a subset of treatment-refractory children with PAN.
Similar content being viewed by others


Background
Polyarteritis nodosa (PAN) is a rare systemic vasculitis with necrotizing inflammation of medium or small sized arteries that may start in childhood [1]. The presentation and clinical course can be variable and range from relatively benign to severe systemic forms affecting multiple organs. In childhood, PAN relapse rates have been described up to 50%, therefore morbidity and mortality are non-negligible [2, 3]. Treatment recommendations include high-dose corticosteroids and cyclophosphamide for severe disease; however, their long-term use may be associated with unfavourable adverse events, especially in children. In recent years, biological agents including TNF-inhibitors (infliximab, adalimumab) and rituximab have been used for refractory cases [4, 5]. Here, we describe the use of tocilizumab (TCZ), an interleukin-6 (IL-6) receptor inhibitor, in a little girl with severe, refractory, necrotizing PAN. Informed parental consent was obtained for the publication of the case and the images.
Case presentation
A previously healthy 4-year-old girl of North African origin developed fever, polyarthralgia, swelling of her hands and feet, palpable nodules in legs, cyanosis and progressive ischemia of the second to fifth right fingers and the second right toe. There was no family history of immunodeficiency, autoimmune or vascular disease. She initially presented at a local hospital in North Algeria where a skin biopsy from a leg nodule was performed showing a vasculitis of the medium-sized vessels suggestive of polyarteritis nodosa. Therapy with high dose prednisone at 4 mg/kg/day, three immunoglobulin infusions at 5 g/kg and methotrexate at 0.2 mg/kg/week was initiated without improvement. The authors do unfortunately not have more information about the rationale for choosing these high doses of prednisone and immunoglobulin infusions. Disease course and treatment regimens are shown in Fig. 1.

Clinical course and treatment regimens. AZA = Azathioprine. Cyclophos = Cyclophosphamide. IVIG = intravenous immunoglobuline. mPSL pulse = Methylprednisolone pulse. MTX = Methotrexate. Prdn = Prednisone. TCZ = Tocilizumab
Three months later parents sought a second opinion in Spain due to worsening disease. At initial presentation the girl was well and afebrile, blood pressure was 98/72 mmHg. She had cutaneous necrosis of the distal phalanx of the second to fifth fingers of the right hand and the second toe of the right foot, palpable nodules in lower limbs without livedo reticularis and myalgia. Pulmonary, abdominal, ear-nose-throat and neurologic exams were normal, there was no evidence of neuropathy.
Laboratory investigations showed elevated acute phase reactants (C-reactive protein 100 mg/l (normal < 5 mg/l), erythrocyte sedimentation rate 120 mm/h, and increased pro-inflammatory cytokines (IL-6 106.43 pg/ml (normal 0–4.3 pg/ml), IL-10 9.62 pg/ml (normal 0–7.8 pg/ml), TNF-alpha 10.7 pg/ml (normal 4–8 pg/ml), measured by ELISA). Creatine kinase was within normal limits, as were liver transaminases. Hepatitis B serology showed immunity through vaccination. The autoimmune workup was negative including anti-phospholipid antibodies.
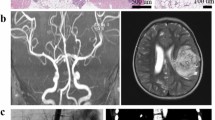
Broad microbiologic cultures were negative and no anti-tissue specific antibodies were found. A primary immunodeficiency panel of 323 genes (including CECR1 for ADA2 deficiency) did not find any pathogenic mutation. Positron emission tomography scan revealed muscular, synovial and diffuse bone involvement, with hyperfixation also of lymph nodes and subcutaneous nodules. A second skin biopsy was performed from the sole of foot and compatible with PAN (Fig. 2). Muscle biopsy was normal.

Histology from skin biopsy. Skin biopsy from a nodule on the foot sole. Histology (hematoxylin eosin staining, × 10 magnification) demonstrated inflammation of a small artery with an inflammatory infiltrate of predominantly lymphocytes with neutrophils. No granulomas were seen
Intravenous corticosteroids were initiated at 1 mg/kg/day for 8 days, but disease activity persisted and the patient was given methylprednisolone 30 mg/kg/day on three consecutive days. However, disease was still not controlled and cutaneous necrosis required amputation of the 2nd to 5th finger of the right hand (Fig. 3). Cyclophosphamide at 500 mg/m2 dose and subsequently azathioprine at 1 mg/kg/day were started due to worsening peripheral oedema, subcutaneous nodules and painful livedo. Despite of treatment escalation and low-dose aspirin, new ischemic signs appeared on the 5th finger of the left hand for which intravenous infusion of alprostadil at 9.6 ng/kg/minute that was maintained for 5 days, a second dose of cyclophosphamide and another bolus of methylprednisolone 30 mg/kg were given. Given the partial response, persistent biologic inflammation and high serum of IL-6 levels, TCZ (8 mg/kg every 2 weeks) was added with clinical and biological improvement within few days. Azathioprine was continued and Prednisone slowly tapered. Six months after TCZ initiation, after increasing the TCZ infusion interval to 3-weekly, she developed panniculitis; TCZ infusion was again administered in 2-weekly intervals while Azathioprine was continued, and panniculitis improved. After the child had moved to France in complete remission and 12 months after treatment initiation, TCZ infusions interval was increased to every 3 weeks and azathioprine discontinued. Prednisone was discontinued after 14 months. At last follow-up, 21 months after treatment initiation, complete clinical and biologic remission persists on 3-weekly TCZ infusions and low-dose aspirin. Serum IL-6 level remained elevated (43.3 pg/ml, normal 0.0–8.5). Serum ADA2 activity was normal. Thoracic and abdominal CT angiography showed no abnormalities.

Ischemia of the extremities. A, B Cutaneous necrosis of the distal phalanx of the right hand and the second right toe prior to surgery. C-E Vasculitic lesions of the feet and left hand. F Right hand, 21 months after treatment initiation
Discussion and conclusions
We hereby report rapid improvement and sustained remission following TCZ therapy in a little girl with severe, treatment-refractory PAN. TCZ was favoured over a TNF-blocker due to high acute phase reactants (indicating increased inflammation) and markedly elevated IL-6 levels (relatively higher compared to TNF-alpha level elevation). Indeed, TNF-inhibitors may be the primary choice in patients in which ADA2 deficiency cannot rapidly be excluded as was the case in our patient by negative genetic testing and normal serum ADA2 activity; TNF-inhibitors have been successfully used in children with PAN and ADA2 deficiency [6, 7].
TCZ was well tolerated without serious adverse events during the 18 months follow-up period. Prior to TCZ, the patient had received high-dose corticosteroids, cyclophosphamide and azathioprine; therefore, a cumulative beneficial effect of these medications cannot be excluded. However, we believe that TCZ was responsible for the clinical and biological improvement observed in the patient because disease activity worsened despite treatment escalation, there was a marked and fast improvement after TCZ initiation and the patient has maintained a sustained clinical remission with exception of a mild disease flare when TCZ dose interval was temporarily increased.
To date, eleven patients (median age 35 years, IQR 23.5–57.5; 5 female) with PAN treated with TCZ mostly for refractory disease have been reported in the literature [8,9,10,11,12,13]; amongst these, two children (Table 1). Watanabe et al. published the case of a 3-year-old boy presenting with fever, periostitis, epididymo-orchitis, arthritis and myositis, who improved clinically, biologically and radiologically on TCZ and cyclophosphamide after having failed IVIG, corticosteroids and infliximab [9]. Inoue et al. reported an 8-year-old girl with cutaneous PAN resistant to multiple treatment lines including corticosteroids, azathioprine and TNF-inhibitors, who eventually achieved remission on TCZ [8]. In adults, TCZ has been successfully used in eight treatment-refractory cases [10,11,12,13,14] and in one patient as first-line therapy in combination with corticosteroids [10]. Our patient received intravenous tocilizumab at a dose of 8 mg/kg every 2 weeks in analogy with the dose used by Inoue an colleagues [8]. Moreover, this lower dose was chosen due to an increased risk for potentially severe infections associated with the therapy, as tocilizumab was initiated only a few days after digital amputation. Later the dose was maintained as clinical and biologic response to tocilizumab was rapid and excellent. Various dosing regimens and administration routes (subcutaneous and intravenous) have been used in the literature, and the optimal dosing regimen still needs to be determined.
Whilst mutations in CECR1 are associated with monogenic PAN in some patients, the etiopathology of classic PAN is not well known [15, 16]. However, both the innate and adaptive immune systems seem to be involved [17]. Our and others clinical observations suggest a role of the pro-inflammatory cytokine IL-6 in the pathophysiology but very few studies have investigated this hypothesis [18,19,20,21]. Increased IL-6 levels have been associated with disease activity in some case reports [18, 20, 21], where IL-6 levels normalized with response to treatment (prednisone, cyclophosphamide, tacrolimus). In addition, Kawakami and colleagues retrospectively evaluated 45 patients with cutaneous PAN [19]. Those with elevated IL-6 levels (n = 19) were more commonly males, had significantly more arthralgia and skin ulcerations, higher CRP serum levels and higher prevalence of antiphospholipid antibodies compared to those with normal IL-6 levels (n = 26). However, none of these patients was treated with an IL-6 inhibitor and repeated IL-6 serum levels were not available [19].
In conclusion, our observation and the published literature suggests that TCZ may represent an effective therapeutic option in a subset of patients with recalcitrant PAN. However, many questions remain to be answered, in particular with the exact pathophysiological role of IL-6 in PAN which has yet to be elucidated, also how to determine which patients will respond to IL-6 blockade, and whether it should be considered as second-line treatment for refractory patients or as first-line therapy.
Availability of data and materials
Not applicable.
Abbreviations
- ADA2:
-
Adenosine Deaminase 2
- CECR1:
-
Cat Eye Chromosome Region 1
- IL:
-
Interleukin
- PAN:
-
Polyarteritis nodosa
- TCZ:
-
Tocilizumab
- TNF:
-
Tumor necrosis factor
References
Ozen S, Pistorio A, Iusan SM, Bakkaloglu A, Herlin T, Brik R, et al. EULAR/PRINTO/PRES criteria for Henoch-Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II: final classification criteria. Ann Rheum Dis. 2010;69(5):798–806. https://doi.org/10.1136/ard.2009.116657.
Eleftheriou D, Dillon MJ, Tullus K, Marks SD, Pilkington CA, Roebuck DJ, et al. Systemic polyarteritis nodosa in the young: a single-center experience over thirty-two years. Arthritis Rheum. 2013;65(9):2476–85. https://doi.org/10.1002/art.38024.
Merlin E, Mouy R, Pereira B, Mouthon L, Bourmaud A, Piette JC, et al. Long-term outcome of children with pediatric-onset cutaneous and visceral polyarteritis nodosa. Joint Bone Spine. 2015;82(4):251–7. https://doi.org/10.1016/j.jbspin.2015.01.007.
Eleftheriou D, Melo M, Marks SD, Tullus K, Sills J, Cleary G, et al. Biologic therapy in primary systemic vasculitis of the young. Rheumatology (Oxford). 2009;48(8):978–86. https://doi.org/10.1093/rheumatology/kep148.
Campanilho-Marques R, Ramos F, Canhão H, Fonseca JE. Remission induced by infliximab in a childhood polyarteritis nodosa refractory to conventional immunosuppression and rituximab. Joint Bone Spine. 2014;81(3):277–8. https://doi.org/10.1016/j.jbspin.2013.11.009.
Ombrello AK, Qin J, Hoffmann PM, Kumar P, Stone D, Jones A, et al. Treatment strategies for deficiency of adenosine deaminase 2. N Engl J Med. 2019;380(16):1582–4. https://doi.org/10.1056/NEJMc1801927.
Kasap Cuceoglu M, Sener S, Batu ED, Kaya Akca U, Demir S, Sag E, et al. Systematic review of childhood-onset polyarteritis nodosa and DADA2. Semin Arthritis Rheum. 2021;51(3):559–64. https://doi.org/10.1016/j.semarthrit.2021.04.009.
Inoue N, Shimizu M, Mizuta M, Yachie A. Successful treatment of tumor necrosis factor inhibitor-resistant cutaneous polyarteritis nodosa with tocilizumab. Pediatr Int. 2020;62(6):753–5. https://doi.org/10.1111/ped.14184.
Watanabe K, Rajderkar DA, Modica RF. A case of Polyarteritis Nodosa associated with vertebral artery Vasculitis treated successfully with tocilizumab and cyclophosphamide. Case Rep Pediatr. 2016;2016:7987081–10. https://doi.org/10.1155/2016/7987081.
Krusche M, Ruffer N, Schneider U, Meyer M, Burmester G, Kötter I. Tocilizumab treatment for polyarteritis nodosa. Rheumatology (Oxford). 2020;59(10):e63–e5. https://doi.org/10.1093/rheumatology/keaa079.
Saunier A, Issa N, Vandenhende MA, Morlat P, Doutre MS, Bonnet F. Treatment of polyarteritis nodosa with tocilizumab: a new therapeutic approach? RMD Open. 2017;3(1):e000446. https://doi.org/10.1136/rmdopen-2017-000446.
Hočevar A, Lestan B, Šemrl SS, Lakota K, Kojc N, Potočnik N, et al. AA amyloidosis in a polyarteritis nodosa patient treated with tocilizumab. Amyloid. 2013;20(4):275–6. https://doi.org/10.3109/13506129.2013.838947.
Bodoki L, Végh E, Szekanecz Z, Szűcs G. Tocilizumab treatment in Polyarteritis Nodosa. Isr Med Assoc J. 2019;21(8):560–2.
Krusche M, Ruffer N, Kötter I. Tocilizumab treatment in refractory polyarteritis nodosa: a case report and review of the literature. Rheumatol Int. 2019;39(2):337–44. https://doi.org/10.1007/s00296-018-4210-2.
Navon Elkan P, Pierce SB, Segel R, Walsh T, Barash J, Padeh S, et al. Mutant adenosine deaminase 2 in a polyarteritis nodosa vasculopathy. N Engl J Med. 2014;370(10):921–31. https://doi.org/10.1056/NEJMoa1307362.
Zhou Q, Yang D, Ombrello AK, Zavialov AV, Toro C, Stone DL, et al. Early-onset stroke and vasculopathy associated with mutations in ADA2. N Engl J Med. 2014;370(10):911–20. https://doi.org/10.1056/NEJMoa1307361.
Ozen S. The changing face of polyarteritis nodosa and necrotizing vasculitis. Nat Rev Rheumatol. 2017;13(6):381–6. https://doi.org/10.1038/nrrheum.2017.68.
Nakahama H, Okada M, Miyazaki M, Imai N, Yokokawa T, Kubori S. Distinct responses of interleukin-6 and other laboratory parameters to treatment in a patient with polyarteritis nodosa--a case report. Angiology. 1992;43(6):512–6. https://doi.org/10.1177/000331979204300610.
Kawakami T, Takeuchi S, Soma Y. Serum levels of interleukin-6 in patients with cutaneous polyarteritis nodosa. Acta Derm Venereol. 2012;92(3):322–3. https://doi.org/10.2340/00015555-1228.
Hirohata S, Tanimoto K, Ito K. Elevation of cerebrospinal fluid interleukin-6 activity in patients with vasculitides and central nervous system involvement. Clin Immunol Immunopathol. 1993;66(3):225–9. https://doi.org/10.1006/clin.1993.1029.
Horai Y, Tokuyama A, Sumiyoshi R, Nakashima Y, Suzuki T, Okada A, et al. A case of cutaneous polyarteritis nodosa with elevated serum interleukin-6 levels complicated by leg arterial stenosis and destructive arthropathy of the left ankle. Mod Rheumatol. 2014;24(1):206–11. https://doi.org/10.3109/14397595.2013.852840.
Acknowledgements
We thank the patient and her family for participating in this study.
Funding
There is no funding to this Case Report.
Author information
Authors and Affiliations
Contributions
All authors participated in clinical care. MB and FAA wrote the case report. MLB, PQ, LBA and ACD reviewed it for important intellectual content. All authors read and approved the final version to be published.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The family gave their consent to the treatment, which was approved by the ethics committee of our institutions.
Consent for publication
Consent for publication was obtained from the family.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Boistault, M., Lopez Corbeto, M., Quartier, P. et al. A young girl with severe polyarteritis nodosa successfully treated with tocilizumab: a case report. Pediatr Rheumatol 19, 168 (2021). https://doi.org/10.1186/s12969-021-00654-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12969-021-00654-7