
Abstract
Background
Traditional medical practices have been used to maintain animal health for millennia and have been passed down orally from generation to generation. In Ethiopia also, plants are the primary means by which the indigenous people in remote areas treat the illnesses of their animals. The present study was therefore, carried out to document the type and distribution of medicinal plants of the county.
Methods
To collect ethnobotanical information, a total of 205 informants (133 men and 72 women) were selected. Among these 121 traditional medicine practitioners, while the remaining 84 were selected through a systematic random sampling method. Ethnobotanical data were collected between January 2023 and August 2023 through semi-structured interviews, participant observation, guided filed walks and focus group discussions. Using descriptive statistics, the ethnobotanical data were analyzed for the Informant Consensus Factor (ICF) and Fidelity Level (FL) values, preference, and direct matrix rankings. SPSS 26.0 and PAST 4.11 software were used in data analysis.
Results
Totally, 78 ethnoveterinary medicinal plants distributed in 36 families were identified in the study area. Asteraceae was the dominant family with 9 species (14%), followed by Euphorbiaceae with 8 species (12%). Herbs 42(56%), wild collected 62 (66%), and leaf part (52%) made the highest share of the plant species. Hordeum vulgare L. had the highest fidelity level (FL = 98%) for treating bone fractures. Blackleg, bloat, and endoparsistes each had the highest values of the consensus factor among the informants (ICF = 1). According to preference ranking, Withania somnifera was the most potent remedy for treating blackleg. Knowledge of medicinal plants was shared through storytelling within families.
Conclusion
In the study area, there is broad access to traditional medicinal plants that can treat ailments in animals. Conservation efforts should be prioritized to protect medicinal plants from threats such as agricultural expansion, drought, and development. Further research should be conducted to explore the potential of different medicinal plants for treating common livestock ailments.
Similar content being viewed by others


Background
Livestock production is vital to developing nations' rural economies, especially in rural communities [1]. Food security and poverty reduction are two benefits it provides, along with support for many cultural rituals [2]. Animals fulfill a number of social roles and are a major source of food, money, and nutrient-rich dung that may rebuild soil [3, 4]. However, their likelihood of catching other diseases is usually higher. Diseases that affect livestock raising to differing degrees may put different kinds of animals at risk [5,6,7]. Ethnoveterinary medicine (EVM) is the application of a range of belief-based systems and knowledge, conventional wisdom, experience, techniques, knowledge of medicinal plants, technologies, and teaching to the care of livestock in order to maintain animal health [8]. However, public veterinary services are only available in large cities and some selected area in terms of economic importance [9]. So, for farmers and livestock herders in remote locations, EVM provides a viable replacement for western veterinary procedures. According to McGaw and Eloff et al. [10], plants contain a variety of phytochemicals and investigations in EVM are necessary. Wendimu et al. [11] claimed these plants can be the leading candidates for the creation of medications and other active items that are useful for controlling human and livestock health ailments. As a nation, Ethiopia continues to rely heavily on traditional medicine, and medicinal herbs in particular, to address problems with livestock health [11, 12]. Given that the country is listed in two biodiversity hotspots and has a rapid population growth and the continued loss of biodiversity highlights the necessity of researching plant resources, especially local species that are considered endemic or indigenous [13, 14].
Despite some efforts [12, 15,16,17,18,19], the lack of documenting and dissemination of scientific data on the use of ethnoveterinary medicine among various ethnic groups worldwide represents a crucial gap in the body of material currently available. The majority of diagnostic and treatment expertise has historically been passed down orally and through mentoring; written records have been used sparingly [20,21,22]. The research and documentation of traditional ethnoveterinary medicine need to be prioritized more and more, as there is a possibility that indigenous knowledge levels could be lost due to many circumstances, including urbanization, migration, and technology [11, 23,24,25,26,27]. The importance of this corpus of information is best expressed by the African saying "When an erudite old man dies, the whole library disappears" [28].
People in the Omo-Gibe and Rift Valley Basins in southern Ethiopia's Wolaita Zone use traditional diagnostic techniques and plant-based treatments to treat livestock ailments. This research investigated ethnoveterinary practices in this region, focusing on traditional diagnostic tools and plant-based treatments for livestock disease, with the goal of preserving indigenous knowledge and improving animal health.
Materials and methods
Description of the study area
Wolaita is the name of one of Ethiopia's zonal administrations. The Wolaita people, whose ancestral home is in the zone, gave it their name. Wolaita is bordered by Gamo Gofa on the south, the Omo River on the west, which separates it from Dawro, Kembata, Tembaro on the northwest, Hadiya on the north, the Oromia Region on the northeast, the Bilate River on the east, which separates it from Sidama Region, and Lake Abaya on the south-east, which separates it from Oromia Region. Sodo serves as the administrative hub of Wolaita. Wolaita Zone is located in one of Ethiopia's Southern Regional states. With a surface area of 4383.7 km2, the zone has a population above 5.3 million [29].
The study was carried out in four districts, such as Damot Sore District and Sodo Zuria District in Omo-Gibe Basin Side and Diguna Fango District and Abala Abaya District in Rift Valley Basin Side of Wolaita Zone (Fig. 1). The maximum monthly temperatures are 17.7°C in July and 22.1°C in February and March. The average annual temperature is 19.9°C [30,31,32]. The region receives an average of 1,350 mm (53 in) of rainfall annually, according to Bagnara [30].

The study area map, Wolaita Zone, Cluster 1, South Ethiopia Regional State (Source: AcrMap10.4.1 by Abenezer Wendimu)
Study design
In a cross-sectional study approach was used to collect ethnoveterinary information from traditional healers in the Wolaita zone between January 2023 and August 2023. The primary study parameters were indigenous ethnobotanical knowledge, resources, and their applications.
Sampling procedure and informant selection
The key informants were chosen by using purposive sampling method. Following the discovery of a few practioners/healers utilizing the sources mentioned above, fruitful initial interactions were made and further ethnopractitioners were found using their existing networks. This method is frequently employed in indigenous knowledge studies to gather data from unexplored communities that are challenging for academics to reach. With the help of the purposive sample technique, it was ensured that only the key respondents with the necessary traits and levels of understanding of the traditional animal healthcare system were selected [32]. Two Hundred Five (205) individuals were chosen to take part in the study, with 65% of them being men and 35% being women while the remaining 84 were selected through a systematic random sampling method. Participants included were farmers, livestock, herders, and individuals with indigenous knowledge, and their ages ranged from 18 to 95. From the total population, 121 were key informants. The selection method for the study's target or key respondents was depending on the target individual's background experience in contemporary ethnoveterinary medical practices. Ethnopractitioners who give the local livestock vital medical care were designated as the target or key respondents.
Data collection
From Damot Sore District, in Rift Valley Basin side, the kebeles (wards; small administrative unit of the district) used to conduct the research were Dege Shekise, Gunino 01, Gunino Hamus, and Sheyemiba kebeles while in Sodo Zuria District, Damot Waja, Waja Kero, Wareza Shoho, and Wareza Gerera kebeles. In Rift Valley Basin side, Abela Longena, Abela Mareqa and Abela Gurcho were kebeles selected from Abala Abaya District and Dimtu Town, Bitena Town and Edo Boloso were kebeles selected from Diguna Fango District.
An open interview questions was created for data collection and given to the participants. The interview was split into two segments. Basic data, including the respondent's name, age, gender, place of birth, and level of education, were gathered in the first section. Different items made up the open interview in the second section including the names of plants, a list of ailments/diseases treated with the claimed MPs, plant parts utilized, mode of preparation, plant habitat, source of information acquisition, etc. The interviewees were requested to go with us to the neighboring mountains, farms, or grasslands to identify the medicinal plants they used and to offer local colloquial names in Wolaita dialect, in addition to written records and audio recordings, which were taken with another party's permission. Individual interview data were cross-checked with additional participants' commentaries from the same villages in order to gather trustworthy information about the study region [33].
Questionnaire distribution
The interviewer assisted each of the respondents in completing a well-structured questionnaire (S1 Appendix). The survey consisted of 18 questions covering: village, respondent's information, approval, ethnoveterinary medicine details, animal species treated, remedy identification, care, compensation, knowledge exchange, livestock illnesses treated, plants used, plant state, plant variables, plant actions, challenges, respondent's views, recommendations, and direct observation by the interviewer.
The interviewer was required to be accompanied by a senior relative or friend, as well as a member of the local government from the office of the area subchief who was acquainted with the interviewee, whenever a questionnaire was delivered to the subject. As the interviewer completed the questionnaire, these two individuals actively and productively engaged the interviewee in conversation. This combination produced a highly beneficial interaction that created a favorable setting for the successful completion of research using Rapid Rural Appraisal (RRA) and Participatory Rural Appraisal (PRA). Because it lessened the following causes of bias, this technique was deemed to be very effective and reliable:—(1) modeling bias, or projecting the interviewer's viewpoint onto the subjects under study, (2) strategic bias, or the subject's expectation of benefits, (3) relationships between senior relatives, administrator representatives, and interviewees that are familiar with one another may lead to rote responses and outsider bias while lessening resistance to questioning and (4), decreasing the influence of "key personas" [25]. Due to these preconceived notions, questionnaires would be filled out incorrectly and the data collected would not be properly documented or analyzed [12, 15].
Plant specimen collection and identification
After the key respondents were personally interviewed, the indicated specimens of plants were identified and collected during numerous field trips. The specimens were collected, and each plant species was verified using The World Flora Online [34] and The Plant List [35] before botanical identification was completed in a field laboratory using biological keys. They were photographed and sampled for identification at the National Herbarium of Ethiopia. Formal identification of the plant materials were carried out by Abenezer Wendimu (the first author) and Zekarias Demisseie (a botanist) assisted the identification.
Data analysis
The collected data on medicinal plants, their uses, and related knowledge were recorded and coded on Microsoft Excel. Descriptive statistics like percentages and frequency tables were employed to analyze the data using SPSS version 20.Remarks about the medical worth of plants, their growing forms, modes of preparation, how they are used, routes of adminstration, dose, and what components of the plants they are made of were all part of the interview session. Using the t-test at a 95% confidence level, it was enabled to us to compare the traditional medical dynamics about the use of plants for medicinal purposes by men and women, young and old, illiterate and educated, key and general informants.
According to Chekole et al. [36], quantitative ethnobotanical methods like Informant Consus Factor (ICF) values were calculated to determine the most common livestock illnesses categories reported across the communities and to identify potentially effective medicinal plant species in respective disease categories.
where; nur (category's total number of citations) was calculated by subtracting the total number of species utilized (nt) and dividing the result by the total number of citations in each category, minus one.
Furthermore, Fidelity Level (FL) values were computed as follows: FL (%) = Ip/Iu × 100. Where Iu stands for all informants who indicated using a plant to treat any sickness, while Ip indicates how many respondents overall suggested utilizing a plant to treat a particular condition. Preference ranking was developed to determine the effectiveness of particular medicinal plants against the most prevalent diseases in the research district.
Results
Diversity of ethnoveterinary medicinal plants in the district
The research districts contained 78 different species of ethnoveterinary medicinal plants, which are belongs into 36 families (Table 1). Asteraceae was a dominant family with 9(14%) species followed by Euphorbiaceae 8(12%), Solanaceae 6(9%), and Cucurbitaceae 3(5%) (Fig. 2).

Frequency of the 32 plant families used in the treatment of livestock diseases
Collection habitat and growth pattern of medicinal plants.
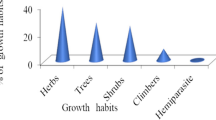
A total of 54 medicinal plants were identified, of which 62(66%) were collected from the wild, 24(26%) were grown in private gardens, and the remaining plant species 8(8%) was gathered from both agricultural and uncultivated wilderness areas. In terms of growth patterns, herbs made up 42(56%) of the higher plant species and were the most frequently gathered to treat livestock diseases, followed by shrubs 24(31%) and trees 10(12%) (Fig. 3).

Medicinal Plants Growth habit
Use knowledge of medicinal plants among people
Despite the fact that male informants reported 133(65%) more medicinal plants than female respondents 72(35%), the difference was statistically insignificant (p > 0.05). Similar to this, there were reported medicinal plant differences between the community unable to read and write 64(80%) and educated groups 41(20%) that were statistically significant (p < 0.05). Compared to general informants, key informants knew a considerably (p < 0.05) a greater number of therapeutic plants (Table 2).
Acquiring and sharing the knowledge of native medicinal plants
From a total of 205 practitioners, 179 (87%) said they had heard stories about medicinal plants from members of their family, especially their father and grandparents, in a very private way. The remaining 15 (7%) and 11 (6%) picked up knowledge of medicinal plants from reading various sources, and trial-and-error, respectively.
Distribution of medicinal plants
The land use and land cover (LULC) data of the study area comprises more than 10 different flora distribution classes (Fig. 4, upper). The habitat of the medicinal plants in the whole Wolaita can be divided into three parts in terms altitude—lowlands (Lowland < 1500 m.a.s.l; near and around villages, collection time within a day, collection areas easily accessible) and highlands (Highland > 2300 m.a.s.l; far from villages, collection takes more than a day, collection areas remote and hard to access) and midland (Midland 1500–2300 m.a.s.l) small villages near the district towns, collection takes not more than a day, collection areas near and accessible) (Fig. 4, lower). Out of the reported species, 29 species are found in the lowlands and 18 species were found in the highlands with 31 species common in lowlands and highlands (Fig. 5). Generally, collection of highland medicinal plants is difficult and hence storage of such species for further use is common practice in the study area.

Land use – Land cover and digital elevation model (DEM) of Wolaita Zone (Source: AcrMap10.4.1 by Abenezer Wendimu)

Distribution of medicinal plants in terms of altitude
The distribution of medicinal plants in terms of major drainage basins in Wolaita revealed that, Omo-Gibe basin holds about 32% of total collection of medicinal plants where as 20% were collected from Rift Valley basin. A significant amount of medicinal plants overlap were recorded from the two basins with 48% of collections common to both basins (Fig. 6).

Distribution of medicinal plants in terms of drainage basins
Aspects of animal disease in the study area
This study found 55 different forms of animal illnesses. Highest number of species (16) were prescribed to treat blackleg followed by 10 species to bloat, 8 Trypanosomosis, and 7 each in colic and leech infestation (Table 3). Practitioners noted that they might utilize one or several medicinal plant species to treat a certain type of sickness. Endoparasite infestation, blackleg, and colic were the most common types of diseases treated by 9 medicinal plant species. In the Wolaita zone, the therapeutic indication of medicinal plant-based medicines included all livestock species. Medicinal plant cures were most frequently prescribed for Bovine ailments 93(49%), followed by Caprine 46(24%), Ovine 42(22%), Equine 3(2%), Galline 3(2%), and Feline 1(1%) aliments (Fig. 7).

Animals treated by traditional medical preparations in the study area
Parts of the medicinal plants utilized in the concoction of herbal remedies
In the study area, leaves 55(52%) were the most often employed plant components in the preparation of remedies, followed by root 18(17%), seed 14(13%), and stems 10(9%). The remaining fruit, sap and whole parts of the plants contributed for 2% and 1% of the remedy preparation were prepared from bulb, flower and latex (Fig. 8). Regarding the state of the plant parts, freshly harvested plant parts dominated (80%), with the remaining 20% being used in both freshly and in a dried form.

Plant parts used for preparation of the remedies
The routes of remedy administration
The target animal and the type of sickness determined how to administer ethnobotanical preparations. In the study area, the most common modes of administration were nasal, oral, topically/dermally, and intraocularly, and others include applying the medication directly to a fresh lesion or cut. Oral 73(69%) and nasal 11(10%) routes were the most frequently used delivery methods followed by dermal 8(7%) and topical 7(7%) administration routes. Ethnomedicines applied via the ophthalmic and ocular modes of administration routes were the least cited routes (Fig. 9).

The administration routes of ethnobotanical preparations
Informant consensus factor
Blackleg, bloat, and endoparsistes each had the highest values of the consensus factor among the informants, which were followed by trypanosomiasis (0.8) and colic (0.79) (Fig. 10). Leech and rabies took the next two spots (0.75 each).

Livestock ailments in the study district along with the Consensus Factor of Informants (ICF)
Fidelity level
Hordeum vulgare L. had the highest fidelity level (FL = 98%) for treating bone fractures followed by Acalypha spp. for treating bloat (FL = 92%) (Table 2).
Preference ranking
According to data collected from six key informants, Withania somnifera was the most potent remedy for treating blackleg. Tragisa spp. and Kalanchoe spp. were the next most efficient therapeutic plants. Ocimum lamiifolium and Prunus africana were, in comparison, the least effective plants for medicinal purposes, according to the data gathered from six key informants (Table 4).
Medicinal plant threats in the area
Both natural factors (such as drought and landslides) and anthropogenic factors (firewood, overgrazing, agricultural expansion, construction, and medicinal use) have an impact on the survival of medicinal plants in the study district. The main dangers to medicinal plants in the study district were the expansion of agriculture, followed by drought and development (Fig. 11).

Medicinal plants conservation threats in the study area
Discussion
Livestock is essential to the livelihoods of the inhabitants of the study districts for a variety of reasons, including crop production, draft power, marketing, and revenue generating. Despite the fact that knowledge differed depending on the age and sex group, this causes the residents of the district to have the knowledge to defend their animals from a variety of illnesses using therapeutic plants. There were just 64.87% of women respondents in this survey, whereas there were 35.12% men. The elders may pass on their knowledge to their older son or to their preferred son rather than their daughter, which could be the cause of this. A different Ethiopian region has also observed similar results [37, 38]. The reason behind this preference for passing on knowledge to a male heir rather than a female one may be rooted in traditional gender roles and societal norms. In many cultures, especially patriarchal ones, sons are often seen as the ones who will carry on the family legacy and continue the family line, while daughters are expected to marry into another family. Additionally, there may be a belief that certain types of knowledge are better suited for men to carry on, such as medicinal or magical practices that require physical strength or are traditionally performed by men. It is important to note that these beliefs are based on outdated gender stereotypes and should not be used to justify discrimination against female family members. Even though, on average, males used slightly more medicinal herbs than women, the differences were not that much big and statistically insignificant (p = 0.53). Other factors may be influencing the higher usage of medicinal herbs among males, but further research is needed to determine these factor.. This finding was consistent with the conclusions reached by Yigezu et al. [39]. The study also revealed that older groups of informants reported a considerably larger average number of therapeutic plants than the youngest group (p < 0.05). The main factors to this notable disparity are the growth of modern medicine and the younger age groups' disinterest in traditional medications. There could be other factors at play, such as differences in cultural upbringing, access to traditional medicine, or differing beliefs about the effectiveness of traditional remedies.
In addition, the youthful group lacks interest due to the seasonal scarcity of therapeutic plants and their hard harvesting. As a result, a decline in positive attitudes toward traditional medicine is a sign that knowledge of these practices and the species of medicinal plants is eroding. The research by Yigezu et al. [39] and Lulekal et al. [40] got the same results. In accordance, significantly (p < 0.05) more medicinal plants were reported by illiterate respondents than by educated respondents. This is because respondents who were educated preferred modern treatment and paid less attention to traditional medicine. In turn, this leads to a decline in medical expertise in the following generation. By Birhan et al. [8], the same conclusion was reported. Key informants could report significantly more medicinal plants than general informants (p < 0.05) as a result of their experience.
The identification and documentation of 78 ethnoveterinary medicinal plant species, including their scientific and local names, habits, methods of preparation, and used components, was included in the present study. The dominant families were Euphorbiaceae and Asteraceae. Ethiopia's Amhara region, according to Lulekal et al. [40], likewise exhibited a predominance of the Asteraceae family. However, the family Solanaceae has been found in various regions of Ethiopia [11, 18, 41, 42], which goes against this study. The district is home to a diverse population, according to this result. Furthermore, the preference for native and endemic plants with therapeutic properties shows that people don't have contemporary knowledge but rather has a lengthy history and is handed down from one generation to the next over an extended period of time. This finding was consistent with studies by Mengesha [43] and Lulekal et al. [40].
The bulk of plant growth forms investigated for medicinal purposes were herbs; shrubs came in second, and trees and climbers next in sequential order of species. In a different region of Ethiopia, a high consumption of shrubs for their therapeutic benefits was noted [18, 41, 44]. This can occur as a result of the relatively abundant herb availability for practitioners in the study districts. According to other findings [37, 45, 46], shrubs predominate.
The majority of the plants in this study—32 (61.5%)—were gathered from the wild, while 11 (25%) were taken from backyard gardens, and the remaining 7 (13.5%) species were found in both backyard and wild habitats. The results of other authors [18, 40, 44, 46] were consistent with this finding. This indicates that growing plants in a home garden for therapeutic reasons is quite uncommon in the research area. This decreased practice of growing medicinal plants in backyard gardens results in a lack of those plants throughout the year as desired by practitioners.
Many medicinally important plant species were reported to be found in the mid-altitudinal ranges (1500–2300 m.a.s.l) for the ollection areas were near and accessible. This is in line with Kunwar and Bussmann [47] who reported an increase of medicinal plant species with increasing altitude up to about 2000 m.a.s.l. The medicinal plant diversity corresponds with total richness of plant diversity [48], however, the high value species were reported from the highland areas.
Although different plant parts have been used to treat various illnesses, leaves and seeds were the two plant parts most frequently used in the study district. This result is consistent with research conducted by Tekle [49] in the southern Ethiopian Amaro special district, the western Ethiopia Horro Gudurru district [18], and the eastern Harerghe Melkabello district [41]. It disagrees, however, with studies done by Jima and Megersa [50] in the Berbere District of Oromia region and by Seid [44] in the Amhara region's Enarj Enawega District's east Gojjam Zone [8]. The persistence of plants in their native environment is not significantly impacted using leaves for medication. However, the use of roots for medicinal purposes could result in the extinction of certain species from their natural habitats as well as the native plant medicine expertise is being lost. The majority of practitioners in the research district like plants in fresh 60 (80%) circumstances. The results of Chekole et al. [51] are consistent with this finding. The harvesting of fresh plant material used by practitioners to make medicines during the dry season may cause the plants' species to be stripped.
Oral form of administration accounted for 62 (74%) of all administrations, followed by nasal mode of administration (13%) and cutaneous mode of administration (8%). This result was consistent with that of Yigezu et al. [39]. There is no standard unit of measuring for plant remedies in the study district; instead, people use their own system of measurement. The medication dosage is based on the age, breed, and size of the animals that are receiving treatment. Other authors reported the same results [42, 52,53,54,55,56].
Blackleg (0.82), general sickness (0.8), and pasteurellosis (0.79), according to informants' consensus factors (ICF), had the highest values. Blackleg received the highest plant citation at the time, 10(30.3%), followed by general disease 7(21.21%). This makes it very evident that blackleg is a widespread and well-known illness in the studied area. There are 10 ethnoveterinary medicinal herbs that can be used to treat this condition. Vernonia amygdalina was the most popular medicinal plant species for treating blackleg, followed by Cucumis ficifolius and Solanecio gigas. According to Mengesha and Dessie [53] and Tadesse et al. [54], different districts used the same ethnoveterinary medicinal herbs that were identified in the research districts to treat blackleg.
In general, the research area has a high biodiversity, and the locals have a wealth of conventional knowledge concerning the use of herbal remedies to treat certain livestock diseases. A variety of indigenous plant species can be found in the study region. The findings of this investigation demonstrated that the district's expertise and therapeutic plants are vulnerable. Therefore, it necessitates special consideration from the public, the government, and all stakeholders.
The cultural interpretation of medicinal plants and diseases in the Wolaita region offers a fascinating glimpse into the rich heritage and traditional knowledge of the local community. For generations, the people of Wolaita have developed a profound understanding of the medicinal properties of various plants, which they have used to treat and manage a wide range of diseases and ailments. The traditional healers, known as "hiillaa," play a significant role in preserving this knowledge and administering remedies derived from the region's diverse flora. These healers possess an intimate understanding of both the physical and spiritual aspects of healing, often incorporating rituals, prayers, and incantations into their practices. In the study area, specific diseases are attributed to spiritual or supernatural causes, leading to the use of specific plants and rituals aimed at appeasing or combatting these metaphysical influences. The cultural interpretation of medicinal plants and diseases in Wolaita intertwines the deep-rooted beliefs, values, and practices of the local population, showcasing their respect for nature and their reliance on traditional wisdom passed down through generations.
Limitation of the study
The study was conducted in small portions of the Omo-Gibe and Rift Valley basins in Ethiopia, which may not fully represent the entire ethnobotanical use of plants in treating livestock ailments of these basins. Future studies should aim to include a more comprehensive assessment of the ethnobotanical use of plants in these basins to provide a more holistic understanding of medicinal plant species diversity, use, distribution, and abundance in the area.
Conclusions
The communities that were chosen are mainly rural in character, and livestock farmers are looking into the local biodiversity and indigenous knowledge systems to satisfy the demands of animal health and productivity. In the study region, 78 ethnoveterinary species of medicinal plants from 28 distinct families were discovered. The Euphorbiaceae and Asteraceae plant families made up the majority of those that were noted. Herbs were the most frequently collected to cure livestock sickness and made up higher plant species in terms of growth patterns. Most of the plants were collected from the wild. According to practitioners, they would use one or several therapeutic plant species depending on the disease. Nine different species of medicinal plants were used to cure the most frequent ailments, including colic, blackleg, and endoparasite infestation. Bovine ailments were most frequently treated using medicinal plant remedies. The plant's fresh leaves were the plant parts that were most frequently used to make medicines. The most popular remedy administrative methods in the study area included the nose, mouth, skin, eyes, and others, including applying the drug directly to a fresh lesion or cut. Blackleg, bloat, and endoparsistes had the highest values of the consensus factor among the informants, according to the data. According to data collected from six important informants, Withania somnifera was the most potent remedy for treating blackleg. The primary threats to botanical medicine in the study region were the expansion of agriculture, followed by drought and development. Despite the fact that the research region in the districts of the Wolaita Zone was proven to be rich in a variety of medicinal plants, there are currently few attempts being made to look at the native knowledge and plants associated with them. To prevent such losses, communities at large along with accountable organizations must protect therapeutic plants. It's also important to choose plants for further study that have a high potential based on the relevant ethnobotanical indices, such as phytochemical analysis and pharmacological and toxicological investigations. In general, the research area has a high biodiversity, and the locals have a wealth of conventional knowledge concerning the use of herbal remedies to treat certain livestock diseases. A variety of indigenous plant species can be found in the study region. The findings of this investigation demonstrated that the district's expertise and therapeutic plants are vulnerable. Therefore, it necessitates special consideration from the public, the government, and all stakeholders.
Availability of data and materials
The data used to support the findings of this study are included within the supplementary information file(s).
References
Varijakshapanicker P, Mckune S, Miller L, Hendrickx S, Balehegn M, Dahl GE, Adesogan AT. Sustainable livestock systems to improve human health, nutrition, and economic status. Anim Front. 2019;9:39–50. https://doi.org/10.1093/af/vfz041.
Chakale MV, Mwanza M, Aremu AO. Ethnoveterinary knowledge and biological evaluation of plants used for mitigating livestock diseases: a critical insight into the trends and patterns in South Africa. Front Vet Sci. 2021;891:710884. https://doi.org/10.3389/fvets.2021.710884.
Mottet A, Teillard F, Boettcher P, De’Besi G, Besbes B. Domestic herbivores and food security: current contribution, trends and challenges for a sustainable development. Animal. 2018;12:s188–98. https://doi.org/10.1017/s1751731118002215.
Banda LJ, Tanganyika J. Livestock provide more than food in smallholder production systems of developing countries. Anim Front. 2021;11:7–14. https://doi.org/10.1093/af/vfab001.
van Jaarsveld BDL, Pieters BDH, Potgieter EDB, vanWyk GDN, Pfitzer KDS, Trümpelmann LD, et al. Monthly Report on Livestock Disease Trends as Informally Reported by Veterinarians Belonging to the Ruminant Veterinary Association of South Africa (RuVASA), a Group of the South African Veterinary Association; Ruminant Veterinary Association of South Africa: Pretoria, South Africa, 2017; p. 28.
Maikhuri R. Eco-energetic analysis of animal husbandry in traditional societies of India. Energy. 1992;17:959–67. https://doi.org/10.1016/0360-5442(92)90045-2.
Dovie DB, Shackleton CM, Witkowski E. Valuation of communal area livestock benefits, rural livelihoods and related policy issues. Land Use Policy. 2006;23:260–71. https://doi.org/10.1016/j.landusepol.2004.08.004.
Birhan YS, Kitaw SL, Alemayehu YA, Mengesha NM. Ethnoveterinary medicinal plants and practices in Enarj Enawga District, East Gojjam Zone, Amhara Region, Ethiopia. Int J Anim Sci. 2018;2(1):1014. https://www.jsmcentral.org/sm-animal-science/ijas-v2-1014.pdf.
Tabuti JR, Dhillion SS, Lye KA. Ethnoveterinary medicines for livestock (Bos indicus) in Bulamogi county, Uganda: plant species and mode of use. J Ethnopharmacol. 2003;88:279–86. https://doi.org/10.1016/s0378-8741(03)00265-4.
McGaw LJ, Eloff JN. Ethnoveterinary use of southern African plants and scientific evaluation of their medicinal properties. J Ethnopharmacol. 2008;119:559–74. https://doi.org/10.1016/j.jep.2008.06.013.
Wendimu A, Tekalign W, Asfaw B. A survey of traditional medicinal plants used to treat common human and livestock ailments from Diguna Fango district, Wolaita, southern Ethiopia. Nord J Bot. 2021;39(5):1–20. https://doi.org/10.1111/njb.03174.
Abraha T, Balcha A, Mirutse G. An ethnobotanical study of medicinal plants used in Kilte Awulaelo District, Tigray Region of Ethiopia. J Ethnobiol Ethnomed. 2013;9(1):1–23. https://doi.org/10.1186/1746-4269-9-65.
Hoveka LN, van der Bank M, Bezeng BS, Davies TJ. Identifying biodiversity knowledge gaps for conserving South Africa’s endemic flora. Biodivers Conserv. 2020;29:2803–19. https://doi.org/10.1007/s10531-020-01998-4.
Wall B, Mateus A, Marshall L, Pfeiffer D, Lubroth J, Ormel H, Otto P, Patriarchi A. Drivers, Dynamics and Epidemiology of Antimicrobial Resistance in Animal Production; Food and Agriculture Organization of the United Nations: Rome, Italy, 2016. http://www.fao.org/3/a-i6209e.pdf.
Elizabeth A, Hans W, Zemede A, Tesfaye A. The current status of knowledge of herbal medicine and medicinal plants in Fiche Ethiopia. J Ethnobiol Ethnomedicine. 2014;10:1–33. https://doi.org/10.1186/1746-4269-10-38.
Lynam T, De Jong W, Sheil D, Kusumanto T, Evans K. A review of tools for incorporating community knowledge, preferences, and values into decision making in natural resources management. Ecol Soc. 2007;12:5. https://doi.org/10.5751/ES-01987-120105.
Beinart W, Brown K. African Local Knowledge & Livestock Health: Diseases & Treatments in South Africa. Johannesburg, South Africa: Wits University Press; 2013.
Birhanu T, Abera D. Survey of ethno-veterinary medicinal plants at selected Horro Gudurru Districts, Western Ethiopia. African Journal of Plant Science. 2015;9(3):185–92. https://doi.org/10.5897/AJPS2014.1229.
McGaw LJ, Famuyide IM, Khunoana ET, Aremu AO. Ethnoveterinary botanical medicine in South Africa: a review of research from the last decade (2009 to 2019). J Ethnopharmacol. 2020;257:112864. https://doi.org/10.1016/j.jep.2020.112864.
Eisner H. What makes the systems engineer successful? various surveys suggest an answer; CRC Press: Boca Raton, FL. USA. 2020. https://doi.org/10.1201/9781003089650.
Bredemus BA. Consensual qualitative research analysis of prominent multicultural psychotherapy researchers’ career experiences; the chicago school of professional psychology proquest dissertations Publishing: Chicago, IL. USA. 2021. https://doi.org/10.1037/a0012051.
Bruchac M. Indigenous knowledge and traditional knowledge. Encycl Glob Archaeol. 2014;10:3814–24. https://www.jstor.org/stable/48717564.
Abebe D. Traditional medicine in Ethiopia: the attempts being made to promote it for effective and better utilization. SINET. 1986;9:61–9.
Giday M, Asfaw Z, Woldu Z. Medicinal plants of the Meinit ethnic group of Ethiopia: an ethnobotanical study. J Ethnopharmacol. 2009;124:513–21. https://doi.org/10.1016/j.jep.2009.05.009.
Asfaw Z. The role of home gardens in the production and conservation of medicinal plants. In: Proceedings of Workshop on Biodiversity Conservation and Sustainable Use of Medicinal Plants in Ethiopia. Addis Ababa: Institute of Biodiversity Conservation and Research; 2001.
Hecht S, Yang AL, Basnett BS, Padoch C, Peluso NL. People in Motion, Forests in Transition: Trends in Migration, Urbanization, and Remittances and Their Effects on Tropical Forests; CIFOR: Bogor, Indonesia, 2015;142. https://doi.org/10.17528/cifor/005762.
Crane PR, Ge S, Hong DY, Huang HW, Jiao GL, Knapp S, Kress WJ, Mooney H, Raven PH, Wen J. The Shenzhen declaration on plant sciences-uniting plant sciences and society to build a green, sustainable earth. J Syst Evol. 2017;55:59–61. https://doi.org/10.1111/jse.12283.
Lalonde A. African indigenous knowledge and its relevance to sustainable development. International program for traditional ecological knowledge, 1993, Ottawa. https://dlc.dlib.indiana.edu/dlc/bitstream/handle/10535/904/African_Indigenous_Knowledge_and_its_Relevance_to_Environment_and_Development_Activities.pdf?sequence=1.
Central Statistical Agency (CSA). Population Size by Sex, Region, Zone and Wereda: July 2021. https://www.statsethiopia.gov.et/wp-content/uploads/2020/08/Population-of-Weredas-as-of-July-2021.pdf.
Bagnara GL. Agricultural Production and Market of Wolaita Rural Area (Ethiopia). Technical Report. 2017. https://doi.org/10.13140/RG.2.2.34313.95846.
Central Statistical Agency (CSA). Tables: Southern Nations, Nationalities, and Peoples’ Region Archived 2012–11–13 at the Wayback Machine, Tables 2.1, and 3.4. 2007.
Russell B. Research methods in anthropology: qualitative and quantitative methods. 3rd ed. California: Altamira Press; 2002. ISBN-10: 0759101485 (ISBN-13: 978–0759101487).
Kongsager R. Data collection in the field: lessons from two case studies conducted in belize. Qual Rep. 2021;26:1218–32. https://doi.org/10.46743/2160-3715/2021.4744.
The World Flora Online. (http://www.worldfloraonline.org/. Accessed 1 – 9 2023.
The Plant List (http://www.theplantlist.com. Accessed 1 – 9 2023.
Chakale MV, Asong JA, Struwig M, Mwanza M, Aremu AO. Ethnoveterinary practices and ethnobotanical knowledge on plants used against livestock diseases among two communities in South Africa. Plants. 2022;11:1784. https://doi.org/10.3390/plants11131784.
Abebe M. The study of ethnoveterinary medicinal plants at Mojana Wodera district, central Ethiopia. PLoS ONE. 2022;17(5):e0267447. https://doi.org/10.1371/journal.pone.0267447.
Chekole G. Ethnobotanical study of medicinal plants used against human ailments in Gubalafto District, Northern Ethiopia. J Ethnobiol Ethnomed. 2017;13(1):1–29. https://doi.org/10.1186/s13002-017-0182-7.
Yigezu Y, Haile DB, Ayen WA. Ethnoveterinary medicine in four districts of Jimma zone, Ethiopia: cross sectional survey for plant species and mode of use. BMC Vet Res. 2014;10:76. https://doi.org/10.1186/1746-6148-10-76.
Lulekal E, Asfaw Z, Kelbessa E, Damme PV. Ethnoveterinary plants of Ankober districts, North Shewa zone, Amhara region Ethiopia. J Ethnobiol Ethnomed. 2014;10:21. https://doi.org/10.1186/1746-4269-10-21.
Mohammed C, Abera D, Woyessa M, Birhanu T. Survey of ethno-veterinary medicinal plants in Melkabello District, eastern Harerghe zone Eastern Ethiopia. Ethiopian Veter J. 2016;20(2):1–15. https://doi.org/10.4314/evj.v20i2.1.
Leul K, Gebrecherkos G, Tadesse B. Ethnobotanical study of medicinal plants in Ganta Afeshum District, Eastern Zone of Tigray, Northern Ethiopia. J Ethnobiol Ethnomed. 2018;14(1):1–19. https://doi.org/10.1186/s13002-018-0266-z.
Mengesha GG. Ethnobotanical survey of medicinal plants used in treating human and livestock health problems in Mandura Woreda of Benishangul Gumuz. Ethiopia Adv Med Plant Res. 2016;4(1):11–26. http://www.netjournals.org/pdf/AMPR/2016/1/16-005.pdf.
Seid M. Critical solutions for critical problems: Threats to sustainable use and management of Nech Sar National Park (NSNP) in Ethiopia. Afr J Hosp Tour Leis. 2019;8:1. https://doi.org/10.20546/ijcrar.701.002.
Giday M, Teklehaymanot T. Ethnobotanical study of plants used in management of livestock health problems by Afar people of Ada’ar District, Afar Regional State Ethiopia. J Ethnobiol Ethnomed. 2013;9(1):1–10. https://doi.org/10.1186/1746-4269-9-8.
Kunwar RM, Bussmann RW. Ethnobotany in the Nepal himalaya. J Ethnobiol Ethnomedicine. 2008;4:24–8. https://doi.org/10.1186/1746-4269-4-24.
Bhattarai KR, Vetaas OR. Variation in plant species richness of different life forms along a subtropical elevation gradient in the Himalayas, east Nepal. Glob Ecol Biogeogr. 2003;12:327–40. https://doi.org/10.1046/j.1466-822X.2003.00044.x.
Usmane A, Birhanu T, Redwan M, Sado E, Abera D. Survey of ethno-veterinary medicinal plants at selected districts of Harari Regional State Eastern Ethiopia. Ethiopian Veter J. 2016;20(1):1–22. https://doi.org/10.4314/evj.v20i1.1.
Tekle Y. Study on ethno veterinary practices in Amaro special district southern Ethiopia. Med Aromat Plants. 2015;4(186):2167–412. https://doi.org/10.4172/2167-0412.1000186.
Jima TT, Megersa M. Ethnobotanical study of medicinal plants used to treat human diseases in Berbere District, Bale Zone of Oromia Regional State, South East Ethiopia. Evid-Based Complement Alternat Med. 2018. https://doi.org/10.1155/2018/8602945.
Chekole G, Asfaw Z, Kelbessa E. Ethnobotanical study of medicinal plants in the environs of Taragedam and Amba remnant forests of Libo Kemkem District, northwest Ethiopia. J Ethnobiol Ethnomed. 2015;11(1):1–38. https://doi.org/10.1186/1746-4269-11-4.
Tolossa K, Debela E, Athanasiadou S, Tolera A, Ganga G, Houdijk JG. Ethno-medicinal study of plants used for treatment of human and livestock ailments by traditional healers in South Omo, Sout hern Ethiopia. J Ethnobiol Ethnomed. 2013;9(1):1–15. https://doi.org/10.1186/1746-4269-9-32.
Mengesha A, Dessie D. Ethno veterinary medicine knowledge and practices in and around Gondar, Ethiopia. Intern J Pub Health Pharm Pharmaco. 2018;3(1):39-68. https://doi.org/10.37745/ijphpp.15.
Tadesse B, Mulugeta G, Fikadu G, Sultan A, Nekemte E. Survey on ethno-veterinary medicinal plants in selected Woredas of east Wollega zone, western Ethiopia. J Biol Agriculture Healthcare. 2014;4(17):97–105. https://iiste.org/Journals/index.php/JBAH/article/view/15175.
Hammad MA, Sulaiman SAS, Aziz NA, Noor DAM. Prescribing statins among patients with type 2 diabetes: The clinical gap between the guidelines and practice. J Res Med Sci. 2019;24:15–9. https://doi.org/10.4103/jrms.JRMS_100_18.
Fennell CW, Light ME, Sparg SG, Stafford GI, Van Staden J. Assessing African medicinal plants for efficacy and safety: agricultural and storage practices. J Ethnopharmacol. 2004;95:113–21. https://doi.org/10.1016/j.jep.2004.05.025.
Acknowledgements
We would like to extend our sincere gratitude to the administrative and agricultural offices of the study districts. We also want to express our gratitude to the informants and development agents who helped us gather all data needed for the study. We are also grateful to Wolaita Sodo University for approving our request to conduct the research. There are no conflicts of interest to declare.
Funding
The study received no funding from government, commercial, or non-profit financing organizations.
Author information
Authors and Affiliations
Contributions
A.W. collected data, wrote the main manuscript text, study area mapping and formal analysis. E.B and Y.A. assisted data collection, project administration and prepared figures. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Not applicable.
Consent for publication
This manuscript doesn’t contain any person’s data, and further consent for publication isn’t required.
Competing interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wendimu, A., Bojago, E. & Abrham, Y. Medicinal ethnoveterinary plants used for treating livestock ailments in the omo-gibe and rift valley basins of Ethiopia. BMC Vet Res 20, 166 (2024). https://doi.org/10.1186/s12917-024-04019-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12917-024-04019-6