
Abstract
Objectives
The main objective of this manuscript was to identify the methods used to create process maps for care pathways that utilized the time-driven activity-based costing method.
Methods
This is a systematic mapping review. Searches were performed in the Embase, PubMed, CINAHL, Scopus, and Web of Science electronic literature databases from 2004 to September 25, 2022. The included studies reported practical cases from healthcare institutions in all medical fields as long as the time-driven activity-based costing method was employed. We used the time-driven activity-based costing method and analyzed the created process maps and a qualitative approach to identify the main fields.
Results
A total of 412 studies were retrieved, and 70 articles were included. Most of the articles are related to the fields of orthopedics and childbirth-related to hospital surgical procedures. We also identified various studies in the field of oncology and telemedicine services. The main methods for creating the process maps were direct observational practices, complemented by the involvement of multidisciplinary teams through surveys and interviews. Only 33% of the studies used hospital documents or healthcare data records to integrate with the process maps, and in 67% of the studies, the created maps were not validated by specialists.
Conclusions
The application of process mining techniques effectively automates models generated through clinical pathways. They are applied to the time-driven activity-based costing method, making the process more agile and contributing to the visualization of high degrees of variations encountered in processes, thereby making it possible to enhance and achieve continual improvements in processes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The time-driven activity-based costing (TDABC) method is a strategy for measuring costs to obtain the actual costs of a given process in healthcare [1, 2]. There are seven steps in the TDABC method [3]: (1) selecting the medical condition, (2) defining the clinical pathway, including the mapping of all key activities performed within the entire care cycle, (3) creating the clinical process maps included in each activity in the patient clinical pathway, incorporating all direct and indirect resources, (4) obtaining time estimates for each process for activities and resources used for each patient, (5) estimating the cost of using patient care resources, the cost of all direct and indirect resources involved in care delivery, (6) estimating the capacity of each resource and calculating the use cost rate and (7) calculating the total cost of patient care [3].
The TBADC method has recently expanded its use in healthcare in the past few years [2, 4, 5]. One of the main steps in applying the TDABC method consists of creating a process map describing all the activities in the analyzed clinical pathway and related resources the patient uses. Process maps assist in cost measurements by allocating resources in the analyzed clinical pathway and involving the necessary times for each process. In this context, the visualization of the involved costs becomes more tangible and can be calculated [6]. After creating the process maps, the costs of each activity are calculated to define the capacity unit value [5]. These activities can then be calculated jointly to measure the total cost of an entire service or care episode [7].
The TDABC method is considered the most precise method for measuring the costs of a specified clinical pathway due to its capability to measure the resources consumed by each patient based on two parameters: activity and time [8, 9]. It accurately provides expenditures based on process maps to navigate the steps a patient must complete throughout their care cycle [10]. In its traditional development method, the construction of clinical pathway process maps relies on conducting research and individual interviews with employees and experts in a particular field to estimate the percentage and time spent on an activity or by direct observation of the procedure [2].
The TDABC method has proven to be an effective tool for aiding administrators of healthcare initiatives based on value and performing micro-cost studies [2,3,4, 7]. The application of the method can also facilitate cost forecasting, supply information for improved management of resources and processes, and also as a basis for making future investment decisions and analyzing underused or unused capabilities in institutions [9]. A systematic review concluded that most studies on the TDABC method in healthcare institutions achieved results that contributed to cost savings. That same review also concluded that applying the TDABC method provided a truer perception to the participating members of the required resources and costs for performing each activity of the analyzed clinical pathways [11]. In addition, as TDABC relies on granular, procedure-level costs instead of broad categories, stakeholders are allowed to see what resources were used for what purposes [12].
There are even differences in the methodologies among the published studies due to the complexity of the healthcare field and the great diversity of costs and the activities present in healthcare services, which can impact cost forecasts [4]. The clinical and non-clinical teams supply information to enable the generation of process maps required for a service or procedure in the traditional TDABC method. Subsequently, the TDABC team is responsible for estimating the capacity of each resource and the necessary time based on surveys by institution professionals, who are specialists on the subject and directly observe the procedure [13]. A systematic review [3] showed the main collection methods for the TDABC method, which were derived from direct observation of procedures and interviews, meetings with the teams, or workshops. However, only one study mentioned the opportunity for creating automated process maps from the hospital data system [3]. The result from that review demonstrates the creation of process maps, even though they were prepared manually, which increases the required time for creating the process maps and the conclusion of the TDABC method.
Some systematic reviews were published on the subject [3, 11]; however, the publications still need to exploit which methods and tools were adopted to create the process maps essential for implementing the TDABC method. Therefore, systematic reviews addressing that topic are necessary for providing support to healthcare administrators regarding the possibility of automating the discovery of process maps to streamline part of the traditional process that can take weeks, according to some recent publications [14,15,16,17,18,19].
The main objective of this systematic review was to identify the methods used to create process maps for care pathways that utilized the time-driven activity-based costing method. That systematic review aimed to answer three questions: (1) What are the main healthcare fields applied to the TDABC method? (2) What methods were the most used for creating the process maps? (3) Have the created process maps been validated by specialists in the healthcare field?
Methods
This systematic literature review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [20], following the recommendations from the Cochrane Handbook [21].
Inclusion and exclusion criteria
The inclusion criteria were studies published in peer-reviewed journals related to practical cases at healthcare institutions independent from the medical field where the TDABC method was applied. Besides that, we selected studies that measured cost by the TDABC method. All study designs were considered. Literature reviews, abstracts, conference papers, letters to editors, editorials, and gray literature were excluded. We included studies that actively created process maps for applying the TDBAC method and studies that utilized existing process maps found in guidelines, clinical protocols, or established care pathways in the literature.
Literature search strategy
Systematic searches were conducted on the following electronic databases: Embase, PubMed, CINAHL, Scopus, and Web of Science, including publications from 2004 to September 25, 2022. The search strategy was performed based on the following keywords: ((“time-driven activity based cost” OR “time-driven activity based costs” OR “time driven activity based cost” OR “time driven activity based costs” OR “timedriven activity based cost” OR “timedriven activity based costs” OR “time-driven cost” OR “time-driven costs” OR “time driven cost” OR “time driven costs” OR “timedriven cost” OR “timedriven costs” OR “TDABC”) AND (“Costs OR Cost Analysis”)). The searches were limited to full-text studies without language restrictions.
The screening process of the studies
Two independent reviewers performed the study selection process (F.I. and M.R.D.). The selected studies were listed on two Microsoft Excel spreadsheets, abiding by the numerical and alphabetical order based on the first author and the publication year of the study. Each reviewer received the same spreadsheet, including the authors, publication year, title, complete abstract from the study, two columns for their decisions for registering the “yes or no” information, and a column for justification, where each reviewer filled in the reason for inclusion or exclusion of the study. In the first reviewing round, each reviewer analyzed the titles and abstracts, defining if the study would enter the step for reading the entire article. After concluding the independent review step, the selection results were compared. When any uncertainties on the aspects of content analysis occurred, the independent reviewers (F.I. and M.R.D.) discussed them until they agreed. In case of any disagreement, a third reviewer (D.R.C.) obtained consensus by discussing the studies or by arbitration.
Data extraction
The independent authors (F.I. and M.R.D.) read the entire text from each study after the studies were selected. When they identified studies that were noncompliant with the eligibility criteria or were unrelated to practical cases for applying the TDABC method at healthcare institutions and did not measure costs by these methods, those studies were discarded. The eligible studies were listed on a Microsoft Excel spreadsheet after making the final selection, in numerical and alphabetical order, listed by the first author and the study publication year. The data collection was performed by grouping the studies according to their publication year, healthcare fields where the TDABC method was applied, and the construction method of the process maps for each study.
After selecting the studies included in this systematic review, the results were also independently generated by two authors (F.I. and M.R.D.). The results’ structure, organized into four spreadsheets, was devised, and filled out by each author. The results were compared upon completion to avoid errors in allocating final studies.
The risk of bias in eligible studies
The risk of bias of eligible studies and the evaluation of their external validity was not performed, as there were no risk instruments for gauging specific risks of bias for the type of studies included in this review. However, a detailed evaluation of the studies enabled the identification of studies. In contrast, there was insufficient clarity in the methodological process to apply the TDABC method, thereby making it possible to use questionnaires and recommendations for future studies.
Results
Study selection and PRISMA flow diagram
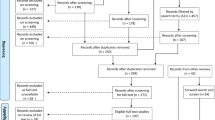
A total of 412 studies were found after searching the selected databases. We identified 130 duplicate studies; there were 282 remaining studies for analysis. Among those, 185 were excluded based on the title or abstract, as they did not mention the use of the TDABC method or were unrelated to the healthcare field. After reviewing the abstracts, 97 studies remained for analysis. Finally, a total of seventy articles were included in our study (Fig. 1).

Flowchart of the selected studies according to the PRISMA statement
General study characteristics
The number of studies with publications related to the TDABC method in the healthcare field has increased in the recent past. Forty-three studies were identified from the 70 selected studies for this review from 2019 to 2022. The number represents 61.4% of the total studies included in the analysis, as shown in Table 1.
Table 2 shows the countries that have applied the TDABC method. Most of the studies are from the United States of America (62.8%), Brazil (7.1%), Australia (4.2%), the United Kingdom (4.2%), and Belgium (4.2%).
Subsequently, we analyzed the healthcare fields where the TDABC method was applied. There is a great variety of hospital surgical procedures, outpatient surgeries, miscellaneous types of hospital services, and sectors where the TDABC method was used for non-hospital services. The TDABC method was applied most commonly to knee arthroplasty (5 studies) in hospital surgical procedures [14, 50, 67, 74, 80], total hip arthroplasty (3 studies) [14, 50, 74], childbirth, and caesarean section (2 studies) [71, 83] and pediatric appendectomy/appendicitis (2 studies) [58, 59].
Diverse types of outpatient surgical procedures were performed. The procedures classified as a miscellaneous hospital or outpatient procedures were predominantly extracorporeal photopheresis procedures (2 studies) [62, 75] and red blood cell transfusion in patients with beta-thalassemia (2 studies) [64, 65]. The studies addressed diverse subjects on non-hospital services, predominantly on studies that proposed to evaluate telemedicine services (3 studies) [15, 51, 63].
We identified some studies in the field of oncology for different clinical pathways, such as breast cancer [31, 56], prostate cancer [30, 39, 42, 79], endometrial cancer [49], uterine cancer [55], and hepatocellular carcinoma [45]. Comparative studies involving new surgical methods through robotic intervention versus traditional methods were also uncovered in our search [44, 60]. All the identified fields are demonstrated in Table 3.
Process map construction
We analyzed how the process maps were created in the selected studies, as the process map creation is an important step for the preparation and application of the TDABC method based on the following five perspectives: (1) direct observation of the procedure; (2) was any hospital documentation and/or medical records used?; (3) did any research, involvement, interview, or meetings with clinical staff occur?; (4) were data from electronic health records used?; (5) were the process maps validated? were other types involved in constructing the process maps?
Most of the included studies utilized direct observations of the procedures [74] and involved the clinical staff, specialists, and multidisciplinary team to create the process maps [73]. 33 (47.1%) of the studies reported using data from electronic healthcare records or hospital documentation to complement the construction of the maps. On the other hand, the majority [67] of the analyzed studies did not validate the process maps after being concluded. The method utilized for creating the process maps in three studies was classified as unclear in their publications; thus, they were classified that way [19, 30, 70].
Regarding the other types of construction, we identified the process maps of a study performed in Canada that created a model for a clinical pathway of a patient submitted to a routine outpatient endoscopic sinus surgery for estimating the cost of this procedure on the patient [72]. In a study performed in Brazil, five main perspectives were analyzed, and the process maps were complemented by the clinical analysis of the protocols in the ischemic stroke condition [61]. The details of how the process maps were constructed in each study are shown in Table 4.
Discussion
The objective of this review has been to analyze the main methods employed in creating process maps for applying the TDABC method, searching for answers to three key questions: (1) What are the main healthcare fields where the TDABC method is applied? (2) What methods were mostly used for creating the process maps? (3) Are the created process maps validated by specialists in those fields? Seventy studies were included. The most identified hospitalized surgical procedures were in the orthopedic field, and studies performed in oncology or procedures related to that field. Studies were comparing new technologies to traditional methods found in this review. We found three studies that addressed telemedicine services in non-hospital services.
The most studies are from the United States of America, however, other countries, such as Brazil, have also begun to adopt the method for cost mapping [16, 60,61,62,63]. Despite the increasing use of TDABC in health-related studies, methodological heterogeneity still exists in how researchers map their clinical processes, present their methods, and report their results [85]. We observed a wide variety of clinical pathways and other studied procedures. We identified a total of 63 different applications that utilized the TDABC method out of the total 70 included studies. This illustrates the significant heterogeneity in themes and applications in using TDABC. Despite having a high degree of heterogeneity (99.1%), this review demonstrated that the TDABC method can be applied to various conditions, allowing cost measurement through the best and most efficient method for cost measurement in healthcare [8, 9].
The main methods for creating process maps are performed by direct observation of the procedure with the involvement of specialists in those fields, and the participation of a multidisciplinary team. We found validation reports only in 33% of the studies among the created process maps. Regarding the tools used to build process maps, we identified studies using QlikView and R software [78], Microsoft Excel and Adobe Illustrator [82] and using digital platforms such as Bizagi or Microsoft Visio [86]. Regarding the use of electronic data in healthcare, one systematic review in 2017 identified a study where the process maps were created based on electronic medical records involving surgeries and medical care procedures [3]. In our review, the electronic medical records were used to construct the process maps identified in 23 studies [5, 16, 22, 24,25,26, 29, 32, 34, 36, 43, 47, 48, 58, 59, 61, 66, 74, 75, 77, 78, 82, 84], proving that using medical data from electronic medical records has enhanced and provided support to the process.
Although the use of electronic data has increased in the past few years, the step of creating process maps for the TDABC method still demands time and the availability of the multidisciplinary team when. We found studies that reported that the total period for constructing process maps ranged from one to 12 weeks [14, 18, 59, 66]. Since there is a growing number of studies utilizing electronic medical data and the construction of the process maps demands longer periods until they are concluded, applying process mining methods can supply new and efficient ways for mapping healthcare processes [3, 87]. Process mining aims to extract knowledge from data in electronic records [88, 89]. Process mining can generate healthcare flowcharts based on administrative or clinical data collected routinely, thereby enabling the automated identification of process maps by identifying events that generally occur in a time sequence [90]. A systematic review identified that healthcare is currently the main field of application for process mining, demonstrating its total applicability to this segment [91]. Another recent publication demonstrated that process mining provides the greatest applicability in the discovery for analyzing process models for evaluating patient healthcare, compliance process evaluation to compare medical protocols and clinical guidelines and performance, bottlenecks, and time management evaluations [92].
The main product process mining is capable of supplying, and it contributes to streamlining the construction of process maps for the TDABC method, which are care flow maps and workflow networks that describe the detailed flow of patients [93]. In care flow maps, the main activities are viewed based on their frequency and established relations between activities and their reoccurrences. The application of process mining also enables identifying the duration between activities [94]. In the case of the TDABC method, the direct timed observations can be automated by applying this technique, as the process maps can be generated in an automated manner through electronic data contained in the hospital data systems [95].
Healthcare processes are known to be highly dynamic, complex, and increasingly multidisciplinary [89]. Therefore, it is important to define the analysis goal to overcome this challenge, starting from the first step of TDABC by selecting the medical condition. After the selection, data processing can be carried out to reduce the variability of data in a patient’s event trajectory, discarding irrelevant information that may be present in the electronic health record. Following data processing, process mining techniques can be applied to generate a process flow, which can then be validated by experts in the field [92].
Process mining has a high potential to substantially contribute to creating process maps for preparing the TDABC method, streamlining the direct observations of procedures for measuring periods, which are currently performed manually. It is worth mentioning that applying process mining and discovering process models do not rule out the validity of specialized professionals in this field, nor the involvement of a multidisciplinary team at institutions. There were 23 studies in our review that validated process maps [14,15,16, 18, 22, 23, 26, 33, 38, 39, 46, 48, 58, 61, 63,64,65,66, 68, 75, 77, 78, 80].
Process mining could add different sources of information and merge them with the conventional model to minimize the biases from registering and validating the discovered maps. That would make it feasible to identify more precisely the fields with greater variability in processes [3] and aid healthcare administrators in identifying important markers of the process map, enabling improved and more agile process management. In future studies, we intend to develop the TDABC method in different oncology fields, utilizing process mining to prepare the process maps to calculate the cost of clinical pathways most relevant to the public healthcare field in Brazil.
Conclusions
We identified that the TDABC method has been more commonly implemented in the past few years and applied to diverse healthcare fields, predominantly in hospital surgical services in orthopedics, oncology, and outpatient telemedicine services. We consider creating process maps, a fundamental step for preparing the TDABC method, which is still performed mostly conservatively. We believe there is great potential in applying process mining to contribute to that process due to its high degree of applicability in the healthcare field, as well as its capability to identify through the discovery of models the main activities, jointly with their established relations, as well as demonstrate the necessary time between one activity and another.
A high degree of variability is encountered in the healthcare field, and there is an increasing amount of data in hospital systems. It can be challenging to create manual process maps. Process mining is an effective technique that has displayed great potential for discovering healthcare clinical pathways, even when facing the large volume of information and the large variation of activities found in clinical pathways. The TDABC method would make this process more agile, minimize the need for analyzing the period of procedures, meetings, and workshops with key stakeholders in institutions, and aid healthcare administrators in improving their process analyses.
Data availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- TDABC:
-
time-driven activity-based costing
References
Kaplan RS, Anderson SR. Time-driven activity-based costing. Harv Bus Rev. 2004;82(11):131–8.
Kaplan AL, Agarwal N, Setlur NP, Tan HJ, Niedzwiecki D, McLaughlin N, et al. Measuring the cost of care in Benign Prostatic Hyperplasia using time-driven activity-based costing (TDABC). Healthc (Amst). 2015;3(1):43–8.
Keel G, Savage C, Rafiq M, Mazzocato P. Time-driven activity-based costing in health care: a systematic review of the literature. Health Policy. 2017;121(7):755–63.
Etges A, Polanczyk CA, Urman RD. A standardized framework to evaluate the quality of studies using TDABC in healthcare: the TDABC in Healthcare Consortium Consensus Statement. BMC Health Serv Res. 2020;20(1):1107.
Anzai Y, Heilbrun ME, Haas D, Boi L, Moshre K, Minoshima S, et al. Dissecting costs of CT study: application of TDABC (Time-driven activity-based Costing) in a Tertiary Academic Center. Acad Radiol. 2017;24(2):200–8.
Basto J, Chahal R, Riedel B. Time-driven activity-based costing to model the utility of parallel induction redesign in high-turnover operating lists. Healthc (Amst). 2019;7(3):100355.
McLaughlin N, Burke MA, Setlur NP, Niedzwiecki DR, Kaplan AL, Saigal C, et al. Time-driven activity-based costing: a driver for provider engagement in costing activities and redesign initiatives. Neurosurg Focus. 2014;37(5):E3.
Vargas D, David C, Horvath J, Silva T, Pereira M, Rigoni L, et al. The use of micro-costing in an economic analysis of allogeneic HSCT in Brazil. Jornal Brasileiro De Economia Da Saúde. 2021;13(2):166–74.
Ostadi B, Mokhtarian Daloie R, Sepehri MM. A combined modelling of fuzzy logic and time-driven activity-based Costing (TDABC) for hospital services costing under uncertainty. J Biomed Inform. 2019;89:11–28.
Constantinescu DS, Haziza S, Vanden Berge DJ, McNamara CA, Hernandez VH, D’Apuzzo MR. Time-Driven activity-based costing in preoperative tasks for total hip and knee arthroplasty. J Arthroplasty. 2022;37(5):809–13.
Etges A, Ruschel KB, Polanczyk CA, Urman RD. Advances in value-based Healthcare by the application of Time-Driven activity-based costing for Inpatient Management: a systematic review. Value Health. 2020;23(6):812–23.
Cidav Z, Mandell D, Pyne J, Beidas R, Curran G, Marcus S. A pragmatic method for costing implementation strategies using time-driven activity-based costing. Implement Sci. 2020;15(1):28.
Pathak S, Snyder D, Kroshus T, Keswani A, Jayakumar P, Esposito K, et al. What are the uses and limitations of Time-driven activity-based costing in total joint replacement? Clin Orthop Relat Res. 2019;477(9):2071–81.
Akhavan S, Ward L, Bozic KJ. Time-driven activity-based Costing more accurately reflects costs in arthroplasty Surgery. Clin Orthop Relat Res. 2016;474(1):8–15.
Cidav Z, Marcus S, Mandell D, Hornbrook MC, Mo JJ, Sun V, et al. Programmatic costs of the Telehealth Ostomy Self-Management Training: an application of Time-Driven activity-based costing. Value Health. 2021;24(9):1245–53.
da Silva Etges APB, Cruz LN, Schlatter R, Neyeloff J, Cardoso RB, Kopittke L, et al. Time-driven activity-based costing as a strategy to increase efficiency: an analyses of interventional coronary procedures. Int J Health Plann Manage. 2022;37(1):189–201.
Demeere N, Stouthuysen K, Roodhooft F. Time-driven activity-based costing in an outpatient clinic environment: development, relevance and managerial impact. Health Policy. 2009;92(2–3):296–304.
Koehler DM, Balakrishnan R, Lawler EA, Shah AS. Endoscopic Versus Open Carpal tunnel release: a detailed analysis using time-driven activity-based costing at an Academic Medical Center. J Hand Surg Am. 2019;44(1):62 e1–e9.
Hamid KS, Matson AP, Nwachukwu BU, Scott DJ, Mather RC 3rd, DeOrio JK. Determining the cost-savings threshold and Alignment Accuracy of Patient-Specific Instrumentation in total ankle replacements. Foot Ankle Int. 2017;38(1):49–57.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2019.
Albright P, Only A, Parikh HR, McCreary DL, Hayek K, Siljander B, et al. External fixation characteristics drive cost of Care for High-Energy Tibial Plateau fractures. J Orthop Trauma. 2022;36(4):189–94.
Balakrishnan K, Goico B, Arjmand EM. Applying cost accounting to operating room staffing in otolaryngology: time-driven activity-based costing and outpatient adenotonsillectomy. Otolaryngol Head Neck Surg. 2015;152(4):684–90.
Berkowitz ST, Sternberg P Jr., Patel S. Cost analysis of routine vitrectomy Surgery. Ophthalmol Retina. 2021;5(6):496–502.
Bobade RA, Helmers RA, Jaeger TM, Odell LJ, Haas DA, Kaplan RS. Time-driven activity-based cost analysis for outpatient anticoagulation therapy: direct costs in a primary care setting with optimal performance. J Med Econ. 2019;22(5):471–7.
Bodar YJL, Srinivasan AK, Shah AS, Kawal T, Shukla AR. Time-Driven activity-based costing identifies opportunities for process efficiency and cost optimization for robot-assisted laparoscopic pyeloplasty. J Pediatr Urol. 2020;16(4):460 e1–e10.
Boyce-Fappiano D, Ning MS, Thaker NG, Pezzi TA, Gjyshi O, Mesko S, et al. Time-Driven, activity-based cost analysis of Radiation Treatment options for spinal metastases. JCO Oncol Pract. 2020;16(3):e271–e9.
Carducci MP, Mahendraraj KA, Menendez ME, Rosen I, Klein SM, Namdari S, et al. Identifying surgeon and institutional drivers of cost in total shoulder arthroplasty: a multicenter study. J Shoulder Elbow Surg. 2021;30(1):113–9.
Deutsch SA, Zomorrodi A, Zent J, Kirk A, O’Brien P, Loiselle C, et al. Hospital costs, revenue, and abuse detection Associated with Occult Injury Screening. Acad Pediatr. 2022;22(6):989–96.
Dutta SW, Bauer-Nilsen K, Sanders JC, Trifiletti DM, Libby B, Lash DH, et al. Time-driven activity-based cost comparison of Prostate cancer brachytherapy and intensity-modulated radiation therapy. Brachytherapy. 2018;17(3):556–63.
Dziemianowicz M, Burmeister J, Dominello M. Examining the Financial impact of altered fractionation in Breast Cancer: an analysis using time-driven activity-based costing. Pract Radiat Oncol. 2021;11(4):245–51.
El Alaoui S, Lindefors N. Combining Time-Driven activity-based costing with clinical outcome in cost-effectiveness analysis to measure value in treatment of Depression. PLoS ONE. 2016;11(10):e0165389.
Erhun F, Mistry B, Platchek T, Milstein A, Narayanan VG, Kaplan RS. Time-driven activity-based costing of multivessel coronary artery bypass grafting across national boundaries to identify improvement opportunities: study protocol. BMJ Open. 2015;5(8):e008765.
French KE, Guzman AB, Rubio AC, Frenzel JC, Feeley TW. Value based care and bundled payments: anesthesia care costs for outpatient oncology Surgery using time-driven activity-based costing. Healthc (Amst). 2016;4(3):173–80.
Gaitonde S, Malik R, Zimmern P. Financial burden of recurrent urinary tract Infections in women: a time-driven activity-based cost analysis. J Urol. 2018;199(4):e650–e.
Hagedorn KN, Hayatghaibi SE, Levine MH, Orth RC. Cost comparison of Ultrasound Versus MRI to diagnose adolescent female patients presenting with Acute Abdominal/Pelvic Pain using Time-Driven activity-based costing. Acad Radiol. 2019;26(12):1618–24.
Hawranko R, Sohn JJ, Neiderer K, Bump E, Harris T, Fields EC et al. Investigation of Isotoxic Dose Escalation and Plan Quality with TDABC Analysis on a 0.35 T MR-Linac (MRL) system in ablative 5-Fraction stereotactic magnetic resonance-guided Radiation Therapy (MRgRT) for primary Pancreatic Cancer. J Clin Med. 2022;11(9).
Hayatghaibi SE, Chau A, Wadler EG, Levine MH, Hernandez AJ, Orth RC. Cost comparison of In-Suite Versus Portable tunneled femoral Central Line Placements in Children using Time-Driven activity-based costing. J Am Coll Radiol. 2020;17(4):462–8.
Ilg AM, Laviana AA, Kamrava M, Veruttipong D, Steinberg M, Park SJ, et al. Time-driven activity-based costing of low-dose-rate and high-dose-rate brachytherapy for low-risk Prostate cancer. Brachytherapy. 2016;15(6):760–7.
Koolmees DS, Ramkumar PN, Solsrud K, Yedulla NR, Elhage KG, Cross AG, et al. Time-Driven activity-based costing accurately determines bundle cost for Rotator Cuff Repair. Arthroscopy. 2022;38(8):2370–7.
Kukreja JB, Seif MA, Mery MW, Incalcaterra JR, Kamat AM, Dinney CP, et al. Utilizing time-driven activity-based costing to determine open radical cystectomy and ileal conduit surgical episode cost drivers. Urol Oncol. 2021;39(4):237 e1–e5.
Laviana AA, Ilg AM, Veruttipong D, Tan HJ, Burke MA, Niedzwiecki DR, et al. Utilizing time-driven activity-based costing to understand the short- and long-term costs of treating localized, low-risk Prostate cancer. Cancer. 2016;122(3):447–55.
Laviana AA, Kundavaram CR, Tan H-J, Burke MA, Niedzwiecki D, Lee RK, et al. Determining the true costs of treating small renal masses using Time Driven, Activity Based Costing. Urol Pract. 2016;3(3):180–6.
Laviana AA, Tan HJ, Hu JC, Weizer AZ, Chang SS, Barocas DA. Retroperitoneal versus transperitoneal robotic-assisted laparoscopic partial nephrectomy: a matched-pair, bicenter analysis with cost comparison using time-driven activity-based costing. Curr Opin Urol. 2018;28(2):108–14.
Ljuboja D, Ahmed M, Ali A, Perez E, Subrize MW, Kaplan RS, et al. Time-Driven activity-based costing in Interventional Oncology: cost measurement and cost variability for Hepatocellular Carcinoma therapies. J Am Coll Radiol. 2021;18(8):1095–105.
McClintock TR, Friedlander DF, Feng AY, Shah MA, Pallin DJ, Chang SL, et al. Determining variable costs in the Acute Urolithiasis cycle of Care through Time-Driven activity-based costing. Urology. 2021;157:107–13.
McCreary DL, White M, Vang S, Plowman B, Cunningham BP. Time-Driven activity-based costing in Fracture Care: is this a more accurate way to prepare for alternative payment models? J Orthop Trauma. 2018;32(7):344–8.
Nguyen HN, Sammer MB, Bales B, Cano MC, Trout AT, Dillman JR, et al. Time-Driven activity-based cost comparison of three imaging pathways for suspected Midgut Volvulus in Children. J Am Coll Radiol. 2020;17(12):1563–70.
Ning MS, Klopp AH, Jhingran A, Lin LL, Eifel PJ, Vedam S, et al. Quantifying institutional resource utilization of adjuvant brachytherapy and intensity-modulated radiation therapy for endometrial cancer via time-driven activity-based costing. Brachytherapy. 2019;18(4):445–52.
Palsis JA, Brehmer TS, Pellegrini VD, Drew JM, Sachs BL. The cost of joint replacement: comparing two approaches to evaluating costs of total hip and knee arthroplasty. J Bone Joint Surg Am. 2018;100(4):326–33.
Parikh NR, Chang EM, Kishan AU, Kaprealian TB, Steinberg ML, Raldow AC. Time-Driven activity-based costing analysis of Telemedicine Services in Radiation Oncology. Int J Radiat Oncol Biol Phys. 2020;108(2):430–4.
Pollard ME, Laviana AA, Kaplan AL, Pagan C, Saigal CS. Time-Driven activity-based costing analysis of Urological Stone Disease. Urol Pract. 2018;5(5):327–33.
Shankar PR, Parikh KR, Heilbrun ME, Sweeney BM, Flake AN, Herbstman EA, et al. Cost Implications of Oral Contrast Administration in the Emergency Department: a Time-Driven activity-based costing analysis. J Am Coll Radiol. 2019;16(1):30–8.
Simmonds JC, Hollis RJ, Tamberino RK, Vecchiotti MA, Scott AR. Comparing the real and perceived cost of adenotonsillectomy using time-driven activity-based costing. Laryngoscope. 2019;129(6):1347–53.
Su L, Dutta SW, Sanders JC, Wu T, Libby B, Romano KD, et al. Time-driven activity-based costing of adjuvant vaginal cuff brachytherapy for Uterine cancer in an integrated brachytherapy suite. Brachytherapy. 2020;19(2):176–80.
Suralik G, Rudra S, Dutta SW, Yu J, Sanders JC, Schad MD, et al. Time-driven activity-based costing of a novel form of CT-guided high-dose-rate brachytherapy intraoperative radiation therapy compared with conventional breast intraoperative radiation therapy for early stage Breast cancer. Brachytherapy. 2020;19(3):348–54.
Thaker NG, Orio PF, Potters L. Defining the value of magnetic resonance imaging in prostate brachytherapy using time-driven activity-based costing. Brachytherapy. 2017;16(4):665–71.
Yu YR, Abbas PI, Smith CM, Carberry KE, Ren H, Patel B, et al. Time-driven activity-based costing to identify opportunities for cost reduction in pediatric appendectomy. J Pediatr Surg. 2016;51(12):1962–6.
Yu YR, Abbas PI, Smith CM, Carberry KE, Ren H, Patel B, et al. Time-driven activity-based costing: a dynamic value assessment model in pediatric Appendicitis. J Pediatr Surg. 2017;52(6):1045–9.
de Oliveira RAR, Guimaraes GC, Mourao TC, de Lima Favaretto R, Santana TBM, Lopes A, et al. Cost-effectiveness analysis of robotic-assisted versus retropubic radical prostatectomy: a single cancer center experience. J Robot Surg. 2021;15(6):859–68.
Etges A, Marcolino MAZ, Ogliari LA, de Souza AC, Zanotto BS, Ruschel R, et al. Moving the Brazilian ischaemic Stroke pathway to a value-based care: introduction of a risk-adjusted cost estimate model for Stroke treatment. Health Policy Plan. 2022;37(9):1098–106.
Vargas DF, Pereira MP, Silva TS, de David CN, Paz AA, Astigarraga CC. Extracorporeal photopheresis in chronic graft-versus-host Disease: clinical description and economic study. Hematol Transfus Cell Ther. 2021.
Zanotto BS, Etges A, Siqueira AC, Silva RSD, Bastos C, Araujo AL, et al. Economic evaluation of a Telemedicine Service to expand primary Health Care in Rio Grande do sul: TeleOftalmo’s microcosting analysis. Cien Saude Colet. 2020;25(4):1349–60.
Burns KE, Haysom HE, Higgins AM, Waters N, Tahiri R, Rushford K, et al. A time-driven, activity-based costing methodology for determining the costs of red blood cell transfusion in patients with beta thalassaemia major. Transfus Med. 2019;29(1):33–40.
McQuilten ZK, Higgins AM, Burns K, Chunilal S, Dunstan T, Haysom HE, et al. The cost of blood: a study of the total cost of red blood cell transfusion in patients with beta-thalassemia using time-driven activity-based costing. Transfusion. 2019;59(11):3386–95.
Boehler CE, Milton KE, Bull FC, Fox-Rushby JA. The cost of changing physical activity behaviour: evidence from a physical activity pathway in the primary care setting. BMC Public Health. 2011;11:370.
Chen A, Sabharwal S, Akhtar K, Makaram N, Gupte CM. Time-driven activity based costing of total knee replacement Surgery at a London teaching hospital. Knee. 2015;22(6):640–5.
Sabharwal S, Carter AW, Rashid A, Darzi A, Reilly P, Gupte CM. Cost analysis of the surgical treatment of fractures of the proximal humerus: an evaluation of the determinants of cost and comparison of the institutional cost of treatment with the national tariff. Bone Joint J. 2016;98–B(2):249–59.
Crott R, Lawson G, Nollevaux MC, Castiaux A, Krug B. Comprehensive cost analysis of sentinel node biopsy in solid head and neck tumors using a time-driven activity-based costing approach. Eur Arch Otorhinolaryngol. 2016;273(9):2621–8.
Defourny N, Perrier L, Borras JM, Coffey M, Corral J, Hoozee S, et al. National costs and resource requirements of external beam radiotherapy: a time-driven activity-based costing model from the ESTRO-HERO project. Radiother Oncol. 2019;138:187–94.
Dubron K, Verschaeve M, Roodhooft F. A time-driven activity-based costing approach for identifying variability in costs of Childbirth between and within types of delivery. BMC Pregnancy Childbirth. 2021;21(1):705.
Au J, Rudmik L. Cost of outpatient endoscopic sinus Surgery from the perspective of the Canadian government: a time-driven activity-based costing approach. Int Forum Allergy Rhinol. 2013;3(9):748–54.
Sadri H, Sinigallia S, Shah M, Vanderheyden J, Souche B. Time-Driven activity-based costing for cataract Surgery in Canada: the case of the Kensington Eye Institute. Healthc Policy. 2021;16(4):97–108.
Andreasen SE, Holm HB, Jorgensen M, Gromov K, Kjaersgaard-Andersen P, Husted H. Time-driven activity-based cost of fast-track total hip and knee arthroplasty. J Arthroplasty. 2017;32(6):1747–55.
Azar N, Leblond V, Ouzegdouh M, Button P. A transition from using multi-step procedures to a fully integrated system for performing extracorporeal photopheresis: a comparison of costs and efficiencies. J Clin Apher. 2017;32(6):474–8.
Chirenda J, Nhlema Simwaka B, Sandy C, Bodnar K, Corbin S, Desai P, et al. A feasibility study using time-driven activity-based costing as a management tool for provider cost estimation: lessons from the national TB control program in Zimbabwe in 2018. BMC Health Serv Res. 2021;21(1):242.
Doyle GA, O’Donnell S, Cullen K, Quigley E, Gibney S, Diabetes Literacy C. Understanding the cost of care of type 2 Diabetes Mellitus - a value measurement perspective. BMJ Open. 2022;12(1):e053001.
Keel G, Muhammad R, Savage C, Spaak J, Gonzalez I, Lindgren P, et al. Time-driven activity-based costing for patients with multiple chronic conditions: a mixed-method study to cost care in a multidisciplinary and integrated care delivery centre at a university-affiliated tertiary teaching hospital in Stockholm, Sweden. BMJ Open. 2020;10(6):e032573.
Keyrilainen J, Sjoblom O, Turnbull-Smith S, Hovirinta T, Minn H. Clinical experience and cost evaluation of magnetic resonance imaging -only workflow in radiation therapy planning of Prostate cancer. Phys Imaging Radiat Oncol. 2021;19:66–71.
Khan RM, Albutt K, Qureshi MA, Ansari Z, Drevin G, Mukhopadhyay S, et al. Time-driven activity-based costing of total knee replacements in Karachi, Pakistan. BMJ Open. 2019;9(5):e025258.
Kumar A, Siddharth V, Singh SI, Narang R. Cost analysis of treating Cardiovascular Diseases in a super-specialty hospital. PLoS ONE. 2022;17(1):e0262190.
Masthoff M, Schneider KN, Schindler P, Heindel W, Kohler M, Schluchtermann J, et al. Value Improvement by Assessing IR Care via Time-Driven activity-based costing. J Vasc Interv Radiol. 2021;32(2):262–9.
Odhiambo J, Ruhumuriza J, Nkurunziza T, Riviello R, Shrime M, Lin Y, et al. Health Facility cost of Cesarean Delivery at a Rural District Hospital in Rwanda using Time-Driven activity-based costing. Matern Child Health J. 2019;23(5):613–22.
Thaker NG, Pugh TJ, Mahmood U, Choi S, Spinks TE, Martin NE, et al. Defining the value framework for prostate brachytherapy using patient-centered outcome metrics and time-driven activity-based costing. Brachytherapy. 2016;15(3):274–82.
Etges A, Polanczyk CA, Urman RD. A standardized framework to evaluate the quality of studies using TDABC in healthcare: the TDABC in Healthcare Consortium Consensus Statement. BMC Health Serv Res. 2020;20(1).
da Silva Etges APB, Cruz LN, Notti RK, Neyeloff JL, Schlatter RP, Astigarraga CC, et al. An 8-step framework for implementing time-driven activity-based costing in healthcare studies. Eur J Health Econ. 2019;20(8):1133–45.
Rebuge Á, Ferreira DR. Business process analysis in healthcare environments: a methodology based on process mining. Inform Syst. 2012;37(2):99–116.
Erdogan TG, Tarhan A. Systematic mapping of process mining studies in Healthcare. IEEE Access. 2018;6:24543–67.
Rojas E, Munoz-Gama J, Sepulveda M, Capurro D. Process mining in healthcare: a literature review. J Biomed Inform. 2016;61:224–36.
Dagliati A, Sacchi L, Zambelli A, Tibollo V, Pavesi L, Holmes JH, et al. Temporal electronic phenotyping by mining careflows of Breast cancer patients. J Biomed Inform. 2017;66:136–47.
Garcia CS, Meincheim A, Faria Junior ER, Dallagassa MR, Sato DMV, Carvalho DR, et al. Process mining techniques and applications – A systematic mapping study. Expert Syst Appl. 2019;133:260–95.
Dallagassa MR, dos Santos Garcia C, Scalabrin EE, Ioshii SO, Carvalho DR. Opportunities and challenges for applying process mining in healthcare: a systematic mapping study. J Ambient Intell Humaniz Comput. 2021;13(1):165–82.
Partington A, Wynn M, Suriadi S, Ouyang C, Karnon J. Process mining for clinical processes. ACM Trans Manage Inform Syst. 2015;5(4):1–18.
Williams R, Ashcroft DM, Brown B, Rojas E, Peek N, Johnson O. Process mining in primary care: avoiding adverse events due to Hazardous Prescribing. Stud Health Technol Inform. 2019;264:447–51.
Van Der Aalst W. Process mining: data science in action. Springer; 2016.
Acknowledgements
The authors would like to thank you for supporting the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) under grant No.: 88887.709155/2022-00.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Author information
Authors and Affiliations
Contributions
Franciele Iachecen: Conceptualization; methodology; validation; investigation; data curation; writing - original draft; and visualization. Marcelo Rosano Dallagassa: Conceptualization; methodology; validation; investigation; data curation; writing - original draft; and visualization. Deborah Ribeiro Carvalho: Conceptualization; methodology; writing – review, editing and data curation. Eduardo Alves Portela Santos: Conceptualization, writing, review, and editing. Sergio Ossamu Ioshii: Conceptualization; methodology; investigation; resources; writing - review and editing; visualization; and supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Iachecen, F., Dallagassa, M.R., Portela Santos, E.A. et al. Is it possible to automate the discovery of process maps for the time-driven activity-based costing method? A systematic review. BMC Health Serv Res 23, 1408 (2023). https://doi.org/10.1186/s12913-023-10411-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-023-10411-z