
Abstract
Background
Learning to interpret electrocardiograms (ECGs) is a crucial objective in medical education. Despite its importance, errors in ECGs interpretation are common, and the optimal teaching methods have not yet been clearly established.
Objectives
To evaluate students’ confidence in ECGs analysis and their opinion on current teaching methods, and to assess the effectiveness of a new ECG educational approach.
Methods
First, we conducted a survey on ECG learning among fourth to sixth-year medical students. Second, a 5-week multicenter comparative study was conducted with fourth-year medical students during their cardiology internship. Two different teaching methods were used, assigned by center. The first group participated in 5-minutes workshops 4 times a week using a “reversed classroom” method, supervised by a cardiologist, where students took turns selecting, presenting and discussing ECGs. The control group attended a single 2-hour face-to-face ECG course. All participants completed a 30-minute ECGs analysis test at baseline and after 5 weeks.
Results
Out of 401 survey respondents, the confidence levels in ECG interpretation were 3/5 (IQR 2–3) for routine situations and 2/5 (IQR 1–3) for emergency situations. Satisfaction with ECG teaching was low (2/5, IQR 1–3) and 96.3% of respondents favored more extensive ECG training. In the comparative study, 52 students from 3 medical schools were enrolled (control group: n = 27; workshop group: n = 25). Both groups showed significant improvement in exam scores from baseline to 5-week (33/100 ± 12/100 to 44/100 ± 12/100, p < 0.0001 for the control group and 36/100 ± 13/100 to 62/100 ± 12/100, p < 0.0001 for the workshop group). The improvement was significantly greater in the workshop group compared to the control group (+ 26 ± 11 vs. + 11 ± 6, p < 0.001).
Conclusions
Among French medical students who initially reported low confidence and insufficient skills in ECG interpretation, the workshop approach using a “reversed classroom” method was found to be more effective than conventional lecture-based teaching during cardiology internship.
Graphical abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Accurate interpretation of electrocardiograms (ECGs) is a fundamental skill in medical education, given their routine use in the diagnosis and evaluation of various cardiac diseases. Despite their widespread use, errors in ECG interpretation are frequent [1,2,3]. Berger et al.. found a high rate of misinterpretation among medical residents, with less than 50% accuracy in diagnosing basic tracings such as complete AV block [4]. Inaccurate ECG interpretation can result in the absence of critical treatment (i.e. complete AV block, ventricular arrhythmia, acute coronary syndrome) or in unnecessary interventions [5]. Bogun et al.. reported that incorrect diagnosis of atrial fibrillation in 4% of patients led to inappropriate treatments, such as unnecessary anticoagulant or antiarrhythmic therapies [5].
Teaching ECG analysis presents significant challenges due to its complexity, so students are often reluctant to engage with the subject. In response to these challenges, the American College of Cardiology issued guidelines [3] recommending that healthcare professionals interpret at least 500 ECGs under expert supervision to achieve clinical competence. However, mere repetition is insufficient; understanding the underlying pathophysiology is crucial for accurate diagnosis. With a variety of pedagogical materials available (e.g., books, articles, quiz, videos) and differing teaching methods across medical schools and countries (e.g., self-directed, workshop-based, lecture-based) [6, 7], the optimal approach remains unclear [2]. While not all medical students need to become ECG experts, they must be capable of recognizing life-threatening conditions. This study aimed to (1) assess students’ confidence in ECG analysis and their perceptions of current teaching methods; and (2) evaluate the effectiveness of a new ECG teaching method.
Methods
Survey on ECG learning
The first part of the study involved a survey on ECG learning. An anonymous, electronic survey was distributed to students in their fourth to sixth years of medical training at three French medical schools. The questionnaire assessed students’ confidence in interpreting ECGs both in routine practice and emergency situations. It also evaluated their satisfaction with current teaching methods and the perceived importance of ECG interpretation for their future medical practice. Responses were collected using Likert scales ranging from 1 to 5. The survey recorded the methods used by the students to interpret ECG tracings, including: (1) Sequential ECG analysis (atrial activity, AV conduction, ventricular activation, ventricular repolarization); (2) FRAICH method (French acronym for Rate, Rhythm, Axis, Ischemia, Conduction, Hypertrophy); (3) Visual memorization of ECG tracings; (4) Other methods. Additionally, students were asked about their preferred medical or surgical specialty for their future practice. The full survey is provided in Supplementary Appendix 1.
Comparative study
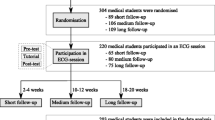
This prospective, multicenter, comparative study was conducted from May 2023 to September 2023, spanning 3 successive internship periods for medical students. Participants were recruited from three French hospitals during their cardiology internships. This study received approval from educational directors and informed consent was obtained from all participants. All students were in their fourth year of medical school and had previously completed ECG training courses according to national objectives, in their 2nd and 4th years.
The study duration was 5 weeks. The teaching method was nonrandomly assigned according to the center. In two French hospitals, students were assigned to the control group, while in the third hospital, students were assigned to the workshop Group.
In the workshop group, 5-minute workshops were conducted 4 times a week throughout the study period. The “reversed classroom” method was employed, where students took turns to selecting and presenting ECGs from patients encountered during their cardiology internship. Each workshop focused on a single ECG, with each student presenting at least two different ECGs over the study period. Students had one minute to reflect on the presented ECG tracing. A correction was then provided by the student presenter. A cardiologist specialized in arrhythmia management was present to emphasize key teaching points and offer additional explanations.
The control group attended a single 2-hour face-to-face ECG course, 3 weeks after the start of their cardiology internship. The course, led by a cardiologist specialized in cardiac arrhythmias, included detailed explanations of ECG interpretation techniques. Students were shown a range normal and abnormal ECG tracing covering the required knowledge. The course content and materials were at the discretion of the instructor and were consistent with the teaching methods previously used in these centers.
Evaluation methods
All participants completed a 30-minute ECG analysis test at the start and at 5 weeks of their cardiology internship. The test consisted of 10 ECG tracings accompanied by open-ended questions. Importantly, no correction was provided after the initial test and the same tracings were used for both initial and final evaluations. Some questions contained brief summaries of medical records and required participants to provide a complete and accurate ECG diagnosis. These 10 tracings were selected to represent key conditions that graduating medical students should be able to diagnose, such as complete heart block, myocardial infarction, ventricular tachycardia, atrial fibrillation, atrial flutter. To ensure comprehensive assessment, some ECGs included multiple diagnoses.
Additionally, participants completed the previously described survey on ECG learning at baseline and 5 weeks. All exam papers were graded by the same instructor, who was blinded to the participants’ assigned groups. A 100-point grading scale (10 points per tracing) was established prior to the study. The primary endpoint was the difference between the scores at the end of the stud and the baseline scores.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data or median and interquartile range (IQR) for non-normally distributed data. Normal distribution was assessed using the Shapiro-Wilk test. Survey results, based on Likert scales, were presented as medians and IQRs. Categorical variables were reported as counts and percentage. Comparisons between categorical variables were performed using the Chi-squared test or Fisher’s exact test, while comparisons for continuous variables were conducted using Student’s t-test or Mann–Whitney U test, as appropriate. To evaluate changes in scores from baseline to the end of the study within each group, a paired t-test was employed. Additionally, a one-way ANOVA was used to compare score changes between the two groups over the 5-week period. All tests were two-sided, with a p-value < 0.05 considered statistically significant. All analyses were performed using the R 3.6.3 software (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Survey
A total of 401 students from 3 different universities responded to the survey on ECG learning. Of these, 170 (42.4%) were in their 4th year, 147 (36.7%) in their 5th year and 84 (20.9%) in their 6th year of medical studies. On a Likert scale ranging from 1 (very unconfident) to 5 (very confident), students reported an overall confidence level of 3 (IQR 2–3) in ECG interpretation during routine medical situations. Confidence in emergency situations was significantly lower as compared to routine medical situations with a median of 2, IQR 1–3 (p < 0.0001). Of note, students intending to specialize in cardiology demonstrated higher confidence level in ECG interpretation than others (in routine situations 4, IQR 3–4 vs. 3, IQR 2–3; p = 0.0002 and in emergency situations 3, IQR 2–3 vs. 2, IQR 1–3; p < 0.0001). Respondents overall placed high importance on ECG interpretation skills for their future medical careers with a median of 5, IQR 4–5 on a scale ranging from 1 to 5 (Fig. 1).

Results of the survey on 401 medical students. Results are indicated on a Likert scale ranging from 1 to 5. Panel A: Level of confidence during ECG interpretation in current medical practice. Panel B: Level of confidence during ECG interpretation in emergency situation. Panel C: Importance attached to ECG interpretation skills in the future medical practice. Panel D: Level of satisfaction with ECG teaching
Regarding methods used for ECG analysis, the FRAICH method predominantly favored, used by 305 out of 401 students (76.4%), compared to other methods such as sequential ECG analysis (57/401, 14.2%), visual memorization (23/401, 5.7%) or other methods (16/401, 4%) (p < 0.0001) (Fig. 2).

Distribution of the methods used to interpret ECG tracings among questioned students
Satisfaction with ECG teaching during the early years of medical training was generally low with a median rating of 2, IQR 1–3. Most respondents felt that the current educational methods were not well-suited to teaching ECG interpretations (median of 2, IQR 2–3).
The great majority of respondents (386 / 401, 96.3%) advocated for more extensive ECG training. The most common suggestions included: (1) regular training (at least weekly) in person or via videoconference (37% of all responders); (2) quarterly workshops in small groups (31%); and (3) access to a bank of normal and pathological ECGs with detailed corrections (16%).
New ECG teaching method
Baseline students’ characteristics
A total of 52 students from 3 different medical schools were enrolled in our study. Twenty-seven students were assigned to the control group (with 3 subgroups of 7 students each and 1 subgroup of 6 students across the successive internship periods), while 25 students were assigned to the workshop group (with 2 subgroups of 8 students each and 1 subgroup of 9 students). There were no significant differences between the two groups at baseline (Table 1). All students in the control group attended the 2-hour ECG course whereas all students in the workshop group participated in at least fifteen workshops. ECG analysis tests were completed by all students at both baseline and 5-week. The baseline exam results (/ 100) were similar between the groups, with scores of 33 ± 12 for the control group and 36 ± 13 for the workshop group (p = 0.40).
Baseline and 5-week ECG test results
The exam results significantly improved from baseline to 5-week assessment in both groups (control group: 33 ± 12 to 44 ± 12, p < 0.0001; workshop group: 36 ± 13 to 62 ± 12, p < 0.0001 in the). Notably, the improvement was significantly greater in the workshop group as compared to the control group (+ 26 ± 11 vs. + 11 ± 6, p < 0.001) (Graphical Abstract).
The median number of ECG tracings for which students provided a response during the 30-minute test was significantly higher at the final exam compared to the initial test (10, IQR 9–10 vs. 9, IQR 8–10, p < 0.001 in the control group and 10, IQR 10–10 vs. 8, IQR 7–10, p < 0.001 in the workshop group). The increase in the number of ECG tracings for which students provided a response was greater in the workshop group compared to the control group (+ 2, IQR 0–3 vs. + 0, IQR 0–1, p = 0.014) (Fig. 3).

Median number of interpreted ECG tracings during the 30-minute test at baseline and 5-week. Panel A: Workshop group. Panel B: Control group. Lines represent medians
Confidence in ECG reading
There was no significant correlation between baseline confidence in ECG interpretation and baseline exam scores (coefficient correlation of rs = 0.15, p = 0.28 in the overall population; rs = 0.20, p = 0.33 in the workshop group and rs = 0.03, p = 0.87 in the control group). On a Likert scale ranging from 1 (very unconfident) to 5 (very confident), confidence levels in ECG interpretation during routine medical practice and emergency situations significantly improved in both groups during the study period (Fig. 4). While the improvement in routine medical practice did not differ significantly between groups, it was greater in the workshop group compared to the control group in emergency situation (median improvement of 1, IQR 1–2 vs. 0, IQR 0–1, p = 0.012).

Baseline and 5-week level of confidence in ECG interpretation. Panel A and B: Confidence level in ECG interpretation during current medical practice among Workshop (A) and control groups (B). Panel C and D: Confidence level in ECG interpretation during emergency situations among Workshop (C) and control groups (D). Lines represent medians
Discussion
Current state of ECG learning among French medical students
In line with the literature [8], our survey confirmed that students’ confidence in their ability to correctly interpret ECGs is generally low. Confidence levels were even lower in emergency situations, which is problematic as many physicians need to make rapid and important medical decisions based on ECG analysis. Kashou et al.. [9] surveyed over 2,500 American healthcare professionals, 80% of whom reported using ECGs as part of their current practice. Notably, 45% expressed discomfort with ECG interpretation. Inadequacies in training were also exposed as more than 70% received less than 5 h of ECG courses, with 45% reporting no education at all. In another study conducted among internal and emergency medical residents, half of the participants felt their ECG training was inadequate [4]. Although conducted in different countries, those studies clearly highlighted the deficiencies in ECG teaching.
Students’ ECG reading skills are below the expected prerequisites, as evidenced by the baseline exam results (< 40% of correct answers). This pedagogical problem is not confined to French universities [1, 8]. A recent meta-analysis [1] of more than 70 studies (3000 students) showed that the accuracy of ECG interpretation among medical students was 42%, which aligns with our findings. The accuracy remained low among residents (56%) and practicing physicians (69%) [1, 10]. In another study conducted in an American medical school, based on the interpretation of classic examples of ECG tracings with no particular difficulty, the rate of correct answers was 36% among 4th-year medical students and 63% among residents [11]. Despite better results among residents, this level of ECG interpretation remains largely inadequate considering the potential clinical consequences of misinterpretation. In a study of 52 first-year residents, correct identification of complete AV block or ventricular tachycardia was achieved by less than 50% of participants [12].
The current pedagogical methods do not meet students’ expectations and fail to enable them to reach a sufficient level of competence. However, the vast majority of medical students are keen to find innovative educational solutions to improve their ECG interpretation skills [12]. In line with our study, nearly all medical professionals (98%) in Kashou et al. [9] survey expressed a desire for more ECG education.
Could we improve ECG teaching during medical training?
Teaching ECG interpretation is a major challenge in medical education and there is currently no definite method to address the difficulties associated with ECG learning. In a randomized study, Mahler et al. [13] demonstrated that self-directed learning was less effective than other educational approaches, such as workshops or lectures. However, no significant difference was found between the effectiveness of workshops and lectures.
Our study demonstrated that the workshop approach was superior to the more conventional approach routinely used in most of the French University Hospitals. The workshop methods were based on two well-known educational principles: (1) learning by repetition and (2) reverse pedagogy. The improvement of memory retention through repeated exposure to material is one of the most evidenced-based elements of adult learning science. In a study conducted by Cunningham et al.., spaced repetition and retrieval practice of ECG analysis improved ECG interpretation skills [14].
To the best of our knowledge, our study on ECG learning is the first to use the principle of the “reversed classroom”, in which students themselves had to look for ECG tracings within patient files. This pedagogical approach had several advantages. It encouraged students to explore a large number of ECG tracings before the workshop to provide their peers with original educational content. It strengthened interactions between medical students and residents, who helped select and interpret ECGs. Finally, students had to present and explain the analysis and underlying pathophysiology of the selected ECG tracing to their peers; teaching others is a well-known method for enhancing memorization and learning.
Repeated workshops and the reversed approach also stimulated students’ curiosity about ECG analysis, which can be daunting at first. As shown in a study by Berger JS et al. [4], students interested in cardiology performed better in ECG interpretation than those not interested.
Another important concept that may explain the better results in the workshop group is the approach used to interpret ECGs. While the “FRAICH” method seems to be widely taught in France, we observed a switch from this method to the “sequential ECG analysis” approach in the workshop group, which was associated with a significant increase in ECG reading skills. This approach involves step-by-step analysis of the atrial activity, AV nodal conduction properties, ventricular activation and ventricular repolarization, enabled a comprehensive and more logical analysis of ECG tracings. In a study by Zeng et al. [15], the evaluated “sequential ECG analysis” approach reduced the average ECG reading time by a factor of 2, and improved significantly the average ECG accuracy results (77% vs. 43% in the traditional teaching group).
Limitations
Although this was a nonrandomized study, the educational method was assigned according to the centers. A switch from the FRAICH method to the “sequential ECG analysis” method was observed only in the workshop group, which could have also contributed to the main result of our study. However, we cannot exclude the possibility that the repeated workshops and the reverse pedagogy independently influenced the students to change their approach to ECG interpretation.
Conclusion
Our survey on ECG learning highlighted a low level of confidence in ECG interpretation among French medical students. Overall satisfaction with current teaching methods was low, and most students expressed a desire for more ECG training and innovative educational approaches.
Our comparative study revealed that students’ ECG reading skills were initially below the expected level. We found that a workshop approach using a “reversed classroom” method significantly improved ECG interpretation skills compared to conventional lecture-based teaching during cardiology internships. The workshop group showed greater improvements in exam scores and confidence, particularly in emergency situations. These findings suggest that the workshop and “reversed classroom” hold promise for enhancing ECG education. Such methods could be extended to ECG teaching in other medical centers and potentially applied to various other medical topics.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Cook DA, Oh S-Y, Pusic MV. Accuracy of Physicians’ Electrocardiogram interpretations: a systematic review and Meta-analysis. JAMA Intern Med. 2020;180:1461–71.
Mele PF. The ECG Dilemma: guidelines on improving interpretation. J Healthc Risk Manage. 2008;28:27–31.
Kadish AH, Buxton AE, Kennedy HL, Knight BP, Mason JW, Schuger CD, Tracy CM, Boone AW, Elnicki M, Hirshfeld JW, Lorell BH, Rodgers GP, Tracy CM, Weitz HH. ACC/AHA clinical competence statement on electrocardiography and ambulatory electrocardiography. A report of the ACC/AHA/ACP-ASIM Task Force on clinical competence (ACC/AHA Committee to develop a clinical competence Statement on Electrocardiography and Ambulatory Electrocardiography). J Am Coll Cardiol. 2001;38:2091–100.
Berger JS, Eisen L, Nozad V, D’Angelo J, Calderon Y, Brown DL, Schweitzer P. Competency in electrocardiogram interpretation among internal medicine and emergency medicine residents. Am J Med. 2005;118:873–80.
Bogun F, Anh D, Kalahasty G, Wissner E, Bou Serhal C, Bazzi R, Douglas Weaver W, Schuger C. Misdiagnosis of atrial fibrillation and its clinical consequences. Am J Med. 2004;117:636–42.
Pines JM, Perina DG, Brady WJ. Electrocardiogram interpretation training and competency assessment in emergency medicine residency programs. Acad Emerg Med. 2004;11:982–4.
Ginde AA, Char DM. Emergency Medicine Residency Training in Electrocardiogram Interpretation. Acad Emerg Med. 2003;10:738–42.
Vishnevsky G, Cohen T, Elitzur Y, Reis S. Competency and confidence in ECG interpretation among medical students. Int J Med Educ. 2022;13:315–21.
Kashou AH, Noseworthy PA, Beckman TJ, Anavekar NS, Angstman KB, Cullen MW, Sandefur BJ, Friedman PA, Shapiro BP, Wiley BW, Kates AM, Braisted A, Huneycutt D, Baranchuk A, Beard JW, Kerwin S, Young B, Rowlandson I, Knohl SJ, O’Brien K, May AM. Exploring factors influencing ECG interpretation proficiency of medical professionals. Curr Probl Cardiol. 2023;48:101865.
Boltri JM, Hash RB, Vogel RL. Are family practice residents able to interpret electrocardiograms? Adv Health Sci Educ Theory Pract. 2003;8:149–53.
Jablonover RS, Lundberg E, Zhang Y, Stagnaro-Green A. Competency in electrocardiogram interpretation among graduating medical students. Teach Learn Med. 2014;26:279–84.
Eslava D, Dhillon S, Berger J, Homel P, Bergmann S. Interpretation of electrocardiograms by first-year residents: the need for change. J Electrocardiol. 2009;42:693–7.
Mahler SA, Wolcott CJ, Swoboda TK, Wang H, Arnold TC. Techniques for teaching electrocardiogram interpretation: self-directed learning is less effective than a workshop or lecture. Med Educ. 2011;45:347–53.
Cunningham JM, Johnson M, Kincaid T, Christensen W, Baker J, Turbyfill W, Adams JE. The spacing effect: improving electrocardiogram interpretation. Clin Teach 2023:e13626.
Zeng R, Yue R-Z, Tan C-Y, Wang Q, Kuang P, Tian P-W, Zuo C. New ideas for teaching electrocardiogram interpretation and improving classroom teaching content. Adv Med Educ Pract. 2015;6:99–104.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
CC and FA made substantial contributions to the conception, design of the work, acquisition, analysis and interpretation of data and have drafted the work. CM, PO, CB made substantial contributions to the acquisition and interpretation of data. FE, PM, AS, RAH and HE made substantial contributions to the data acquisition and have revised the work. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received approval from educational directors and informed consent was obtained from all participants. Need for ethics approval in educational studies is deemed unnecessary according to national French regulations (Avis n°131 du 7 novembre 2019: Cadre éthique de l’expérimentation pédagogique en situation réelle.)
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chaumont, C., Morgat, C., Ollitrault, P. et al. How to improve medical students’ ECG interpretation skills ? Multicenter survey and results of a comparative study evaluating a new educational approach. BMC Med Educ 24, 979 (2024). https://doi.org/10.1186/s12909-024-05929-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-024-05929-7