
Abstract
Background
Diabetes is a multifactorial disease state that requires adequate patient monitoring for improved health outcomes. Diabetes knowledge and attitude, and associated factors such as medication adherence, medication discrepancy, health literacy, and glycemic control were evaluated in this study. The selected factors were also compared with diabetes knowledge and attitude.
Methods
A cross-sectional study was carried out among ambulatory diabetes patients in three tertiary healthcare facilities in Nigeria. An interviewer-administered semi-structured questionnaire was utilized for data collection. Data was analysed using descriptive and inferential statistics with the level of significance set at p < 0.05.
Results
A total of 188 diabetes patients participated in the study; 51 (27.1%) at the Federal Medical Center, Abeokuta, 69 (36.7%) at the University College Hospital, Ibadan, and 68 (36.2%) at the University of Ilorin Teaching Hospital, Ilorin. One hundred and twelve (59.6%) female patients participated in the study and patients’ average age was 58.69 ± 13.68 years. Medication discrepancy was observed among 101 (53.7%) patients. One hundred and three (54.8%), 47 (25.0%) and 38 (20.2%) had high, medium, and low medication adherence, respectively. Ninety-one (48.4%) had high health literacy. Mean diabetes knowledge score was 14.64 ± 2.55 points out of a maximum obtainable score of 18 points. Mean diabetes attitude of patients was 62.50 ± 6.86 points out of a maximum obtainable score of 70 points. Significant positive association was observed between diabetes knowledge and health literacy (Beta = 0.021, p = 0.029). Diabetes knowledge was higher in patients with higher level of formal education (p = 0.046), higher diabetes attitude (p < 0.001) and high health literacy (p = 0.002). Patients’ diabetes attitude was higher in individuals older than 60 years of age (p = 0.029), and those with high health literacy (p = 0.005).
Conclusions
The diabetes patients displayed good disease knowledge, attitude and medication adherence. Average levels of health literacy and medication discrepancy was observed among the patients. Significant differences were observed between patients’ diabetes knowledge and level of formal education, diabetes attitude, health literacy and age. Patients’ health literacy was significantly associated with diabetes knowledge.
Similar content being viewed by others

Introduction
Diabetes is a foremost reason for death and life expectancy reduction in humans [1,2,3]. It is also a key universal health concern which poses a heavy challenge to public health and socio-economic progress [4]. The prevalence of diabetes is on the increase, especially in low- and middle-income countries [5]. The worldwide burden of diabetes has soared recently, and this trend may continue [2].
Diabetes knowledge includes patients’ understanding of risk factors, worsening factors and complications of diabetes while diabetes attitude involves patients’ thoughts and behavior towards diabetes. There are lots of variables interfering with the management process of diabetes. Disease knowledge and attitude of diabetes patients have been found to impact their disease prognosis and quality of life [6,7,8]. Previous studies in Nigeria reported varying levels of disease knowledge and attitude among this cohort of patients. While a study in North-Western Nigeria reported good diabetes knowledge and attitude [9], another study carried out in the same zone reported a below-average diabetes knowledge and average diabetes attitude [10]. Also, a study in South-Southern Nigeria revealed poor disease knowledge and average attitude displayed by diabetes patients [11] while yet another study in South-Western Nigeria reported good knowledge and attitude among the diabetes patients [12].
Aside from diabetes knowledge and attitude assessment, it is important to evaluate other associated variables such as medication adherence, level of education and health literacy which may play vital roles in disease control. Adequate adherence to medication, diet and exercise are a sine qua non to effective disease control and improved therapeutic outcomes among diabetes patients [13]. Studies have shown a positive association between patients’ level of formal education and diabetes management [9, 14].
Consistent medication adherence plays a major role in glycemic control and in improving health outcomes of patients [15]. Clifford and colleagues [16], in a systematic review, stated that self-report and medication possession ratio are two widely used methods of medication adherence assessment. Another review also reported that medication adherence was associated with better glycemic control, lesser visits to emergency departments, reduced hospitalisations, and reduced medical costs [17]. In addition, the review also identified that health training, point-of-care testing, pharmacists’ involvement, case managers, and phone interventions were some of the factors which enhance patients’ medication adherence.
Health literacy is an important factor for accessing healthcare and making informed health-related decisions [18]. Inadequate health literacy is related to poor health outcomes, inefficient access to healthcare services and inadequate understanding of health-related information [19]. Association between health literacy level and medication discrepancies were reported by previous studies [20]. High health literacy has been reported to increase glycemic control in diabetes patients [21].
However, there is dearth of literature on comparing disease knowledge and attitude among ambulatory type 2 diabetes patients and the related factors in Nigeria. Also, the interactions between the variables could have important implications for consideration by healthcare professionals. Therefore, this study assessed associations and comparison of diabetes knowledge and attitude with selected variables such as medication adherence, medication discrepancy, glycemic control and health literacy.
Methods
Study design, setting and participants
A cross-sectional study was carried out in three tertiary healthcare facilities in Nigeria. The study sites were the University College Hospital, Ibadan (950-bed healthcare facility), the University of Ilorin Teaching Hospital, Ilorin (650-bed healthcare facility), and the Federal Medical Center, Abeokuta (250-bed healthcare facility). These healthcare facilities are key referral centers and accredited for undergraduate and postgraduate education for pharmacists, physicians, physiotherapists, nurses, and other healthcare practitioners. Ambulatory diabetes patients above eighteen years of age who were on at least one medication for diabetes were recruited for the study. Patients who were unconscious, pregnant or did not give their consent were excluded from the study.
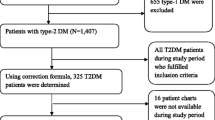
Sample size calculation was based on disease prevalence [22] which according to the International Diabetes Federation is 3.7% in Nigeria [23]. With 5% precision and 95% confidence interval, the minimum sample size for each study center was 55 patients, making 165 in total. 10% nonresponse rate was factored in to make a total of 188 patients.
Data collection tools
The diabetes knowledge and attitude assessment scales for patients were developed by the authors sequel to extensive literature search. The diabetes knowledge assessment scale is an 18-item scale with three options – “yes”, “no” and “don’t know”. Each correct response was assigned “1” point while each incorrect response was assigned “0” point. The diabetes attitude assessment scale is a 14-item scale with a Likert response ranging from ‘strongly disagree’ to ‘strongly agree’. The Likert responses were assigned one to five points based on the expected response to questions asked. Both scales were subjected to content validation by four faculties in the Department of Clinical Pharmacy and Pharmacy Administration, Faculty of Pharmacy, University of Ibadan. Face validation was done by pretesting the scales among twenty ambulatory diabetes patients at Catholic Hospital, Oluyoro in Ibadan. Cronbach Alpha reliability test was conducted to ascertain the internal consistency of the knowledge and attitude scales. Cronbach alpha for diabetes knowledge and attitude assessment scales were 0.70 and 0.83, respectively. Each participant’s scores for both scales were summed, converted to percentages, and categorized as follows: poor = 0–49.9%, fair = 50–69.9%, good = 70–89.9%, and excellent ≥ 90%.
The validated 18-item Short Assessment Health Literacy–English (SAHL-E) scale was utilised for patients’ health literacy evaluation [24]. Patients with 0–14 points were categorized to have low health literacy and those with 15–18, high health literacy. Patients’ self-reported medication adherence was evaluated using the validated 4-item Morisky, Levine, Green scale [25] used with permission from Professor Donald E. Morisky. Responses were coded “yes” and assigned a score of “0” while “no” was assigned a score of “1”. High adherence was defined as a total score of zero, medium adherence as 1 and low adherence as > 1.
Medication reconciliation was carried out for the recruited patients. Information on whether or not they had their medication packs with them was noted. Medication discrepancies, defined as inconsistencies between prescribed medications, including the dosage regimen and the medications taken by the patients [26], were also documented. For the purpose of this study, geriatric patients were ≥ 60 years.
The semi-structured questionnaire was divided into five sections. Sections A was for sociodemographic data, while Sections B to E were for diabetes knowledge, diabetes attitude, health literacy and medication adherence assessments, respectively. The participants were approached while waiting to see their physicians on clinic days. The purpose of the study was explained to them before their informed consent was obtained. The questionnaire, which took about 20–30 min to complete, was then administered to the patients who were consecutively sampled. The questionnaire was translated to Yoruba language (the local language) for patients who did not understand English language.
Glycemic control was defined as a fasting blood glucose ranging from 70 to 130 mg/dL [27]. Fasting blood glucose value at the clinic on the day of clinic appointment was documented.
Data analysis
Data was analyzed using SPSS for Windows Version 20.0 (IBM Corp, New York, USA). Descriptive statistics was summarized with frequency counts, percentages, and mean ± standard deviation. Negatively worded questions were reversed during analysis.
Standard multiple regression analysis was carried out to assess associations between diabetes knowledge and attitude with gender, medication discrepancy, educational qualification, health literacy, age, glycemic control, and medication adherence. Independent-samples t-test evaluated the difference between means scores of patients’ diabetes knowledge and attitude scores among categorical variables such as gender, health literacy, glycemic control and medication discrepancy. One-way analysis of variance compared patients’ diabetes knowledge and attitude with level of formal education and medication adherence.
Results
A total of 188 diabetes patients, 51 (27.1%) at Federal Medical Center, Abeokuta, 69 (36.7%) University College Hospital, Ibadan, and 68 (36.2%) University of Ilorin Teaching Hospital, Ilorin participated in the study. There were 112 (59.6%) females who participated in the study. Mean age of the patients was 58.69 ± 13.68 years. Further details on participants’ sociodemographic characteristics are shown in Table 1. Medication discrepancy was observed among 101 (53.7%) patients. Self-reported medication adherence of the participants showed that 103 (54.8%), 47 (25.0%) and 38 (20.2%) had high, medium and low medication adherence, respectively. Ninety-one (48.4%) were found to have high health literacy while 97 (51.6%) had low health literacy.
Majority, 167 (88.8%) knew that diabetes is not contagious. Only 52 (27.7%) knew that untreated diabetes does not lead to typhoid fever. One hundred and twenty-six (67.0%) knew that diabetes is incurable. Average diabetes knowledge score was 14.64 ± 2.55 out of a maximum obtainable score of 18. Majority of the patients, 91 (48.4%) and 61 (32.4%) had “good” and “excellent” diabetes knowledge score, respectively (Table 2). Eighty-five (45.2%) participants strongly disagreed with the statement that “It is not important to have a self-monitoring blood glucose meter”. One hundred and sixty-nine (89.9%) believed strongly that taking their medications would make them live long. Majority, 53 (28.2%) and 126 (67.0%) had “good” and “excellent” attitude to diabetes, respectively. A mean score of 62.50 ± 6.86 out of a maximum obtainable score of 70 was obtained for diabetes attitude assessment (Table 3). Cronbach alpha for diabetes knowledge and attitude assessment scales were 0.70 and 0.83, respectively.
Participants’ diabetes knowledge was higher among those with higher level of formal education (p = 0.046), higher diabetes attitude (p < 0.001) and high health literacy (p = 0.002). For diabetes attitude, individuals older than 60 years of age (p = 0.029), with higher diabetes knowledge (p < 0.001) and high health literacy (p = 0.005) had significantly higher values.were significantly different Details on the comparisons between diabetes knowledge and attitude with some selected variables are given in Table 4. Significant positive association was observed between diabetes knowledge and health literacy (Beta = 0.021, p = 0.029) (Table 5).
Discussion
The study revealed significant associations between type 2 diabetes patients’ diabetes knowledge and health literacy. Significant differences were observed between disease knowledge and educational level, disease attitude and health literacy, while disease attitude was significantly different when compared with age and disease knowledge. Disease knowledge, attitude, level of formal education, health literacy, patient’s age, number of medications taken by patients, medication adherence, medication discrepancy, and glycemic control were all evaluated in this study. It is important to consider these variables during the management of diabetes patients to achieve better health outcomes.
Majority of the patients had good diabetes knowledge with only two having less than 50% knowledge score. While a study carried out in North-western Nigeria had a similar observation [9], on the contrary, other studies in North-Western [10], and South-Southern Nigeria [11] reported poor diabetes knowledge among diabetes patients. While patients’ knowledge in the study is commendable, there is need for regular knowledge update. Also, another study in South-Western Nigeria reported good knowledge and attitude among the diabetes patients [12]. Many studies carried out in other developing nations such as Bangladesh, Ethiopia Mongolia and Zimbabwe observed inadequate knowledge of diabetes among patients [28,29,30,31]. Studies carried out in Bangladesh [32], and Sri Lanka [33] and the United Arab Emirates [34] however reported good diabetes knowledge among majority of the patients. It is worthy to note that different diabetes knowledge assessment tools were used for these studies.
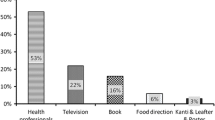
Dearth of effectively trained healthcare practitioners is a factor that might be responsible for the poor diabetes knowledge among the patients [10, 35]. Healthcare practitioners need to consistently educate patients on diabetes-related knowledge as it is vital in diabetes management [36]. In the study setting, diabetes patients are jointly educated by nurses on each clinic appointment before their appointment with the physicians. The ambulatory diabetes patients also have association in each hospital, where they come together monthly for peer group discussion. Peer support has been found to aid learning and adaptations for self-management among diabetes patients [37, 38], thereby complementing information provided by the physicians on self-management of the disease.
Interestingly, two thirds of the participants believed that taking “bitters” such as Swedish bitters helps to reduce blood sugar. There is a general belief that bitters could be good for elevated blood sugar level. A study carried out in India and another in Saudi Arabis reported the misconception among diabetes patients [39, 40]. Some diabetes patients may rely on these preparations instead of adequately adhering to the prescribed medications thereby worsening their disease condition. Also, about 15% believed that herbal remedies were more effective than prescribed medications at managing blood glucose level. It will not be a surprise if this 15% abandon their medications for herbal remedies. Consumption of herbal remedies could lead to diabetic kidney disease which in turn could affect glycemic control [41].
With a third of the study participants not knowing that diabetes is incurable, and that they will have to be on medications indefinitely, the need for improved patient education becomes glaring. Patients need to be educated on the fact that they will be on medications indefinitely. Some patients have been known to stop their medications once they feel better [42, 43] and stopping the medications could predispose to developing complications of diabetes.
Some of the participants were not aware that obesity is a risk factor for diabetes. For diabetes, adequate adherence to exercise, diet and medications is required for improved patient outcomes. Obesity causes insulin resistance [44] and there is need for patients to be aware of it. Also, some of the participants were not aware that diabetes could be genetic, and this may expose their offspring to higher risks. Such children could be educated by their parents to minimize their risks for type 2 diabetes.
On the other hand, almost of the participants were knowledgeable about diet requirement and exercise. Although, such knowledge of such health benefits does not guarantee adherence to the practice, it places the patient at a good vantage. Many of the patients were also aware of the complications of diabetes such as blindness and kidney disease. However, some of them believed that diabetes could lead to typhoid fever.
Level of formal education, diabetes attitude and health literacy were associated with diabetes knowledge in this study. As expected, patients with high health literacy, better diabetes attitude, as well as those with higher formal educational qualification had better diabetes knowledge. Level of formal education was significantly associated with diabetes knowledge and attitude [11]. A related study in Netherland observed a significant association between poor diabetes knowledge and attitude [45]. Herath and colleagues in Sri Lanka [33], Gautam and colleagues in Nepal, Salem and colleagues in Riyadh, and Phoosuwan and colleagues in Thailand observed better diabetes knowledge among patients with higher educational level [46,47,48].
Average health literacy was observed among the patients. Level of formal education was significantly different with health literacy level. Teach back technique is a method that would help to simplify communications, where patients are asked to explain what they were told by healthcare practitioners in their own words [49]. It helps to address low health literacy.
Majority of patients displayed good attitude towards diabetes. This is similar to the study by Sadiq et al. in North-Western Nigeria [9], but unlike what was reported among diabetes patients in North-western Nigeria where poor attitude was reported [10]. Diabetes attitude was found to be poor among majority of patients in a study carried out in Sri Lanka [33], and average in Palestine [50]. While majority of the diabetes patients displayed excellent attitude in this study, it is needful to keep educating them in order to encourage positive attitudes and not resign to fate or other alternative practices.
There was no significant association observed in this study between diabetes knowledge and medication adherence. A cross-sectional studied carried out among diabetes patients also reported no significant association between diabetes knowledge and medication adherence [51]. High medication adherence was observed among majority of the patients. Medication adherence was not found to be significantly different when compared with age, educational level, diabetes knowledge or attitude. Even though polypharmacy, due to comorbidities, is a risk for poor medication adherence, the present study and a similar study [52] showed that medication adherence for diabetes patients does not decline with increase in medications taken.
Glycemic control had no significant association with diabetes knowledge and attitude in this study. Another study carried out in Enugu State, Nigeria also found no significant association between diabetes attitude and glycemic control but found a significant association between diabetes knowledge and glycemic control [53]. Glycemic control was significantly different with patients’ age, medication adherence and level of formal education. Geriatric patients are more likely to have comorbidities that could impact on their glycemic control. However, the geriatric patients in this study showed a significantly better attitude to diabetes which could explain their better glycemic control, despite the likelihood of comorbidities. Similar studies also reported that glycemic control was associated with formal education and medication adherence [54, 55]. However, a study by Al-Rasheedi found no association between glycemic control and level of educational qualification [56].
A major limitation to this study was that glycemic control was assessed using fasting blood glucose instead of glycated hemoglobin (HbA1c) which is the gold standard. Also, data on level of income and duration of diabetes were not included in the study.
Conclusion
The diabetes patients displayed good disease knowledge and attitude. Level of health literacy and medication discrepancy was average among the patients, while a high proportion showed high medication adherence. Patients’ health literacy was significantly positively associated with diabetes knowledge. The determinants of diabetes knowledge are level of formal education, diabetes attitude, health literacy, and age; while the determinants of diabetes attitude are health literacy, age and diabetes knowledge.
While the patients displayed good disease knowledge and attitude, it is important to ensure that this does not decline. The average level of health literacy should be put into consideration when passing medical information to the patients so as to ensure that they are able to appropriately interpret and comprehend the instructions.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- SAHL-E:
-
Short Assessment Health Literacy–English
- SPSS:
-
Statistical Package for Social Sciences
References
Secrest AM, Washington RE, Orchard TJ et al. Mortality in Type 1 Diabetes. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 35.
Lin X, Xu Y, Pan X, Xu J, Ding Y, Sun X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. https://doi.org/10.1038/s41598-020-71908-9. Published 2020 Sep 8.
Tönnies T, Baumert J, Heidemann C, von der Lippe E, Brinks R, Hoyer A. Diabetes free life expectancy and years of life lost associated with type 2 diabetes: projected trends in Germany between 2015 and 2040. Popul Health Metrics. 2021;19:38. https://doi.org/10.1186/s12963-021-00266-z.
Mohamed SF, Mwangi M, Mutua MK, Kibachio J, Hussein A, Ndegwa Z, et al. Prevalence and factors associated with pre-diabetes and diabetes mellitus in Kenya: results from a national survey. BMC Public Health. 2018;18(Suppl 3):1215. https://doi.org/10.1186/s12889-018-6053-x. Published 2018 Nov 7.
World Health Organisation. 2021. Diabetes key facts. Date accessed May 17, 2022. https://www.who.int/news-room/fact-sheets/detail/diabetes
Al-Aboudi IS, Hassali MA, Shafie AA. Knowledge, attitudes, and quality of life of type 2 diabetes patients in Riyadh, Saudi Arabia. J Pharm Bioallied Sci. 2016;8(3):195–202. https://doi.org/10.4103/0975-7406.171683.
Fatema K, Hossain S, Natasha K, Chowdhury HA, Akter J, Khan T, Ali L. Knowledge attitude and practice regarding diabetes mellitus among nondiabetic and diabetic study participants in Bangladesh. BMC Public Health. 2017;17:364. https://doi.org/10.1186/s12889-017-4285-9.
Le NK, Turnbull N, Van Dam C, Khiewkhern S, Thiabrithi S. Impact of knowledge, attitude, and practices of type 2 diabetic patients: a study in the locality in Vietnam. J Educ Health Promot. 2021;10:72. https://doi.org/10.4103/jehp.jehp_712_20.
Sadiq AA, Hanif SM, Muhammad DG. Assessment of knowledge, attitude, practice, and barriers to lifestyle modification among individuals with diabetes mellitus in Kano Nigeria. Adesh Univ J Med Sci Res. 2021;3:100–7.
Muhammad FY, Iliyasu G, Uloko AE, Gezawa ID, Christiana EA. Diabetes-related knowledge, attitude, and practice among outpatients of a tertiary hospital in North-western Nigeria. Ann Afr Med. 2021;20(3):222–7. https://doi.org/10.4103/aam.aam_48_20.
Aniedi UV, Effiong JH, Akpan EE. Knowledge, attitudes and practices on diabetes mellitus among out-patients with type 2 diabetes in Uyo, South-South Nigeria. J Med Sc Cli Res. 2020;8(11):423–30.
Adetona IO, Ogbo PU, Aina BA. Knowledge and attitude towards Diabetes Mellitus among residents of Igbo-Ora, a Rural Community in South-Western Nigeria. Nigeria J Pharm. 2019;53(2):38–47.
Mirahmadizadeh A, Khorshidsavar H, Seif M, Sharifi MH. Adherence to Medication, Diet and Physical Activity and the Associated factors amongst patients with type 2 diabetes. Diabetes Ther. 2020;11(2):479–94. https://doi.org/10.1007/s13300-019-00750-8.
Tadesse E, Adem AM, Gelaw BK, Ahmed M, Seifu MF, Thirumurugan G. Assessment of knowledge, attitude and practices regarding life style modification among type 2 diabetic mellitus patients attending Adama hospital medical college, Oromia region, Ethiopia. Glob J Med Res. 2014;14:7.
Krass I, Schieback P, Dhippayom T. Adherence to diabetes medication: a systematic review. Diabet Med. 2015 32(6):725 – 37. https://doi.org/10.1111/dme.12651. PMID: 25440507.
Clifford S, Perez-Nieves M, Skalicky AM, Reaney M, Coyne KS. A systematic literature review of methodologies used to assess medication adherence in patients with diabetes. Curr Med Res Opin. 2014;30:1071–85.
Capoccia K, Odegard PS, Letassy N. Medication adherence with diabetes medication: a systematic review of the literature. Diabetes Educ. 2016;42(1):34–71. https://doi.org/10.1177/0145721715619038. Epub 2015 Dec 4. PMID: 26637240.
Woudstra AJ, Meppelink CS, Pander Maat H, Oosterhaven J, Fransen MP, Dima AL. Validation of the short assessment of health literacy (SAHL-D) and short-form development: Rasch analysis. BMC Med Res Methodol. 2019;19(1):122. https://doi.org/10.1186/s12874-019-0762-4. Published 2019 Jun 14.
Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107. https://doi.org/10.7326/0003-4819-155-2-201107190-00005.
Persell SD, Osborn CY, Richard R, Skripkauskas S, Wolf MS. Limited health literacy is a barrier to medication reconciliation in ambulatory care. J Gen Intern Med. 2007;22(11):1523–6. https://doi.org/10.1007/s11606-007-0334-x.
Saleh A, Wirda W, Irwan AM, Latif AI. The relationships among self-efficacy, health literacy, self-care and glycemic control in older people with type 2 diabetes mellitus. Working Older People. 2021;25(2):164–9.
Sampsize. (2019). http://sampsize.sourceforge.net/iface/
Diabetes in Nigeria. 2021. https://idf.org/our-network/regions-and-members/africa/members/nigeria/
Personal Health Literacy Measurement Tools. Agency for Healthcare Research and Quality, Rockville, MD. https://www.ahrq.gov/health-literacy/research/tools/index.html
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74.
Abu Farha R, Yousef A, Gharaibeh L, Alkhalaileh W, Mukattash T, Alefishat E. Medication discrepancies among hospitalized patients with hypertension: assessment of prevalence and risk factors. BMC Health Serv Res. 2021;21(1):1338. https://doi.org/10.1186/s12913-021-07349-5. PMID: 34903221; PMCID: PMC8670213.
Bin Rakhis SA, Sr, AlDuwayhis NM, Aleid N, AlBarrak AN, Aloraini AA. Glycemic Control for type 2 diabetes Mellitus patients: a systematic review. Cureus. 2022;14(6):e26180. https://doi.org/10.7759/cureus.26180. Published 2022 Jun 21.
Demaio AR, Otgontuya D, de Courten M, Bygbjerg IC, Enkhtuya P, Oyunbileg J, et al. Exploring knowledge, attitudes and practices related to diabetes in Mongolia: a national population-based survey. BMC Public Health. 2013;13:236.
Fottrell E, Ahmed N, Shaha SK, Jennings H, Kuddus A, Morrison J, et al. Diabetes knowledge and care practices among adults in rural Bangladesh: a cross-sectional survey. BMJ Glob Health. 2018;3:e000891. https://doi.org/10.1136/bmjgh-2018-000891.
Mufunda E, Ernersson Å, Hjelm K. Limited knowledge of diabetes in patients attending an outpatient diabetes clinic at a referral hospital in Zimbabwe: a cross-sectional study. Pan Afr Med J. 2018;29:144. https://doi.org/10.11604/pamj.2018.29.144.12301. Published 2018 Mar 5.
Kifle ZD, Adugna M, Awgichew A, Chanie A, Sewnet G, Asrie AB. Knowledge towards diabetes and its chronic complications and associated factors among diabetes patients in University of Gondar comprehensive and specialized hospital, Gondar, Northwest Ethiopia. Clin Epid Gl Health. 2022;15. https://doi.org/10.1016/j.cegh.2022.101033.
Saleh F, Mumu SJ, Ara F, Begum HA, Ali L. Knowledge and self-care practices regarding diabetes among newly diagnosed type 2 diabetics in Bangladesh: a cross-sectional study. BMC Pub Health. 2012;12:1112.
Herath HMM, Weerasinghe NP, Dias H, Weerarathna TP. Knowledge, attitude and practice related to diabetes mellitus among the general public in Galle district in Southern Sri Lanka: a pilot study. BMC Pub Health. 2017;17:535. https://doi.org/10.1186/s12889-017-4459-5.
Al-Maskari F, El-Sadig M, Al-Kaabi JM, Afandi B, Nagelkerke N, Yeatts KB. Knowledge, attitude and practices of diabetic patients in the United Arab Emirates. PLoS ONE. 2013;8(1):e52857.
Tella EE, Yunusa I, Hassan JH, Chindo IA, Oti VB, Prevalence. Contributing factors and management strategies (self-Management education) of type 2 diabetes patients in Nigeria: a review. Int J Diabetes Clin Res. 2021;8:148. https://doi.org/10.23937/2377-3634/1410148.
Zhou W, Huang J, Yang L, Qiu T, Zhang Y, Liu F, Zhou Z. Long-term training in diabetes-related knowledge, attitudes, and self-reported practice among diabetes liaison nurses. J Int Med Res. 2020;48(2):300060519882838. https://doi.org/10.1177/0300060519882838. Epub 2019 Oct 29. PMID: 31662018; PMCID: PMC7873921.
Aziz Z, Riddell MA, Absetz P, Brand M, Oldenburg B. Australasian Peers for Progress Diabetes Project investigators. Peer support to improve diabetes care: an implementation evaluation of the Australasian Peers for Progress Diabetes Program. BMC Pub Health. 2018;18:262. https://doi.org/10.1186/s12889-018-5148-8.
Azmiardi A, Murti B, Febrinasari RP, Tamtomo DG. The effect of peer support in diabetes self-management education on glycemic control in patients with type 2 diabetes: a systematic review and meta-analysis. Epidemiol Health. 2021;43:e2021090. https://doi.org/10.4178/epih.e2021090.
Patil R, Nasrin AN, Datta SS, Boratne AV, Lokeshmaran. Popular misconceptions regarding the diabetes management: where should we focus our attention? J Clin Diagn Res. 2013;7(2):287–91. https://doi.org/10.7860/JCDR/2013/4416.2749. Epub 2013 Feb 1. PMID: 23542645; PMCID: PMC3592294.
Alsunni A, Albaker W, Badar A. Determinants of misconceptions about diabetes among Saudi diabetic patients attending diabetes clinic at a tertiary care hospital in Eastern Saudi Arabia. J Family Community Med. 2014;21(2):93. https://doi.org/10.4103/2230-8229.134764.
Mardani S, Nasri H, Rafieian-Kopaei M, Hajian S. Herbal medicine and diabetic kidney disease. J Nephropharmacol. 2013;2(1):1–2. PMID: 28197432; PMCID: PMC5297466.
Al-Qerem W, Jarab AS, Badinjki M, Hyassat D, Qarqaz R. Exploring variables associated with medication non-adherence in patients with type 2 diabetes mellitus. PLoS ONE. 2021;16(8):e0256666. https://doi.org/10.1371/journal.pone.0256666.
Nadery Y, Khorasani P, Feizi A, Parvizy S. Causes of nonadherence to treatment in people with myocardial infarction: content analysis. J Educ Health Promot. 2021;10:330. https://doi.org/10.4103/jehp.jehp_92_21.
Wondmkun YT, Obesity. Insulin resistance, and type 2 diabetes: associations and therapeutic implications. Diabetes Metab Syndr Obes. 2020;13:3611–6. https://doi.org/10.2147/DMSO.S275898.
van der Heide I, Uiters E, Rademakers J, Struijs JN, Schuit AJ, Baan CA. Associations among health literacy, diabetes knowledge, and self-management behavior in adults with diabetes: results of a Dutch cross-sectional study. J Health Commun. 2014;19(Suppl):115–31.
Gautam A, Bhatta DN, Aryal UR. Diabetes related health knowledge, attitude and practice among diabetic patients in Nepal. BMC Endocr Disord. 2015;5:15:25. https://doi.org/10.1186/s12902-015-0021-6. PMID: 26045031; PMCID: PMC4456997.
Salem A, Majed A, Mustafa M, Abdulsalam A, Asdaq S, Mohammed A. Knowledge, attitude, and practice regarding diabetes mellitus among general public and diabetic patients in Riyadh, Saudi Arabia. Asian J Pharm. 2018;12:268–76.
Phoosuwan N, Ongarj P, Hjelm K. Knowledge on diabetes and its related factors among the people with type 2 diabetes in Thailand: a cross-sectional study. BMC Pub Health. 2022;22:365. https://doi.org/10.1186/s12889-022-14831-0.
Griffey RT, Shin N, Jones S, Aginam N, Gross M, Kinsella Y, et al. The impact of teach-back on comprehension of discharge instructions and satisfaction among emergency patients with limited health literacy: a randomized, controlled study. J Commun Healthc. 2015;8(1):10–21. https://doi.org/10.1179/1753807615Y.0000000001.
Shawahna R, Samaro S, Ahmad Z. Knowledge, attitude, and practice of patients with type 2 diabetes mellitus with regard to their disease: a cross-sectional study among palestinians of the West Bank. BMC Public Health. 2021;21:472. https://doi.org/10.1186/s12889-021-10524-2.
Muhammad Haskani NH, Goh HP, Wee DVT, Hermansyah A, Goh KW, Ming LC. Medication knowledge and adherence in type 2 diabetes Mellitus patients in Brunei Darussalam: A Pioneer Study in Brunei Darussalam. Int J Environ Res Public Health. 2022;19(12):7470. https://doi.org/10.3390/ijerph19127470. PMID: 35742719; PMCID: PMC9224316.
Adisa R, Fakeye TO, Fasanmade A. Medication adherence among ambulatory patients with type 2 diabetes in a tertiary healthcare setting in southwestern Nigeria. Pharm Pract. 2011;9(2):72–81.
Anakwue RC, Young EE, Ezenduka CC, Okoli CI, Maduforo AN, Nnakenyi ID, et al. Assessment of patients’ knowledge and attitude towards diabetes and its relationship with glycemic control: a cross-sectional study in a Nigerian tertiary hospital. Niger J Med. 2019;28(1):46–55.
Khattaba Maysaa K, Yousef S, Al-Khawaldehd, Abdelkarim, Ajlounid Kamel. Factors associated with poor glycemic control among Jordanian patients with type 2 diabetes. J Diabetes Complicat. 2010;24:84–9.
Khan AR, Al-Abdul Lateef ZN, Al Aithan MA, Bu-Khamseen MA, Al Ibrahim I, Khan SA. Factors contributing to non-compliance among diabetics attending primary health centers in the Al Hasa district of Saudi Arabia. J Family Community Med. 2012 Jan-Apr;19(1):26–32.
Al-Rasheedi AA. The role of Educational Level in Glycemic Control among patients with type II diabetes Mellitus. Int J Health Sci (Qassim). 2014;8(2):177–87. https://doi.org/10.12816/0006084.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Dr. Akinniyi A. Aje: Principal investigator and corresponding author. Contributions: Study design, data collection and analysis, manuscript writing. Professor Titilayo O. Fakeye: Study design, manuscript review.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval for the study was granted by the Federal Medical Center, Abeokuta Health Research Ethics Committee (FMCA/470/HREC/06/2014), the University of Ilorin Teaching Hospital Ethics Research Committee (ERC/PAN/2018/08/1814) and the joint University of Ibadan/University College Hospital Health Research and Ethics Committee (UI/EC/15/0308). The study was explained to the type 2 diabetes patients. Informed consent to participate was obtained from the participants included in this study. Only those who gave informed consent were recruited for this study. The research was carried out in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Aje, A.A., Fakeye, T.O. Factors associated with disease knowledge and attitude among ambulatory patients with type 2 diabetes – a multicenter study. BMC Endocr Disord 24, 158 (2024). https://doi.org/10.1186/s12902-024-01696-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-024-01696-0