
Abstract
Background
Considering the high prevalence of polycystic ovary syndrome (PCOS) in women of reproductive age and the metabolic disorders associated with it, this study was conducted to determine the effects of curcumin on metabolic indices and androgen level (primary outcomes), and menstruation characteristics, and hirsutism (secondary outcomes) in women with PCOS.
Methods
This triple-blind randomized controlled trial was conducted on women with PCOS who visited the health centers at Eslamshahr County (Tehran Province-Iran) from 2020 to 2022. The participants were allocated into two groups (curcumin and placebo) using block randomization method. The treatment group received two 500 mg edible curcumin tablets together at the same time per day for twelve weeks while the control group received placebo tablets similar to curcumin. Biochemical parameters such as Fasting Blood Insulin (FBI), Fasting Blood Sugar (FBS), triglyceride, total cholesterol, Low Density Lipoprotein- cholesterol (LDL-C), High Density Lipoprotein- cholesterol (HDL-C) were measured before intervention and then 3 months after the intervention. Sex Hormone Binding Globulin (SHBG) and testosterone serum levels were measured 3 months after the intervention. Questionnaires regarding the menstrual cycle characteristics and the Ferriman–Gallwey score were also filled for evaluating hirsutism before the intervention as well as 3 months after the intervention. The independent t-test, Mann-Whitney U test, and ANCOVA were used to analyze the data.
Results
There was no statistically significant difference between the two groups in terms of socio-demographic and the baseline levels of measured outcomes. After 12 weeks of intervention, the mean serum FBS levels in the curcumin group were significantly lower than in the placebo group (mean difference: 6.24; 95%confidence interval: -11.73 to -0.76; P = 0.027) but there was no significant difference between the two groups in terms of triglyceride (P = 0.351), cholesterol (P = 0.528), LDL (P = 0.064), HDL (P = 0.306), FBI (p = 0.929), SHBG (p = 0.682), and testosterone (p = 0.133) serum levels. After the intervention, amenorrhea and oligomenorrhea frequency in the curcumin group was significantly lower than in the placebo group (13% vs. 22%, P = 0.038). There was no significant difference in terms of duration of menstruation (P = 0.286) and hirsutism (P = 0.630) between the two groups.
Conclusion
Curcumin decreased FBS levels and improved menstruation characteristics (amenorrhea, oligomenorrhea, and menstrual irregularities) in women with PCOS but did not affect other metabolic, hormonal, and hirsutism indices. More studies using a larger sample size are required for a definitive conclusion.
Trial registration
Iranian Registry of Clinical Trials (IRCT): IRCT20120718010324N51 Date of registration: 30/11/2019. URL: https://en.irct.ir/user/trial/40597/view; Date of first registration: 30/11/2020.
Similar content being viewed by others


Background
Polycystic ovary syndrome (PCOS), also known as metabolic syndrome or insulin resistance syndrome [1, 2], is a common endocrine and metabolic disorder among women [3] and is a series of symptoms related to hormonal imbalance [4]. This hormonal imbalance causes irregularities in ovulation that could lead to the formation of small cysts in the ovary [5]. This syndrome is the most common hormonal disorder in women [6] and is seen in 4–6% of women of reproductive age. Studies suggest an increase in this syndrome [6]. The prevalence of PCOS among Iranian women is reported to be between 7.1 and 14.6% [7].
Many of the systems in the body are affected by PCOS which leads to several complications such as menstrual disorders, infertility, hirsutism, acne, obesity and metabolic syndrome [8], increase in LH levels, slight decrease or lack of change in FSH levels, a slight increase in prolactin, increase in estradiol and estrogen levels, possible increase in dehydroepiandrosterone sulfate (DHEAS), androstenedione, and testosterone, and decrease in sex hormone-binding globulin (SHBG) levels [9]. Metabolic disorders are seen in women with PCOS include resistance to insulin, hyperinsulinemia, and dyslipidemia (decrease in High Density Lipoprotein- cholesterol (HDL-C), increase in total cholesterol, Low Density Lipoprotein- cholesterol (LDL-C), and triglycerides), so we can say that women with PCOS are prone to type 2 diabetes and cardiovascular diseases [10]. Insulin’s role in PCOS is to regulate the activities of ovary and liver enzymes that have a role in the production of androgen and low-grade inflammation, respectively. Reportedly, insulin resistance usually leads to problems such as dyslipidemia as well as cardiovascular and metabolic diseases [11].
PCOS pathogenesis are still unknown but studies show that PCOS has a complicated and multi-factor cause that stems from the interaction of genetic, environmental, and intrauterine factors [12]. Currently, there is no cure for PCOS and as treatment, women with PCOS are only recommended to change their lifestyle [13]. Most of these interventions focus on changing eating habits, physical activity, and losing weight [14, 15]. However, new studies in the field of medicinal herbs and complementary therapy have shown promising results in curing PCOS.
Curcumin is a polyphenol derived from the curcuma longa species and traditionally can be found in Asian food [16]. Recently curcumin was studied as supportive therapy for a wide range of diseases such as type 2 diabetes which is one of the complications of PCOS [17]. Based on a study on animals, curcumin can be effective in improving insulin sensitivity and decreasing CRP and IL-6 levels [18]. Moreover, it was reported in a study on humans that the edible intake of curcumin led to a significant decrease in FBS, HOMA-IR, HbA1c, triglycerides, and total cholesterol levels in patients with metabolic diseases.
As seen in animal experiments, the use of curcumin can lead to a decrease in insulin resistance (one of the key features of PCOS phenotype), a decrease in blood’s inflammatory factors such as CRP and IL-6 [18] (which are high in people with PCOS and have a direct relationship with insulin sensitivity [19], a decrease in FBS and cholesterol levels in people with metabolic disorders (complications of PCOS) [20], but the administration of curcumin can lead to improvement in insulin sensitivity, cholesterol levels and metabolic factors in people with PCOS as well. So, this study was conducted to determine the effects of curcumin on metabolic indices and androgen level (primary outcomes), menstruation characteristics and hirsutism (secondary outcomes) in women with PCOS.
Methods
Study design and setting
This study was a superiority randomized controlled trial with two-parallel arms. The participants, researcher, and analyst in this study were blinded to the intervention received by the participants. This study was conducted in the health centers at Eslamshahr County (Tehran Province-Iran) from 2020 to 2022.
Eligibility criteria
The study was conducted on women aged 18 to 45 with PCOS and a BMI of 18.5 to 40. The exclusion criteria were as follows: taking vitamins, contraceptives, hormonal drugs, minerals, and omega-3 during the study and 3 months before intervention; having other metabolic diseases such as diabetes and androgenic disorders such as congenital adrenal hyperplasia (CAH) or androgen-producing glands; thyroid gland diseases; Cushing syndrome; pregnancy or breastfeeding; prior surgery on one or both ovaries; smoking and alcohol consumption.
Sampling
Sampling started after the approval of the ethics committee of Tabriz University of Medical Sciences (Ethics code: IR.TBZMED.REC.1398.017) and registering the study in Iranian Registry of Clinical Trials (IRCT) (Code: IRCT20120718010324N51). The researcher attended at the health centers in the Eslamshahr city and searched for women with eligible criteria and willingness to participate in the study. They were surveyed based on Rotterdam criteria (the presence of two of the three criteria is enough to diagnose PCOS) which include oligomenorrhea (i.e., a menstrual cycle that lasts more than 35 days or having four to nine cycles each year) [21] or lack of ovulation, clinical and laboratory signs and symptoms of hyperandrogenism, and polycystic ovary.
After PCOS was confirmed, written consent is obtained in case of the patient’s willingness to participate in the study and questionnaires regarding socio-demographic and menstrual cycle characteristics were completed. A food consumption frequency questionnaire was also provided to the participants to record their average annual food consumption. The hirsutism score of the participants was determined by the researcher using Ferriman-Gallwey criteria as well as their weight and height to determine their BMI before intervention were measured. A checklist was given to the participants to remind them of their daily medication use, and they were contacted monthly to ensure that they were taking the medication.
The participants’ biochemical parameters including Fasting Blood Insulin (FBI), Fasting Blood Sugar (FBS), triglyceride, total cholesterol, LDL-C, HDL-C were measured before intervention and then 3 months after. The participants were directed to Ava laboratory in Eslamshahr for those measurements. Venous sampling was used with a 5 ml syringe by the laboratory personnel to extract 5 ml of blood from the brachial region. The test results were provided to the researcher. Three months after the intervention, hormonal tests (testosterone and SHBG) were measured as well. All blood tests were conducted at a certain stage of the menstrual cycle (follicular phase). Insulin resistance index (HOMA-IR) was calculated based on FBS and FBI. The participants were to refrain from using hormonal drugs, and supplements, having specific diets or doing heavy sports during the study.
Random allocation & intervention
The participants were allocated into two groups (curcumin and placebo) using block randomization with a ratio of 1:1. Identical black opaque bottles numbered consecutively (in order of allocation) were used to conceal what was allocated to each participant. The bottles were prepared by a third party that had no role in the sampling or gathering and analysis of data. The curcumin and placebo were produced by Dineh Iran pharmaceutical company (Qazvin, Iran). The intervention group received two 500 mg tablets of edible curcumin together at the same time per day for twelve weeks while the control group received placebo tablets similar to curcumin. Placebo and curcumin tablets were identical in terms of weight, shape, color and smell.
Data collection tools
Questionnaires for socio-demographic information, a checklist for recording tests, a menstrual cycle characteristics questionnaire, and the Ferriman–Gallwey scale were used to collect the data. The food frequency questionnaire (FFQ) was used to measure the nutritional status of the participants.
The menstrual cycle characteristics questionnaire includes questions about the average interval of menstrual cycles and the average duration of bleeding in the last three months which are asked twice, once at the beginning of the study and then three months after the intervention.
The Ferriman–Gallwey scale is also used in the same two time periods to evaluate hirsutism. This scale evaluates the state of hair growth in 9 areas of the body and assigns a score between zero and four according to the Likert scale. Zero means no hair and four means excessive hair growth. The highest possible score for any one participant in this questionnaire would be 36 and the lowest score would be zero [22].
The FFQ used in this study included 67 types of food which were used to gather information about the intake of each food. The participants were asked about the frequency and amount of intake of each food during a day, week, and month. The data was eventually summarized into “how many times in the week the participant ate each type of food”, “how many grams of it was eaten each time”, and “how many grams of it was eaten each week”.
To assess adherence to treatment, the participants were requested to record the drug use in a drug use checklist.
Sample size
The sample size was determined based on the testosterone levels using G*Power software. Considering the data from the Gholizadeh Shamasbi study [23]; a 25% decrease in mean FBS levels; and the following values, M1 = 80.68; Sd1 = Sd2 = 12.3, M2 = 67.6; power = 95% and the two-sided α = 0.05, the sample size was calculated equal with 25 people for each group. With this calculated sample size, the trial has > 95% power for other primary outcomes except of testosterone variable.
Statistical analysis
After gathering the data, SPSS software version 24 was used for data analysis. Descriptive statistics such as mean (standard deviation) were used for quantitative data and number (percentage) was used for qualitative data. Median (percentile 25 to percentile 75) was used for quantitative data that had an abnormal distribution. Kolmogorov-Smirnov test was used to evaluate the normality of the data. Variables such as fasting insulin and HOMA-IR before and after intervention, testosterone, SHBG, hirsutism before and after intervention, and the duration of menstruation had an abnormal distribution while other variables had a normal distribution. An independent t-test was used for an intergroup comparison of variables with a normal distribution before intervention and after the intervention, ANCOVA test was used with a control of baseline values. Mann-Whitney U test was used for an intergroup comparison of variables with an abnormal distribution before and after the intervention. The paired samples t-test and Wilcoxon signed ranks test were used for intra-group comparisons of outcomes with normal and abnormal distribution, respectively.
To analyze the FFQ, the nutrient units were converted to grams per day using the book “The Manual for Household Measures”. Also, any food or drink was coded and recorded in Nutritionist IV software which was adjusted for Iranian food to evaluate the amount of energy and nutrients received by the participants. The intake of energy, macronutrients, and micronutrients of each participant was also determined. All of the analysis was done base on an intention to treat. P < 0.05 was considered as significant.
Results
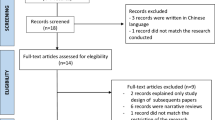
Between 2019 and 2022 about 100 people were evaluated in terms of having the necessary criteria. Four did not enter the study for lack of interest, 15 for having a certain diet, and 27 for having used contraceptives recently. In the end, the data from 27 people in the intervention group and 27 people in the control group were analyzed (Fig. 1). The percentage of adherence to therapy in the both groups was 100%.

Study flow chart
The average age of women in the curcumin group was 28.44 (SD: 7.61) years while the average age of women in the placebo group was 30.85 (SD: 8.63) years. The BMI score of the curcumin group was 27.34 (SD: 5.42) kg/m2 and the placebo group was 26.41 (SD: 4.21) kg/m2. Most women in both groups were nulliparous (74% in the curcumin group and 63% in the placebo group). There was no significant statistical difference between the curcumin and placebo groups in terms of socio-demographic and obstetrics characteristics. There was no statistically significant difference between the two groups in terms of intake of nutrients such as energy, cholesterol, protein, saturated fat, carbohydrate, total fat, and fiber as well (Table 1).
Primary outcomes
The mean (SD) serum FBS level before intervention was 93.92 (9.12) in the curcumin group and 91.33 (9.40) in the placebo group so there was no statistically significant difference between the two groups (P = 0.314). After 12 weeks of intervention, the mean (SD) serum FBS level in the curcumin group was 90.38 (10.69) and in the placebo group it was 95.22 (11.22) which is significantly higher than the curcumin group (Mean Difference (MD): -6.24; 95% Confidence Interval (95% CI): -11.73 to -0.76; P = 0.027).
The mean (SD) serum triglyceride level before intervention was 110.81 (47.11) in the curcumin group and 137.19 (43.20) in the placebo group which means a statistically significant difference between the two groups (P = 0.038). After 12 weeks of intervention, the mean (SD) serum triglyceride level in the curcumin group was 128.02 (6.13) and in the placebo group it was 136.27 (6.00) which means no statistically significant difference between the two groups (MD: -8.25; 95% CI: -25.85 to 9.35; P = 0.351).
The mean (SD) serum cholesterol level before intervention was 158.46 (32.9) in the curcumin group and 162.59 (34.97) in the placebo group so there was no statistically significant difference between the two groups (P = 0.660). After 12 weeks of intervention, the mean (SD) serum cholesterol level in the curcumin group was 165.85 (37.69) and in the placebo group it was 174.19 (40.93) which means no statistically significant difference between the two groups (MD: -6.25; 95% CI: -26.13 to 13.57; P = 0.528).
The mean (SD) serum LDL level before intervention was 88.77 (25.33) in the curcumin group and 91.11 (27.99) in the placebo group so there was no statistically significant difference between the two groups (P = 0.751). After 12 weeks of intervention, the mean (SD) serum LDL level in the curcumin group was 89.96 (30.92) and in the placebo group it was 105.70 (29.33) which means no statistically significant difference between the two groups (MD: -14.81; 95% CI: -30.52 to 0.91; P = 0.064).
The mean (SD) serum HDL level before intervention was 50.12 (10.89) in the curcumin group and 105.70 (29.33) in the placebo group so there was no statistically significant difference between the two groups (P = 0.614). After 12 weeks of intervention, the mean (SD) serum HDL level in the curcumin group was 53.77 (13.15) and in the placebo group it was 51.56 (9.74) which means no statistically significant difference between the two groups (MD: 3.22; 95% CI: -3.04 to 9.48; P = 0.306).
The mean (SD) serum fasting insulin level before intervention was 12.54 (7.56) in the curcumin group and 9.76 (7.25) in the placebo group so there was no statistically significant difference between the two groups (P = 0.135). After 12 weeks of intervention, the mean (SD) serum fasting insulin level in the curcumin group was 9.50 (7.02) and in the placebo group it was 10.11 (9.30) which means no statistically significant difference between the two groups (P = 0.929).
The mean (SD) HOMA-IR before intervention was 2.88 (1.99) in the curcumin group and 2.16 (1.43) in the placebo group so there was no statistically significant difference between the two groups (P = 0.229). After 12 weeks of intervention, the mean (SD) serum HOMA-IR in the curcumin group was 2.11 (1.79) and in the placebo group it was 2.40 (2.11) which means no statistically significant difference between the two groups (P = 0.736).
After the intervention, the mean (SD) serum testosterone level in the curcumin group was 0.64 (0.39) and in the placebo group it was 0.77 (0.36) which means no statistically significant difference between the two groups (0.133). After the intervention, the mean (SD) serum SHBG level in the curcumin group was 57.11 (38.57) and in the placebo group it was 60.67 (40.87) which means no statistically significant difference between the two groups (P = 0.682).
The intra-group comparison results showed that there was statistical significant difference between before and after intervention in terms of fasting insulin level (P = 0.005) and HOMA-IR (P = 0.005) in the curcumin group. Also, the post-intervention FBS level increased significantly compared to pre-intervention level in the placebo group (P = 0.037) (Table 2).
Secondary outcomes
Amenorrhea (i.e., cessation of previously regular menses for three months or previously irregular period for six months) [24] frequency before intervention was %26.98 in the curcumin group and %37.0 in the placebo group while oligomenorrhea frequency was %63.0 in the curcumin group and % 59.3in the placebo group, so there was no statistically significant difference between the two groups. After the intervention, the amenorrhea frequency was %11.1 in the curcumin group and %29.68 in the placebo group while the oligomenorrhea frequency was %37.0 in the curcumin group and %51.9 in the placebo group, so there was a statistically significant difference between the two groups in terms of menstruation characteristics (P = 0.038). The median (Percentile 25 to 75) length of menstruation before intervention was 4.0 (2.0 to 5.0) in the curcumin group and 5.0 (3.0 to 5.0) in the placebo group, so there was no significant difference between the two. The median (Percentile 25 to 75) length of menstruation after the intervention was 4.0 (0.0 to 5.0) in the curcumin group and 4.0 (2.0 to 5.0) in the placebo group, so there was no statistically significant difference between the two groups (P = 0.286) (Table 3).
The mean hirsutism score (SD) before intervention was 11.85 in the curcumin group (4.63) and 12.19 (3.65) in the placebo group so there was no statistically significant difference between the two groups (P = 0.602). The mean (SD) hirsutism score after intervention in the curcumin group was 11.92 (4.71) and 12.19 (3.65) in the placebo group, which means no statistically significant difference between the two groups (P = 0.630) (Table 4).
Discussion
According to the study results, administrating curcumin only led to a decrease in FBS levels and did not significantly affect other metabolic indices (triglyceride, cholesterol, LDL-C, HDL-C, insulin, testosterone and SHBG). Regarding the amenorrhea and oligomenorrhea frequency, the numbers in the curcumin group were significantly lower than in the placebo group but there was no statistically significant difference between the two groups in terms of length of menstruation. Also, curcumin had no significant positive effect on hirsutism in women with PCOS.
In the present study, administrating curcumin led to a decrease in FBS, FBI and HOMA-IR in the curcumin group. Our results were partly consistent with those of previous studies; in a randomized clinical trial, 60 individuals with PCOS were randomly divided into a curcumin and placebo groups and received 500 mg of curcumin or placebo tablets for 12 weeks. Generally administrating curcumin for 12 weeks to women with PCOS had positive effects on body weight, controlling the blood sugar, serum lipids (except triglycerides), very low-density lipoprotein (VLDL-cholesterol) levels, and peroxisome proliferator-activated receptor gamma (PAR-g) and low-density lipoprotein receptor (LDLR) gene expression [25]. In another randomized trial, 67 individuals with PCOS received 500 mg curcumin or placebo tablets three times a day, for 12 weeks. According to the study results, plasma fasting glucose levels, as well as dehydroepiandrosterone, were decreased significantly in the curcumin group in comparison to the placebo group [26].
In a systematic review, the effect of curcumin on glycemic control and lipid profile was examined. Based on the result of the reviewed studies, curcumin improved fasting glucose levels, insulin, and homeostasis model assessment of insulin resistance (HOMA-IR) in a significant way. Moreover, high-density lipoprotein and cholesterol levels were significantly improved. But it did not have any significant effect on improving low-density lipoprotein and triglyceride levels [27]. This is following the results of our study which showed that curcumin improved fasting glucose levels but had no significant effect on triglyceride and LDL.
Curcumin decreases blood sugar through different mechanisms such as increasing glucose and glycolysis uptake and glycogen synthesis in skeletal muscles or decreasing gluconeogenesis in the liver [28]. Furthermore, curcumin was shown to be able to increase glucose uptake by increasing phosphorylation in AMP-activated protein kinase (AMPK) [29]. Curcumin increases the performance of mitogen-activated protein kinase (MAPK), kinase (MEK) 3/6-p38 signaling pathways, and MAPK downstream from the AMPK cascade, which will in turn increase cellular glucose consumption [30, 31]. Curcumin stimulates adenosine monophosphate-activated protein kinase, which suppresses gluconeogenesis through preventing phosphoenolpyruvate carboxykinase and glucose-6 phosphatase [32, 33].
Probably, the anti-inflammatory property of curcumin is also effective in regulating glucose and lipid metabolism. As pro-inflammatory cytokines is higher in patients with PCOS [34]. TNF-α can stimulate serine phosphorylation of the insulin receptor, which leads to insulin resistance [35]. Curcumin significantly reduces TNF-α and interleukin-6 levels [36, 37]. Therefore, it can reduce insulin sensitivity and insulin resistance caused by obesity [38, 39]. Curcumin can upregulate the gene expression of peroxisome proliferator-activated receptor-gamma coactivator 1 alpha (PGC-1α), which rises the activity of glutathione peroxidase, reducing the oxidative stress expression [26].
Also, it seems that curcumin affects glucose metabolism by causing changes in enzyme activity associated with glucose; curcumin increases hepatic glucokinase activity while significantly decreasing glucose 6-phosphate and phosphoenolpyruvate carboxykinase activities. Curcumin stimulates the release of glucagon-like peptide-1 [40, 41]. The reason behind the differences between our study and other studies can be the differences in demography, age, genetics, anthropometrics, dosage, pharmacokinetic factors, follow-up duration, and sample size.
Following all principles of a clinical trial such as random allocation, hiding allocation, and blinding were among the strengths of this study. No loss of samples was another strength of this study. The small sample size was one of the limitations of this study and having a bigger sample size is recommended for further studies. Also, the study power was lower than 80% for detecting of significant difference between groups for testosterone level outcome.
Conclusion
Curcumin decreased FBS levels and improved menstruation characteristics (amenorrhea, oligomenorrhea, and menstrual irregularities) in women with PCOS but did not affect other metabolic, hormonal, and hirsutism indices. More studies using a larger sample size are required for a definitive conclusion.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author on reasonable request.
Abbreviations
- FBI:
-
Fasting Blood Insulin
- FBS:
-
Fasting Blood Sugar
- LDL-C:
-
Low Density Lipoprotein- cholesterol
- HDL-C:
-
High Density Lipoprotein- cholesterol
- SHBG:
-
Sex Hormone Binding Globulin
- IRCT:
-
Iranian Registry of Clinical Trials
- PCOS:
-
Polycystic ovary syndrome
- DHEAS:
-
dehydroepiandrosterone sulfate
- CAH:
-
Congenital Adrenal Hyperplasia
- FFQ:
-
Food Frequency Questionnaire
- SD:
-
Standard Deviation
- MD:
-
Mean Difference
- 95% CI:
-
95% Confidence Interval
- AMPK:
-
AMP-activated protein kinase
- MAPK:
-
Mitogen-Activated Protein Kinase
- HOMA-IR:
-
Homeostatic Model Assessment for Insulin Resistance.
References
Reaven GM, Banting. lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595 – 607.
Zhou JY, Chan L, Zhou SW. Omentin: linking metabolic syndrome and cardiovascular disease. Curr Vasc Pharmacol. 2014;12(1):136–43.
March WA, Moore VM, Willson KJ, Phillips DIW, Norman RJ, Davies MJ. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum Reprod. 2010;25(2):544–51.
Barbieri RL, Ehrmann DA. Clinical manifestations of polycystic ovary syndrome in adults.UpToDate. 2014;17.
Speroff L, Fritz MA. Clinical gynecologic endocrinology and infertility. 8th edition. USA: Lipppincott Williams & Wilkins; 2012.
Sayehmiri F, Kiani F, sayehmiri K, Maleki F, Ahmadi M, Shohani M. Prevalence of polycystic ovary syndrome in iranian women: a systematic review and Meta-analysis. Iran J Obstet Gynecol Infertil. 2014;17(115):11–21.
Tehrani FR, Simbar M, Tohidi M, Hosseinpanah F, Azizi F. The prevalence of polycystic ovary syndrome in a community sample of iranian population: iranian PCOS prevalence study. Reprod Biol Endocrinol. 2011;9(39):39.
Norman RJ, Dewailly D, Legro RS, Hickey TE. Polycystic ovary syndrome. Lancet. 2007;370(9588):685–97.
Norman RJ, Teede HJ. A new evidence-based guideline for assessment and management of polycystic ovary syndrome. Med J Aust. 2018;209(7):299–300.
Elsheikh M, Murphy C. Polycystic ovary syndrome. New York: Oxford University Press; 2008.
Barrea L, Marzullo P, Muscogiuri G, et al. Source and amount of carbohydrate in the diet and inflammation in women with polycystic ovary syndrome. Nut Res Rev. 2018;31(2):291–301.
Goodarzi MO. Looking for polycystic ovary syndrome genes: rational and best strategy. Semin Reprod Med. 2008;26(1):5–13.
Moran LJ, Hutchison SK, Norman RJ, Teede HJ. Lifestyle changes in women with polycystic ovary syndrome.Cochrane Database Syst Rev. 2011(2):Cd007506.
Jeanes YM, Barr S, Smith K, Hart KH. Dietary management of women with polycystic ovary syndrome in the United Kingdom: the role of dietitians. J Hum Nutr Diet. 2009;22(6):551–8.
Harrison CL, Lombard CB, Moran LJ, Teede HJ. Exercise therapy in polycystic ovary syndrome: a systematic review. Hum Reprod Update. 2011;17(2):171–83.
Hewlings SJ, Kalman DS, Curcumin. A review of its effects on human health. Foods. 2017;6:92.
Nistico S, Tamburi F, Bennardo L et al. Treatment of telogen effluvium using a dietary supplement containing Boswellia serrata, Curcuma longa, and Vitis vinifera: results of an observational study.Dermatol Ther. 2019, 32, e12842.
Mohammadi S, Karimzadeh Bardei L, Hojati V, Ghorbani AG, Nabiuni M. Anti-inflammatory effects of curcumin on insulin resistance index, levels of interleukin-6, c-reactive protein, and liver histology in polycystic ovary syndrome-induced rats. Cell J. 2017;19(3):425–33.
Rey-Roldan E, Perez Lana MB, Galluzzo L, Blanco G, Onetto C, Straminsky V, et al. Is the polycystic ovary syndrome the causative of the increase in inflammatory markers and metabolic risk? Gynecol Endocrinol. 2013;29(2):141–4.
Tabrizi R, Vakili S, Lankarani KB, et al. The effects of curcumin on glycemic control and lipid profiles among patients with metabolic diseases: a systematic review and meta-analysis of randomized controlled trials. Curr Pharm Des. 2018;24(27):3184–99.
Riaz Y, Parekh U. Oligomenorrhea. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [cited 2022 Dec 26]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK560575/
Mirghafourvand M, Charandabi SM-A, Aliasghari F. Predictors of depression in iranian women with polycystic ovarian syndrome. Community Ment Health J. 2018;54(8):1274–83.
Gholizadeh Shamasbi S, Dehgan P, Mohammad-Alizadeh Charandabi S, Aliasgarzadeh A, Mirghafourvand M. The effect of resistant dextrin as a prebiotic on metabolic parameters and androgen level in women with polycystic ovarian syndrome: a randomized, triple-blind, controlled, clinical trial. Eur J Nutr. 2019;58(2):629–40.
Klein DA, Paradise SL, Reeder RM, Amenorrhea. A systematic Approach to diagnosis and management. Am Fam Physician. 2019;100(1):39–48.
Jamilian M, Foroozanfard F, Kavossian E, et al. Effects of curcumin on body weight, glycemic control and serum lipids in women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Clin Nutr ESPEN. 2020;36:128–33.
Heshmati J, Moini A, Sepidarkish M, et al. Effects of curcumin supplementation on blood glucose, insulin resistance and androgens in patients with polycystic ovary syndrome: a randomized double-blind placebo-controlled clinical trial. Phytomed. 2021;80:153395.
Chien YJ, Chang CY, Wu MY, Chen CH, Horng YS, Wu HC. Effects of curcumin on glycemic control and lipid profile in polycystic ovary syndrome: systematic review with meta-analysis and trial sequential analysis. Nutrients. 2021;13(2):684.
Wojcik M, Krawczyk M, Wojcik P, Cypryk K, Wozniak LA. Molecular mechanisms underlying curcumin-mediated therapeutic effects in type 2 diabetes and cancer. Oxid Med Cell Longev. 2018;2018:9698258.
Lu X, Wu F, Jiang M, Sun X, Tian G. Curcumin ameliorates gestational diabetes in mice partly through activating AMPK. Pharm Biol. 2019;57(1):250–4.
Akbari A, Mobini GR, Agah S, et al. Coenzyme Q10 supplementation and oxidative stress parameters: a systematic review and meta-analysis of clinical trials. Eur J Clin Pharmacol. 2020;76(11):1483–99.
Kim JH, Park JM, Kim EK, et al. Curcumin stimulates glucose uptake through AMPK-p38 MAPK pathways in L6 myotube cells. J Cell Physiol. 2010;223(3):771–8.
Srivastava RA, Pinkosky SL, Filippov S, Hanselman JC, Cramer CT, Newton RS. AMP-activated protein kinase: an emerging drug target to regulate imbalances in lipid and carbohydrate metabolism to treat cardio-metabolic diseases. J Lipid Res. 2012;53:2490–514.
Fujiwara H, Hosokawa M, Zhou X, Fujimoto S, Fukuda K, Toyoda K, Nishi Y, Fujita Y, Yamada K, Yamada Y, et al. Curcumin inhibits glucose production in isolated mice hepatocytes. Diabetes Res Clin Pract. 2008;80:185–91.
Gao L, Gu Y, Yin X. High serum tumor necrosis factor-alpha levels in women with polycystic ovary syndrome: a meta-analysis. PLoS ONE. 2016;11:e0164021.
Rui L, Aguirre V, Kim JK, Shulman GI, Lee A, Corbould A, Dunaif A, White MF. Insulin/IGF-1 and TNF-alpha stimulate phosphorylation of IRS-1 at inhibitory Ser307 via distinct pathways. J Clin Investig. 2001;107:181–9.
Sahebkar A, Cicero AFG, Simental-Mendia LE, Aggarwal BB, Gupta SC. Curcumin downregulates human tumor necrosis factor-alpha levels: a systematic review and meta-analysis ofrandomized controlled trials. Pharmacol Res. 2016;107:234–42.
Derosa G, Maffioli P, Simental-Mendia LE, Bo S, Sahebkar A. Effect of curcumin on circulating interleukin-6 concentrations: a systematic review and meta-analysis of randomized controlled trials. Pharmacol Res. 2016;111:394–404.
Akash MSH, Rehman K, Liaqat A. Tumor necrosis factor-alpha: role in development of insulin resistance and pathogenesis of type 2 diabetes mellitus. J Cell Biochem. 2018;119:105–10.
Moller DE. Potential role of TNF-alpha in the pathogenesis of insulin resistance and type 2 diabetes. Trends Endocrinol Metab. 2000;11:212–17.
Seo KI, Choi MS, Jung UJ, et al. Effect of curcumin supplementation on blood glucose, plasma insulin, and glucose homeostasis related enzyme activities in diabetic db/db mice. Mol Nutr Food Res. 2008;52(9):995–1004.
Kato M, Nishikawa S, Ikehata A, et al. Curcumin improves glucose tolerance via stimulation of glucagon-like peptide‐1 secretion. Mol Nutr Food Res. 2017;61(3):1600471.
Acknowledgements
We sincerely thank all women who participated in this study. Also, we thank Dineh Iran pharmaceutical company for supplying the curcumin and placebo tablets.
Funding
This research is supported by Tabriz University of Medical Sciences. The funding source had no involvement in design of the study, data collection, data analysis, etc.
Author information
Authors and Affiliations
Contributions
NG and MM were responsible for drafting the trial protocol, data collection, data analysis and interpretation and writing of the final report. SG, ES and SA were involved in drafting the protocol, data collection and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics committee of Tabriz University of Medical Sciences with the code of IR.TBZMED.REC.1398.017. All participants were ensured about the matter of confidentiality. Also, informed written consent was obtained from all participants and parent/legally authorized representatives of illiterate participants. All methods were performed in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ghanbarzadeh-Ghashti, N., Ghanbari-Homaie, S., Shaseb, E. et al. The effect of Curcumin on metabolic parameters and androgen level in women with polycystic ovary syndrome: a randomized controlled trial. BMC Endocr Disord 23, 40 (2023). https://doi.org/10.1186/s12902-023-01295-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01295-5