
Abstract
Background
Hepatocellular Carcinoma (HCC) can be classified as one of the most common malignancies worldwide. There is scarcity of the published data on the risk factors for HCC in the Gulf Cooperation Council countries specifically Kuwait. Therefore, this case-control study sought to examine the risk factors associated with HCC in Kuwait.
Methods
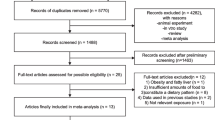
Fifty-three histopathologically confirmed HCC cases were recruited from the Kuwait Cancer Control Center Registry. One hundred ninety-six controls (1:4 ratio) were selected from medical and/ or surgical outpatient’s clinics at all six public hospitals of Kuwait. A structured questionnaire was used to collect the data both from cases and controls through face-to-face interviews. A multivariable logistic regression model was fitted to the case-control data. Adjusted odds ratios (ORadj) and their 95% confidence intervals (CI) were computed using the parameters’ estimates of the final model and used for interpretation of the model.
Results
The HCC cases compared with the controls were 41.6 times more likely to have had the history of non-alcoholic fatty liver disease (NAFLD) (ORadj = 41.6; 95% CI: 8.9–193.5; p < 0.001). The cases compared with the controls were more likely to have reported the history of heavy alcohol drinking (ORadj = 14.2; 95% CI: 1.2–173.4; p = 0.038). Furthermore, compared with the controls, the HCC cases tended to frequently consume milk and/or milk substitutes (≥ 3 glass/ week) (ORadj = 7.2; 95% CI: 1.2–43.4). Conversely however, there was a significant protective effect if the participants reportedly have had regularly used olive oil in their routine diet as a source of fat (ORadj = 0.17; 95% CI: 0.04–0.80) or regularly used non-steroid anti-inflammatory drugs (NSAIDs) (ORadj = 0.20; 95% CI: 0.05–0.71).
Conclusions
This study showed that heavy alcohol consumption, NAFLD history, and excessive consumption of milk/ milk substitutes were associated with a significantly increased HCC risk. Conversely however, regular use of olive oil in the diet as a source of fat or regular use of NSAIDs had a significantly protective effect against HCC risk. Adapting healthy dietary habits and preventing/ treating NAFLD may minimize the HCC risk. Future research with a larger sample size may contemplate validating the results of this study and unraveling additional risk factors contributing to HCC risk. The resultant data may help design and implement evidence-based educational programs for the prevention of HCC in this and other similar settings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is one of the major types of primary liver cancer with an estimated 75% of all liver cancers [1]. Annually about seven million people die of HCC worldwide, making it the third leading cause of cancer-related deaths [2, 3]. HCC is the 5th most common cancer among men and the 9th most common cancer among women [3]. Recent global statistics revealed that the HCC incidence rate (per 105person-years) and HCC related-mortality rates (per 105person-years) were substantially higher among men (14.1, 12.9) than women (5.2, 4.8) [3]. Furthermore, HCC incidence rate varies substantially across the globe [4]. Asia and Africa have the highest incidence rate (per 105 person-years) of HCC ranging between 3 and 26 in the world [5]. In East Asia, Magnolias has the highest HCC incidence rate (93.7 per 105 person-years). However, China has the greatest number of HCC cases because of both an increased incidence rate (18.3 per 105 person-years) and with the world’s largest population (1.4 billion). Between 1987 and 2012, a decline in the HCC incidence was observed in many Asian countries [6]. Conversely however, an increase HCC incidence was reported from India, Americas, Oceania, and most of the European countries [7]. In the Middle Eastern countries, the HCC prevalence is lower compared to sub-Saharan Africa and some Far East countries [4]. However, the HCC prevalence in the Middle Eastern countries has also been increasing and mostly among men than women [8] Over the past decade, the HCC incidence in the Middle Eastern countries has increased dramatically with more pronounced increase in Saudi Arabia (4.5 per 105 person-years) and Egypt (26.4 per 105 person-years) [9]. In Kuwait, the incidence rate of primary liver cancer is 11.7 per 105 person-years and HCC-related mortality rate is 1.8 per 100,000 person-years [4].
Most frequent risk factors for HCC worldwide include lifestyle factors (tobacco smoking, heavy alcohol drinking, consumption of food contaminated with aflatoxin (AFB1), obesity), comorbidities (infection with hepatitis B virus (HBV), hepatitis C virus (HCV), histological liver fibrosis and cirrhosis resulting from HBV and HCV infections, exposure to chemical hazard, diabetes mellitus (DM), genetic hemochromatosis, nonalcoholic fatty liver disease (NAFLD) [10,11,12]. Furthermore, a dose-response relationship has been reported between AFB1 and HCC [13]. Metabolic syndrome, insulin resistance, abdominal adiposity, atherogenic dyslipidemia and high blood pressure (hypertension) have also been implicated in increasing the HCC risk [14]. A meta-analysis has revealed that metabolic syndrome increases the HCC risk by approximately 81% [15]. Parenthetically, a very high prevalence (22.1%) of metabolic syndrome among adults in Kuwait has been reported [16]. In GCC (Gulf Cooperation Council) countries including Kuwait, relatively low prevalences of infections with of HBV (1.1–2.3%) [17, 18] and HCV (0.8 − 1.5%) [18, 19] have been recorded. Moreover, relatively recently it has been shown that Helicobacter pylori, microbiota, co-infection with HBV and hepatitis D virus, oral contraceptive pills and chronic kidney disease were also associated with an increased HCC risk [20, 21]. Over the past decade, it has been shown that the use of statins, metformin, aspirin, and coffee consumption have protective effects against HCC risk [22]. However, there is a paucity of the published data on the risk factors profile for HCC risk in the middle eastern countries including Kuwait. Therefore, the objective of this case-control study was to investigate the risk factors including diet, lifestyles factors and comorbidities associated with HCC risk in Kuwait.
Methods
Study design, setting, and participants
Organizationally Kuwait has six governorates with well-defined area of each governorate, which comprises several demarcated districts. Medical services in each governorate comprise a network of primary health-care clinics and a public hospital. Moreover, there are centralized specialty hospitals, including the Kuwait Cancer Control Centre (KCCC). KCCC is a specialized cancer treatment hospital equipped with the modern facilities for cancer diagnosis, treatment, and follow-up. KCCC is also a full member of the international Association of Cancer Registries (IACR). As per IACR guidelines, KCCC registry collects information concerning malignant neoplasm, as well as mortality data from the Vital and Health Statistics Division of Ministry of Health, Kuwait. Five main areas identified by the IACR are used while assessing the quality of KCCC registry data i.e., completeness of the coverage, completeness of detail of cancer cases, accuracy of said detail, accuracy of reporting, and the accuracy of interpretation. KCCC registry data are also used for research, policymaking, and health service planning, which indeed is dependent on the quality of KCCC database. The accuracy of KCCC registry data appears to be just as accurate as other cancer registries in some western countries including United States, United Kingdom, and Netherlands [23]. Almost all the suspected cancer patients are referred to KCCC. The cancer patients which are initially diagnosed and/or treated elsewhere are also referred to KCCC for further follow-up and treatment management. Health-care is provided free by the government to the nationals, whereas foreign residents must pay nominal fee to seek medical services [24, 25].
A hospital-based case-control study design was implemented to identify the potential risk factors associated with HCC risk. HCC cases registered with KCCC were enrolled. As noted above, suspected cancer patients are referred to KCCC for confirmatory diagnosis and treatment. The cancer patients diagnosed elsewhere are referred to KCCC for follow-up treatment. KCCC is equipped with the modern facilities for cancer diagnosis and treatment. The four controls per case (1:4 ratio) were selected from the general medical and/ or surgical out-patient clinics of the six main public hospitals from all the six governorates of Kuwait.
Case definition, inclusion, and exclusion criteria
A patient of any age, sex (male or female) and nativity (Kuwait or non-Kuwaiti) with histological confirmed HCC diagnosis and treated at KCCC by medical oncologist and hepatologists was enrolled as a case. A patient diagnosed with HCC elsewhere and underwent follow-up for subsequent treatment at KCCC was also eligible for enrollment. A patient with previous diagnosis of cancer of any other body sites was excluded.
Control definition, inclusion, and exclusion criteria
An individual of any age, sex (male or female), nativity (Kuwait or non-Kuwaiti) and without the prior history of HCC and/or cancer of any other body sites was enrolled as a control. Individual visiting an outpatient clinic in selected tertiary-care hospitals with minor complaint (minor trauma/injuries, upper respiratory tract infections, skin rash/ infection, headache, etc.) or accompanying such person was considered for enrollment as a control. The controls were enrolled from the selected tertiary-care hospitals as a sample of convenience by implementing the purposive sampling strategy. No frequency matching was carried out. Individual suffering from acute morbidity or short-term visitor to Kuwait was excluded.
Exposure assessment
A structured questionnaire prepared based on the pertinent literature review [26,27,28], was used to collect the data both from cases and controls by a trained interviewer. Before actual use in the field, the questionnaire was pretested on 30 individuals demographically alike to our potential study participants. The questionnaire comprised questions which were grouped into four sections i.e., (a) socio-demographics including current age (years), age (years) at diagnosis, gender, marital status, nationality, educational attainment, occupation, governorate of residence. (b) potential exposures such as family history, history of current and/ or past morbidities including HBV and/ or HCV infection status (12 questions). Specifically, for the enrolled HCC cases, the history of infection with HBV and/ or HCV was based on their medical records. Whereas, for the controls’ status of infection with HBV and/ or HCV was based on self-reports in response to a question i.e., have you been ever diagnosed as positive for infection with HBV and/ or HCV based on the laboratory test recommended by a physician or your own suspicion of potential exposure to these viral infections. (c) history of weight (kg), height (cm), and physical activity level, past and current smoking (6 questions). (d) dietary habits and past diagnosis of fatty liver, fibrosis, cirrhosis, non-alcoholic fatty liver disease (NAFLD). Dietary habits include frequency of consumption of dietary items, and food frequency (17 questions). For the cases, histopathological information from medical files in KCCC Registry was sought. For the cases, the date of HCC diagnosis was considered as an index year and history of potential exposures was assessed prior to the end of that year. Similarly, for the four controls for a given case, a date of pseudo-diagnosis of HCC was constructed, which was the date of HCC diagnosis in the case. The controls were asked to report their exposures prior to the end of the index year (i.e., year of their pseudo-diagnosis of HCC). Data collection was carried out from August through November 15, 2022. The HCC cases diagnosed between January 1, 2018, and November 14, 2022, were included in the study.
Statistical analysis
Descriptive statistics of sociodemographics were computed to characterize the cases and controls. Chi-squared analysis was used to examine the relationship between the potential risk factors and HCC. The unadjusted associations of sociodemographics and exposures with HCC status were quantified by using simple logistic regression analysis. The variables significantly (p ≤ 0.150) related with HCC status on the univariable analysis were considered for possible inclusion in the multivariable logistic regression analysis. A backward stepwise procedure was used to arrive at the final multivariate logistic regression model. The variables significantly (p < 0.05) related with the case-control status were retained in the final multivariable logistic regression model. To evaluate the goodness-of-fit of the final model, we used the Hosmer and Lemeshow test. Logistic regression assumes that there is little to no multicollinearity between independent variables (IVs), which essentially means IVs shouldn’t be too highly correlated with each other. Nonetheless, we examined multicollinearity by seeking and evaluating the correlation matrix of the coefficients of logistic model. The interaction between any of the two main effects in the final multivariable logistic model was not our interest in this study, therefore none was evaluated. The main effects included in the final multivariable logistic regression model were used to obtain the adjusted odds ratios (ORadj), their corresponding 95% confidence intervals (CI) and were used for the interpretation of the final model. The analysis was performed using the Statistical Package for Social Sciences (SPSS version 26).
For this case-control study, our computed sample size was 53 cases and 196 controls (case to controls ratio = 1:4). Furthermore, this sample size was large enough to achieve a study power of 80% to relate most of the potential exposures (having prevalence of 10% or higher in general population) and the HCC status with an OR of 2.5 or higher using logistic regression assuming 5% significance level (α). This sample size also accounted for potential refusals up to 10%.
Ethics
Before the interview, a written informed consent was sought both from the cases and controls after explaining the study objectives. Confidentiality of the data was assured to the participants. The study protocol was approved (protocol number 1007/11/08/2022) by the Ethics Committee of Ministry of Health, Kuwait. Additionally, the study protocol was also approved (#: VDR/EC-4056/178) by the Ethics Committee of Health Sciences Center, College of Medicine, Kuwait University.
Results
Characteristics of the samples
The final study samples included 53 HCC cases and 196 controls. More HCC cases tended to be 60 years old or older than controls (79.2% vs. 45.9%). The response rate among the cases and the controls was 100% and 91.2% (196/215) respectively. The cited reasons for non-response among the controls were mainly ‘busy’ (5), I don’t like’ (8) and need to go somewhere (6). The distributions of sex and nativity were nearly the same both among cases and controls. A slightly higher proportion of the cases (100%) than controls (94.3%) were ever married. The higher proportions of cases than controls have had a low level of educational attainment (62.3% vs. 54.6%), unemployment (73.9% vs. 56.9%) and a total family income (Kuwaiti dinars per month) ≤ 1000 (62.2% vs. 48.5%) (Table 1).
Chi-squared and univariable logistic regression analyses
Chi-squared analyses showed the distributions of various groups of variables and their association with the HCC status including sociodemographics (age, marital status employment status, total family monthly income), lifestyle factors (cigarette smoking, hookah smoking, physical activity, BMI), comorbidities (family history of HCC, history of diabetes mellites type 2, history of infection with HBV, history of infection with HCV, history of fibrosis, history of cirrhosis, history of NAFLD, history of regular use of NSAID, history of cardiovascular disease, history of statins use), and dietary patterns (frequency of fruits and vegetables consumption, frequency of use of milk and milk substitutes, alcohol drinking, regular use of olive oil, consumption of seafood, butter, ghee, cream, consumption of nuts, consumption of turmeric (Table 2). The unadjusted ORs (ORunadjusted) and their corresponding 95% CIs for the variables in relation to case-control status are in Table 3. Univariable logistic regression analysis showed, that of the demographics, age, total family income (Kuwaiti Dinars/month) were significantly related to case-control status (p < 0.05). From among the lifestyle factors and comorbidities, family history of HCC, history of infections with HBV, HCV, history of diagnosis of fibrosis, cirrhosis, NAFLD, cardiovascular disease, regular use of NSAIDs, frequency of milk or milk substitutes use, heavy alcohol drinking, regular use of olive oil as a source of fat, consumption of nuts, and consumption of turmeric were significantly (p < 0.05) related to the case-control status (Table 3).
Multivariable logistic regression model
The final multivariable logistic regression model showed the risk factors which were significantly (p < 0.05) and independently associated with the HCC status (Table 4). Hosmer and Lemeshow goodness-of-fit test for the final model showed a good fit (Hosmer and Lemeshow test statistic = 7.79; p-value = 0.454). After controlling for the effects of other variables in the model, the HCC cases compared with the controls were more likely to have had reported the history of being heavy drinker of alcohol (ORadj = 14.2; 95% CI: 1.2–173.4; p = 0.038). Moreover, the HCC cases compared with the controls were 41.6 times more likely to have had history of NAFLD (ORadj = 41.6; 95% CI: 8.9–193.5; p < 0.001). Furthermore, compared with the controls, the HCC cases frequently (≥ 3 glasses per week vs. rare (1–2 glasses per week or never) consumed milk or milk substitutes prior to HCC development (ORadj = 7.2; 95% CI: 1.21 = − 43.4; p = 0.038). Conversely however, there was a significant protective effect if the participants reportedly have had regularly used NSAIDs (ORadj = 0.18; 95% CI: 0.05–0.71; p = 0.014) or regularly consumed olive oil in their routine diet as source of fat (ORadj = 0.2; 95% CI: 0.04–0.8). This study did not find any meaningful association between seafood consumption and the HCC status neither in univariable nor in multivariable logistic regression analysis.
Discussion
This study examined the relationship between sociodemographics, dietary patterns, tobacco smoking, alcohol drinking, family history of HCC, comorbidities including diagnosis of infection with HBV, HCV, diabetes type 2, NAFLD, use of NSAIDs, statins and HCC risk. The final multivariable logistic regression model revealed that the history of NAFLD diagnosis, heavy alcohol drinking, frequency of use of milk and milk substitutes, regular use of NSAIDs and regular use of olive oil as a source of fat in the diet were significantly and independently associated with HCC risk after the adjustment for the effects of other variables in the model.
Alcohol consumption was associated with an increased HCC risk in this case-control study. Previously, a meta-analysis of 11 case-controls studies and another meta-analysis of 16 cohort studies revealed that heavy alcohol drinkers had a significantly higher HCC risk compared with nondrinkers or light drinkers of alcohol [29]. The plausible concurrent and/ or alternate pathobiological mechanisms that could potentially explain the association between heavy alcohol drinking and HCC risk include (i) metabolic product of alcohol is acetaldehyde, that has the potential of inducing oxidative stress, thus theoretically generating DNA adducts (i.e., DNA segments) bound to cancer causing chemical. This process could lead to the development of cancerous cells, or carcinogenesis [30]; (ii) heavy alcohol drinking modifies enzymes alcohol dehydrogenase1B (ADH1B) and aldehyde dehydrogenase 2 (ALDH2), hence promote liver carcinogenesis [31]; (iii) heavy alcohol consumption and long-term exposure to alcohol may lead to alcoholic liver disease, which lead to the liver cirrhosis and eventually progress to HCC [32]; (iv) alcohol as a solvent could enhance penetration of carcinogens inside the cells [33]; and/ or heavy alcohol consumption could impair immunity and hepatic detoxification [32].
The results of this case-control study showed that NAFLD (NASH - nonalcoholic steatohepatitis) was significantly and independently related to an increased HCC risk. A review and meta-analysis of 103 observational studies showed a significant association between NAFLD/NASH and HCC risk [34]. Clinically, NAFLD and NASH are caused by the multiple risk factors [35]. Adipose tissue secrete adipokines that provide fatty acid – a main source of NAFLD development. Several adipokines including resistin, leptin, and visfatin are known to play a role in the development of NAFLD, progression to NASH and subsequently to HCC [36, 37]. However, ghrelin, adiponectin, and irisin are considered to have beneficial impact on NAFLD and NASH [38, 39].
In this case-control study, milk and milk substitutes were positively associated with the increased HCC risk. A systematic review and dose-response meta-analyses of seven cohort and eight case-control studies showed that milk and milk substitutes were positively associated with liver cancer [40, 41]. Moreover, two cohort studies showed that consumption of milk and milk substitutes (but not the yogurt) were significantly associated with increased HCC risk [42, 43]. Numerous mechanistic pathways have been proposed to concurrently and/or alternatively explain the association between excessive consumption of dairy products and increased HCC risk. First, several observational and experimental studies have found milk and milk substitutes increase the concentration of insulin-like growth factor-1 (IGF-1), and high levels of IGF-1 could enhance the cancer risk by inhibiting apoptosis and stimulating cell proliferation [44]. This effect was confirmed by meta-analysis of eight randomized trials and 15 cross-sectional studies [45]. In experimental studies, high levels of IGF-1 were shown to enhancing the development of certain cancers including HCC [46, 47]. Furthermore, liver is the main source of circulating IGF-1, therefore compared to other organs, liver has increased exposure to this hormone. High levels of IGF-1 may enhance the growth of HCC both in vivo and vitro [48]. Second, there is an evidence that excessive amount of branched-chain amino acids, lactose which is disaccharide of milk and milk substitutes provide galactose with IGF-1, which could possibly enhance and stimulate the mechanism of target rapamycin complex 1 signaling, and possibly leading to enhance cell proliferation and carcinogenesis [49]. Additionally, milk and milk substitutes are essential sources of dietary fat and excessive consumption of fat has been shown to be correlated with insulin resistance which could be linked to liver diseases including elevated HCC risk [50, 51].
In this case-control study, regular use of olive oil had a significant and independent protective against the HCC risk. A systematic review and meta-analysis showed that the consumption of regular olive oil in the diet as a source of fat was associated with 31% lower cancer risk [52]. Moreover, a large cohort study and a case-control study showed that the regular intake of monosaturated fatty acid was associated with lower HCC risk [53, 54]. A systematic review and a meta-analysis of 117 studies (a total 3,202,496 participants) showed a significant inverse association between Mediterranean diet and the HCC risk [55,56,57]. Mediterranean diet is considered a strong method to fight cancer and this protective effect has been extensively reported [58]. This diet is based on high intake of monounsaturated fatty acid from extra virgin olive oil, fruits and vegetables, nuts, fish, legumes, reducing the consumption of dairy products and meat [56]. The monounsaturated fatty acid down regulates nuclear factor i.e., kappa B NF-κB, which is a family of proteins that facilitate cell functions [59]. NF-κB may be found in an excessive amount in some types of pre-cancerous cells, eventually leading to cancer cell growth [60].
Regular use of NSAIDs had a significantly protective effect against HCC risk in this study. A systematic review and meta-analysis of the observational studies showed that aspirin use was significantly associated with lower HCC risk [61]. Furthermore, regular NSAIDs use was shown to be associated with 41–54% reduction in HCC risk [62, 63]. The use of NSAIDs tends to lower the incidence and related mortality of certain malignancies, especially gastrointestinal cancer. Chronic inflammation is believed to induce the pathogenesis of HCC [64]. Cyclooxygenase (COX) enzymes are well-known targets of NSAIDs. However, the conventional NSAIDs non-selectively inhibit both the constitutive form COX-1, and the inducible form COX-2. COX-2 facilitates inflammatory processes and its expression is undetectable in most normal tissues. It is usually overexpressed in response to proinflammatory stimuli, such as proinflammatory cytokines, mitogens, tumor promoters and growth factors including those which facilitate hepatic carcinogenesis [64,65,66]. NSAIDs tend to obstruct and alter the COX enzymatic pathways important in prostaglandins synthesis which lead to inhibition of HCC cell growth by cell cycle induction of apoptosis. NSAIDs use may regulate hepatocarcinogenesis by non-COX pathways like mitogen-activated protein kinase and PI3K/Akt pathways [67], Moreover, NSAIDs use can downregulate the pro-inflammatory cytokines [65].
This case-control study did not show a meaningful relationship between the consumption of seafood and the HCC risk, whereas, EPIC cohort study [68], and a nested case-control study showed that regular consumption of fish was inversely associated with the HCC risk [69]. The non-significant association between fish consumption and HCC risk in this study could possibly be due to a smaller sample size. Future studies may consider this observation at the planning stage.
Strengths and limitations of the study
Strengths
The study has some notable strengths including, (i) HCC cases enrolled were a representative sample of all such cases in Kuwait. In this study, we enrolled all alive HCC cases using the list frame of the patients from (2018–2022) KCCC; (ii) all the studied HCC cases were diagnosed in a relatively narrow time window, therefore, presumably were comparable with the incident HCC cases and this attribute of selected HCC cases might have contributed to minimizing the recall bias in exposures assessment.
Limitations
This study has some limitations; First, HCC is a rare and aggressive disease with a median survival time of approximately 6–20 months, thus, such incident HCC cases could not be enrolled. Therefore, the possibility of prevalence-incidence (Neyman’s) bias could not be ruled out. Furthermore, we did not have the data on the specific date of HCC diagnosis, consequently we could not calculate and report the median survival time of cases till their enrollment in the study. Second, the data were collected in-person interviews both from cases and controls. Thus, the possibility of respondent’s bias may not be ruled out, since the respondents might have withheld answers to some of the questions pertaining to lifestyle factors including alcohol consumption, body weight, tobacco use. However, the interviewers were trained in interviewing technique and were careful about this aspect of exposures’ assessment. Hence, interviewers tried their best to pose the questions to cases and controls in a comparable manner to ensure unbiased exposures’ assessment. Third, this was a hospital-based case-control study, therefore, the role of Berkson’s bias cannot be ruled out. This bias tends to make risk factors’ distributions similar between case and control groups, thus, weakening the associations of interest between the risk factors of interest and outcome (case-control status). However, we tried to ensure the enrollment of controls free from any gastrointestinal ailments. Fourth, all the HCC cases in this study were histopathologically confirmed, while the study controls didn’t undergo the similar rigorous diagnostic/ screening procedures to rule out the HCC positive status, rather their HCC status was self-reported. Such disparity in diagnostic/ screening procedures for disease status assessment in cases and controls might have led to information bias in the data. However, we selected the controls from among the individuals who were visiting the general hospitals for seeking healthcare for medical conditions other than that of gastrointestinal tract ailments. Therefore, the possibility of such information bias in the data is likely to be very minimal. Fifth, the controls were selected from the patients with minor ailments other than those of gastrointestinal tract who were visiting outpatient clinics of the tertiary-care hospitals. Thus, the controls might not have truly represented the exposures’ experience of the general population at large, hence potentially hampering the generalizability of the results to the target population. Sixth, some confidence intervals for the effect estimates are relatively imprecise mainly because of limited availability of cases due to the aggressive nature of the disease. Moreover, owing to a relatively small sample size and the resultant low study power, some of suspected exposure-outcome associations might have remained undetected. Future studies may take into account this aspect at a planning stage. Lastly, some of the cases soon after HCC diagnosis travelled abroad for treatment, therefore, we might have missed out such cases from the enrollment in this study. However, the proportion of such HCC patients presumably was not large enough to impair the parameters’ estimates in this study.
Conclusions
In conclusion, heavy alcohol consumption, non-alcoholic fatty liver disease, frequent consumption of milk and milk substitutes were associated with a significantly increased HCC risk. Conversely however, the regular use of olive oil in the diet as a source of fat, and the regular use of NSAIDs were significantly protective against the HCC risk. Adapting healthy dietary habits and preventing/ treating NAFLD may minimize the HCC risk. Future research with a larger sample size may contemplate validating the results of this study and unraveling additional risk factors contributing to the HCC risk. The resultant data may help design and implement evidence-based educational programs for the prevention of HCC in this and other similar settings.
Data availability
The dataset used in this study can be made available on a reasonable request to the corresponding author (SA).
References
Harris PS, Hansen RM, Gray ME, Massoud OI, McGuire BM, Shoreibah MG. Hepatocellular carcinoma surveillance: an evidence-based approach. World J Gastroenterol. 2019;25(13):1550–9.
Cavalluzzo B, Mauriello A, Ragone C, Manolio C, Tornesello ML, Buonaguro FM, Tvingsholm SA, Hadrup SR, Tagliamonte M, Buonaguro L. Novel molecular targets for Hepatocellular Carcinoma. Cancers (Basel) 2021, 14(1).
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and Mortality Worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Poustchi H, Sepanlou S, Esmaili S, Mehrabi N, Ansarymoghadam A. Hepatocellular carcinoma in the world and the middle East. Middle East J Dig Dis. 2010;2(1):31–41.
Sahu SK, Chawla YK, Dhiman RK, Singh V, Duseja A, Taneja S, Kalra N, Gorsi U. Rupture of Hepatocellular Carcinoma: a review of literature. J Clin Exp Hepatol. 2019;9(2):245–56.
McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of Hepatocellular Carcinoma. Hepatology. 2021;73(1):4–13.
McGlynn KA, Petrick JL, London WT. Global epidemiology of hepatocellular carcinoma: an emphasis on demographic and regional variability. Clin Liver Dis. 2015;19(2):223–38.
Wu EM, Wong LL, Hernandez BY, Ji JF, Jia W, Kwee SA, Kalathil S. Gender differences in hepatocellular cancer: disparities in nonalcoholic fatty liver disease/steatohepatitis and liver transplantation. Hepatoma Res 2018, 4.
Alghamdi IG, Alghamdi MS. The incidence rate of Liver Cancer in Saudi Arabia: an Observational Descriptive Epidemiological Analysis of Data from the Saudi Cancer Registry (2004–2014). Cancer Manag Res. 2020;12:1101–11.
Fujiwara N, Friedman SL, Goossens N, Hoshida Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J Hepatol. 2018;68(3):526–49.
Li B, Zhang C, Zhan YT. Nonalcoholic Fatty Liver Disease Cirrhosis: A Review of Its Epidemiology, Risk Factors, Clinical Presentation, Diagnosis, Management, and Prognosis. Can J Gastroenterol Hepatol 2018, 2018:2784537.
Schott E, Bergk A, Berg T. [Strategies for the prevention of hepatocellular carcinoma in the context of chronic viral hepatitis]. Z Gastroenterol. 2008;46(1):69–80.
Hoseyni MS. Risk assessment for aflatoxin: III. Modeling the relative risk of hepatocellular carcinoma. Risk Anal. 1992;12(1):123–8.
Li Y, Shi J, Liu X, Deng Q, Huang Y, Yang Z. Metabolic syndrome relates to high risk in hepatocellular carcinoma: a meta-analysis. Discov Med. 2018;26(144):185–96.
Jinjuvadia R, Patel S, Liangpunsakul S. The association between metabolic syndrome and hepatocellular carcinoma: systemic review and meta-analysis. J Clin Gastroenterol. 2014;48(2):172–7.
Alkazemi D, Alsouri N, Zafar T, Kubow S. Hypomagnesemia and the Metabolic Syndrome among Apparently Healthy Kuwaiti Adults: A Cross-Sectional Study. Nutrients 2022, 14(24).
Alali AA, Abo-Shehada MN. Prevalence of Hepatitis B Virus infection in the Gulf Cooperation Council: a systematic review and meta-analysis. BMC Infect Dis. 2022;22(1):819.
Ameen R, Sanad N, Al-Shemmari S, Siddique I, Chowdhury RI, Al-Hamdan S, Al-Bashir A. Prevalence of viral markers among first-time arab blood donors in Kuwait. Transfusion. 2005;45(12):1973–80.
Hasan F, Alfadhli A, Al-Gharabally A, Alkhaldi M, Colombo M, Lazarus JV. Accelerating the elimination of hepatitis C in Kuwait: an expert opinion. World J Gastroenterol. 2020;26(30):4415–27.
Trad D, Bibani N, Sabbah M, Elloumi H, Gargouri D, Ouakaa A, Kharrat J. Known, new and emerging risk factors of hepatocellular carcinoma (review). Presse Med. 2017;46(11):1000–7.
Fabrizi F, Cerutti R, Alfieri CM, Ridruejo E. An update on Hepatocellular Carcinoma in chronic kidney disease. Cancers (Basel) 2021, 13(14).
Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604.
Elbasmi AA, Fayaz MS, Al-Mohanadi S, Al-Nesf Y, Al-Awadi A. Reliability of the Kuwait Cancer Registry: a comparison between breast cancer data collected by clinical oncologists and registry staff. Asian Pac J Cancer Prev. 2010;11(3):735–8.
Akhtar S, Alroughani R, Ahmed SF, Al-Hashel JY. Retrospective cohort study of gender Differential in risk of multiple sclerosis in Kuwait. Neuroepidemiology. 2016;46(3):203–8.
Ziyab AH, Akhtar S. Incidence and trend of road traffic injuries and related deaths in Kuwait: 2000–2009. Injury. 2012;43(12):2018–22.
Alsheridah N, Akhtar S. Diet, obesity and colorectal carcinoma risk: results from a national cancer registry-based middle-eastern study. BMC Cancer. 2018;18(1):1227.
Moussa I, Day RS, Li R, Kaseb A, Jalal PK, Daniel-MacDougall C, Hatia RI, Abdelhakeem A, Rashid A, Chun YS, et al. Association of dietary fat intake and hepatocellular carcinoma among US adults. Cancer Med. 2021;10(20):7308–19.
George ES, Sood S, Broughton A, Cogan G, Hickey M, Chan WS, Sudan S, Nicoll AJ. The Association between Diet and Hepatocellular Carcinoma: a systematic review. Nutrients 2021, 13(1).
Turati F, Galeone C, Rota M, Pelucchi C, Negri E, Bagnardi V, Corrao G, Boffetta P, La Vecchia C. Alcohol and liver cancer: a systematic review and meta-analysis of prospective studies. Ann Oncol. 2014;25(8):1526–35.
Rajalakshmi TR, AravindhaBabu N, Shanmugam KT, Masthan KM. DNA adducts-chemical addons. J Pharm Bioallied Sci. 2015;7(Suppl 1):S197–199.
Cheng G, Zhang W, Jentys A, Ember EE, Gutierrez OY, Liu Y, Lercher JA. Importance of interface open circuit potential on aqueous hydrogenolytic reduction of benzyl alcohol over Pd/C. Nat Commun. 2022;13(1):7967.
He F, Sha Y, Wang B. Relationship between alcohol consumption and the risks of liver cancer, esophageal cancer, and gastric cancer in China: Meta-analysis based on case-control studies. Med (Baltim). 2021;100(33):e26982.
Papadimitriou N, Markozannes G, Kanellopoulou A, Critselis E, Alhardan S, Karafousia V, Kasimis JC, Katsaraki C, Papadopoulou A, Zografou M, et al. An umbrella review of the evidence associating diet and cancer risk at 11 anatomical sites. Nat Commun. 2021;12(1):4579.
Petrelli F, Manara M, Colombo S, De Santi G, Ghidini M, Mariani M, Iaculli A, Rausa E, Rampulla V, Arru M, et al. Hepatocellular carcinoma in patients with nonalcoholic fatty liver disease: a systematic review and meta-analysis: HCC and Steatosis or Steatohepatitis. Neoplasia. 2022;30:100809.
Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–48.
Genc H, Dogru T, Kara M, Tapan S, Ercin CN, Acikel C, Karslioglu Y, Bagci S. Association of plasma visfatin with hepatic and systemic inflammation in nonalcoholic fatty liver disease. Ann Hepatol. 2013;12(4):548–55.
Jamali R, Arj A, Razavizade M, Aarabi MH. Prediction of nonalcoholic fatty liver Disease Via a Novel panel of serum adipokines. Med (Baltim). 2016;95(5):e2630.
Hu J, Ke Y, Wu F, Liu S, Ji C, Zhu X, Zhang Y. Circulating irisin levels in patients with nonalcoholic fatty liver disease: a systematic review and Meta-analysis. Gastroenterol Res Pract. 2020;2020:8818191.
Petta S, Gastaldelli A, Rebelos E, Bugianesi E, Messa P, Miele L, Svegliati-Baroni G, Valenti L, Bonino F. Pathophysiology of non alcoholic fatty liver disease. Int J Mol Sci 2016, 17(12).
Zhao Q, He Y, Wang K, Wang C, Wu H, Gao L, Hu A, Yang W, Wang S. Dairy consumption and Liver Cancer risk: a systematic review and dose-response Meta-analysis of Observational studies. Nutr Cancer. 2021;73(11–12):2821–31.
Melnik BC. Dairy consumption and hepatocellular carcinoma risk. Ann Transl Med. 2021;9(8):736.
Yang W, Sui J, Ma Y, Simon TG, Chong D, Meyerhardt JA, Willett WC, Giovannucci EL, Chan AT, Zhang X. A prospective study of dairy product intake and the risk of hepatocellular carcinoma in U.S. men and women. Int J Cancer. 2020;146(5):1241–9.
Kakkoura MG, Du H, Guo Y, Yu C, Yang L, Pei P, Chen Y, Sansome S, Chan WC, Yang X, et al. Dairy consumption and risks of total and site-specific cancers in Chinese adults: an 11-year prospective study of 0.5 million people. BMC Med. 2022;20(1):134.
Heaney RP, McCarron DA, Dawson-Hughes B, Oparil S, Berga SL, Stern JS, Barr SI, Rosen CJ. Dietary changes favorably affect bone remodeling in older adults. J Am Diet Assoc. 1999;99(10):1228–33.
Qin LQ, He K, Xu JY. Milk consumption and circulating insulin-like growth factor-I level: a systematic literature review. Int J Food Sci Nutr. 2009;60(Suppl 7):330–40.
Ngo MT, Jeng HY, Kuo YC, Diony Nanda J, Brahmadhi A, Ling TY, Chang TS, Huang YH. The role of IGF/IGF-1R signaling in Hepatocellular carcinomas: Stemness-Related properties and Drug Resistance. Int J Mol Sci 2021, 22(4).
Malaguarnera R, Belfiore A. The emerging role of insulin and insulin-like growth factor signaling in cancer stem cells. Front Endocrinol (Lausanne). 2014;5:10.
Lei T, Ling X. IGF-1 promotes the growth and metastasis of hepatocellular carcinoma via the inhibition of proteasome-mediated cathepsin B degradation. World J Gastroenterol. 2015;21(35):10137–49.
Melnik BC, Schmitz G. Pasteurized non-fermented cow’s milk but not fermented milk is a promoter of mTORC1-driven aging and increased mortality. Ageing Res Rev. 2021;67:101270.
El-Serag HB, Hampel H, Javadi F. The association between diabetes and hepatocellular carcinoma: a systematic review of epidemiologic evidence. Clin Gastroenterol Hepatol. 2006;4(3):369–80.
Freedman ND, Cross AJ, McGlynn KA, Abnet CC, Park Y, Hollenbeck AR, Schatzkin A, Everhart JE, Sinha R. Association of meat and fat intake with liver disease and hepatocellular carcinoma in the NIH-AARP cohort. J Natl Cancer Inst. 2010;102(17):1354–65.
Markellos C, Ourailidou ME, Gavriatopoulou M, Halvatsiotis P, Sergentanis TN, Psaltopoulou T. Olive oil intake and cancer risk: a systematic review and meta-analysis. PLoS ONE. 2022;17(1):e0261649.
Duarte-Salles T, Fedirko V, Stepien M, Aleksandrova K, Bamia C, Lagiou P, Laursen AS, Hansen L, Overvad K, Tjonneland A, et al. Dietary fat, fat subtypes and hepatocellular carcinoma in a large European cohort. Int J Cancer. 2015;137(11):2715–28.
Kuper H, Tzonou A, Lagiou P, Mucci LA, Trichopoulos D, Stuver SO, Trichopoulou A. Diet and hepatocellular carcinoma: a case-control study in Greece. Nutr Cancer. 2000;38(1):6–12.
Gao M, Sun K, Guo M, Gao H, Liu K, Yang C, Li S, Liu N. Fish consumption and n-3 polyunsaturated fatty acids, and risk of hepatocellular carcinoma: systematic review and meta-analysis. Cancer Causes Control. 2015;26(3):367–76.
Davis C, Bryan J, Hodgson J, Murphy K. Definition of the Mediterranean Diet; a literature review. Nutrients. 2015;7(11):9139–53.
Morze J, Danielewicz A, Przybylowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr. 2021;60(3):1561–86.
Dayi T, Oniz A. Effects of the Mediterranean diet polyphenols on cancer development. J Prev Med Hyg. 2022;63(2 Suppl 3):E74–80.
Kasonga A, Kruger MC, Coetzee M. Activation of PPARs Modulates Signalling Pathways and Expression of Regulatory Genes in osteoclasts derived from human CD14 + monocytes. Int J Mol Sci 2019, 20(7).
Xia L, Tan S, Zhou Y, Lin J, Wang H, Oyang L, Tian Y, Liu L, Su M, Wang H, et al. Role of the NFkappaB-signaling pathway in cancer. Onco Targets Ther. 2018;11:2063–73.
Simon TG, Ma Y, Ludvigsson JF, Chong DQ, Giovannucci EL, Fuchs CS, Meyerhardt JA, Corey KE, Chung RT, Zhang X, et al. Association between Aspirin Use and Risk of Hepatocellular Carcinoma. JAMA Oncol. 2018;4(12):1683–90.
Nierengarten MB. Aspirin decreases the risk of hepatocellular cancer in at-risk patients. Cancer. 2022;128(2):214–5.
Petrick JL, Sahasrabuddhe VV, Chan AT, Alavanja MC, Beane-Freeman LE, Buring JE, Chen J, Chong DQ, Freedman ND, Fuchs CS, et al. NSAID Use and Risk of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma: the Liver Cancer Pooling Project. Cancer Prev Res (Phila). 2015;8(12):1156–62.
Hakansson A, Molin G. Gut microbiota and inflammation. Nutrients. 2011;3(6):637–82.
Cervello M, Montalto G. Cyclooxygenases in hepatocellular carcinoma. World J Gastroenterol. 2006;12(32):5113–21.
Kumar M, Zhao X, Wang XW. Molecular carcinogenesis of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: one step closer to personalized medicine? Cell Biosci. 2011;1(1):5.
Sahasrabuddhe VV, Gunja MZ, Graubard BI, Trabert B, Schwartz LM, Park Y, Hollenbeck AR, Freedman ND, McGlynn KA. Nonsteroidal anti-inflammatory drug use, chronic liver disease, and hepatocellular carcinoma. J Natl Cancer Inst. 2012;104(23):1808–14.
Jiang W, Li FR, Yang HH, Chen GC, Hua YF. Relationship between Fish Oil Use and Incidence of Primary Liver Cancer: findings from a Population-based prospective cohort study. Front Nutr. 2021;8:771984.
Fedirko V, Trichopolou A, Bamia C, Duarte-Salles T, Trepo E, Aleksandrova K, Nothlings U, Lukanova A, Lagiou P, Boffetta P, et al. Consumption of fish and meats and risk of hepatocellular carcinoma: the European prospective investigation into Cancer and Nutrition (EPIC). Ann Oncol. 2013;24(8):2166–73.
Acknowledgements
The authors express their gratitude to study participants for their understanding, Dr. Asit Kumar, Medical Oncologist at Kuwait Cancer Control Center, Kuwait for facilitating the study.
Funding
This research received no direct external funding.
Author information
Authors and Affiliations
Contributions
All authors contributed equally and reviewed and approved the manuscript for submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Before the interview, a written informed consent was sought both from the cases and controls after explaining the study objectives. Confidentiality of the data was assured to the participants. The study protocol was approved (protocol number 1007/11/08/2022) by the Ethics Committee of Ministry of Health, Kuwait. Additionally, the study protocol was also approved (#: VDR/EC-4056/178) the Ethics Committee of Health Sciences Center, College of Medicine, Kuwait University. The written Informed consent was sought from each study participant. All methods in this study were carried out in accordance with relevant guidelines and regulations of Declaration of Helsinki for medical research involving human subjects.
Consent for publication
Consent to published research manuscript using deidentified data was sought as a part of the overall Informed Consent.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Almohaid, S., Akhtar, S. Diet, lifestyle factors, comorbidities, and hepatocellular carcinoma risk in a middle eastern country: a case-control study. BMC Cancer 24, 694 (2024). https://doi.org/10.1186/s12885-024-12409-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-12409-0