
Abstract
Background
Although lymph node (LN) status and the LN burden determine the outcome of bladder cancer patients treated with cystectomy, compelling arguments have been made for the incorporation of LN density into the current staging system. Here, we investigate the relationship between LN density and clinical outcome in patients with LN-positive disease, following radical cystectomy for bladder cancer.
Methods
PubMed, SCOPUS, the Institute for Scientific Information Web of Science, and the Cochrane Library were searched to identify relevant published literature.
Results
Fourteen studies were included in the meta-analysis, with a total number of 3311 patients. Of these 14 publications, 6 studies, (533 patients), 10 studies (2966 patients), and 5 studies (1108 patients) investigated the prognostic association of LN density with disease-free survival (DFS), disease-specific survival (DSS), and overall survival (OS), respectively. The pooled hazard ratio (HR) for DFS was 1.45 (95 % confidence interval [CI], 1.10–1.91) without heterogeneity (I2 = 0 %, p = 0.52). Higher LN density was significantly associated with poor DSS (pooled HR, 1.53; 95 % CI, 1.23–1.89). However, significant heterogeneity was found between studies (I2 = 66 %, p = 0.002). The pooled HR for OS was statistically significant (pooled HR, 1.45; 95 % CI, 1.11–1.90) without heterogeneity (I2 = 42 %, p = 0.14). The results of the Begg and Egger tests suggested that publication bias was not evident in this meta-analysis.
Conclusions
The data from this meta-analysis indicate that LN density is an independent predictor of clinical outcome in LN-positive patients. LN density may be useful in future staging systems, thus allowing better prognostic classification of LN-positive bladder cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Radical cystectomy with lymph node (LN) dissection remains the standard treatment for patients with muscle-invasive urothelial carcinoma of the bladder, and also for non-muscle-invasive disease, refractory to intravesical therapy. Pelvic LN involvement occurs in approximately 25 % of patients undergoing radical cystectomy for urothelial cancer [1]; when LN positivity is observed, the 10-year mortality rate can reach 80 %, despite adjuvant chemotherapy [2, 3]. Although LN involvement portends a relatively poor prognosis, some patients exhibit long-term survival following surgery, with, or without systemic chemotherapy [4]. Efforts have been made to stratify LN-positive patients according to different prognostic factors to obtain more individualized risk estimations. Although several prognostic factors have previously been reported for LN-positive patients, predictive factors for survival in LN-positive patients have not been clearly defined.
The concept of LN density, i.e. the number of LNs containing metastatic deposits divided by the total number of LNs removed, was first described for bladder cancer in 2003 [5, 6]. Recent studies have suggested that LN density is superior to the tumor-node-metastasis (TNM) classification system [5], and to the absolute number of positive LNs [5, 7] in predicting disease-free survival (DFS) and disease-specific survival (DSS). Although radical surgery alone cures 5–34 % of patients with LN-positive disease, most survivors have only 1–2 microscopically involved LNs, rather than grossly positive, or multiple LN involvement [8]. Therefore, LN metastasis (LN status), and the number of involved LNs (LN burden) determine the outcome of patients with bladder cancer treated with cystectomy [8]. Compelling arguments have been made for the incorporation of LN density into the current American Joint Committee on Cancer (AJCC) staging system [9]. The present study aimed to elucidate the relationship between LN density and clinical outcome in LN-positive patients with bladder cancer following radical cystectomy.
Methods
This analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Additional file 1) [10].
Data sources and search strategy
PubMed, SCOPUS, the Institute for Scientific Information Web of Science, and the Cochrane Library were searched to identify potentially relevant published literature. The search was performed in August 2014. The search terms used included “bladder cancer,” “radical cystectomy,” and “lymph node density.” We also carefully examined the references of articles and reviews to identify potential additional studies.
Study eligibility
Studies were eligible for inclusion in the meta-analysis if they met the following criteria: (1) patients studied had LN-positive bladder cancer; (2) LN density was measured; (3) the association between LN density and clinical outcome was investigated; and (4) the full text articles were published in English. Studies were excluded based on the following criteria: (1) if they were abstracts, review articles, case reports, letters, or laboratory studies; (2) if key information for further analysis was absent; (3) when part, or all, of the same patient series was included in more than one publication, the largest sample size, or the most recent publication was included to avoid duplication of the same survival data; and (4) when studies did not report an adjusted hazard ratio (HR) in multivariate analysis, as the accuracy of HRs without using multivariate analysis is uncertain. However, if the result was negative in univariate analysis and as a result, LN density could not be included in multivariate analysis, the result of the univariate analysis was included. Two reviewers (MK and HSK) independently determined study eligibility. Disagreements were resolved by consensus.
Data extraction and quality assessments
Using a standardized form, data extraction from each of the included studies was performed independently by two reviewers (CK and CWJ). When discrepancies arose between two reviewers, discussion with another reviewer (HHK) was undertaken until a consensus was reached. Quality assessment in this meta-analysis was carried out using the REporting recommendations for tumor MARKer prognostic studies (REMARK) guidelines and quality scale [11, 12], and included the following study parameters: (1) inclusion and exclusion criteria; (2) prospective or retrospective data; (3) sufficient description of patient and tumor characteristics; (4) sufficient description of LN density measurement; (5) well-defined study endpoint; (6) description of patient follow-up period; and (7) identification of patients lost to follow-up or not available for statistical analysis. Scores ranged from 0 to 8; studies with a total score of 8 were considered to show the highest study quality, whereas a score of 0 indicated studies with the lowest quality.
Statistical analysis
We calculated the pooled HR with its corresponding 95 % confidence interval (CI) to assess the association of LN density with survival in LN-positive patients. A HR of >1 indicated a worse prognosis in patients with higher LN density, if the 95 % CI did not overlap. If explicit survival data were not provided, they were calculated from the available numerical data using methods reported by Parmer et al. [13]. A meta-analysis was performed using the DerSimonian and Laird random effects model, applying the inverse of variance as a weighing factor [14]. Heterogeneity between studies was estimated by using the Cochran Q-static and I2 tests [15]. A Q-test with a p-value of <0.05 or an I2 value of >50 % was considered to represent substantial heterogeneity between studies. We also used subgroup analysis with meta-regression analysis to explore the sources of heterogeneity. Funnel plots, the Begg rank correlation test, and the Egger linear regression test were applied to explore potential publication bias, and a p-value of <0.05 was considered significant [16, 17]. All statistical tests were two-sided, and statistical significance was defined as p < 0.05. RevMan statistical software version 5.0 (the Cochrane Collaboration, Copenhagen, Denmark) was used in this study. Meta-regression and publication bias were analyzed using R statistical software version 2.13.0 (R development Core Team, Vienna, Austria; http://www.r-project.org).
Results
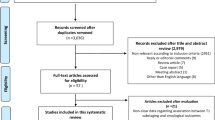
The search strategy retrieved 253 publications, of which 81 were reviewed for eligibility, with 14 studies finally included [5, 18–30]. The detailed screening process used is shown in Fig. 1.

Flow chart of the literature search used in this meta-analysis
Study characteristics
The characteristics of the selected studies are described in Table 1. The total number of patients from all of the studies was 3311 (range, 43–1038; median, 93). The included studies were published between 2003 and 2014. Three studies were conducted in Asian countries, and 11 studies were carried out in non-Asian countries. Among these 14 studies, although data were collected prospectively in 4 studies, none of selected studies was prospective study. Different cut-off values were used for LN density. The quality scores ranged from 3 to 6. As shown in Table 1, 10 of the 14 studies had quality scores of <5, suggesting that most of the studies were not well designed. Other characteristics of the eligible studies are reported in Tables 2 and 3.
Outcomes from eligible studies
Of the 14 publications included in the meta-analysis, 6 studies (533 patients), 10 studies (2966 patients), and 5 studies (1108 patients) investigated the prognostic association of LN density with DFS, DSS, and overall survival (OS), respectively (Tables 3, 4, 5, and 6).
The results of the meta-analysis are shown in Figs. 2, 3, and 4. Overall, the pooled HR for DFS was 1.45 (95 % CI, 1.10–1.91), suggesting that a higher LN density was an indicator of poor prognosis for bladder cancer. No significant heterogeneity was observed among the studies (I2 = 0 %, p = 0.52) (Fig. 2). A meta-analysis of 10 studies found that higher LN density was significantly associated with poor DSS (pooled HR, 1.53; 95 % CI, 1.23–1.89). However, significant heterogeneity was found between studies (I2 = 66 %, p = 0.002) (Fig. 3). Subgroup analysis with meta-regression analysis showed that the number of patients (pheterogeneity = 0.0015), median follow-up (pheterogeneity = 0.0017), and quality scale (pheterogeneity = 0.0233) were possible explanations for heterogeneity (Table 7). Meta-analysis of the 5 studies evaluating the association of LN density with OS found that a higher LN density predicted a worse outcome, with a pooled HR of 1.45 (95 % CI, 1.11–1.90). Inter-study heterogeneity was not significant (I2 = 42 %, p = 0.14) (Fig. 4).

Forest plots of disease-free survival by lymph node density. (Left) The horizontal lines correspond to the study-specific hazard ratio (HR) and 95 % confidence interval (CI), respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of HR and 95 % CI. (Right) The Begg test funnel plots for publication bias. Each point represents a separate study of the indicated association. The vertical line represents the mean effects size

Forest plots of disease-specific survival by lymph node density. (Left) The horizontal lines correspond to the study-specific hazard ratio (HR) and 95 % confidence interval (CI), respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of HR and 95 % CI. (Right) The Begg test funnel plots for publication bias. Each point represents a separate study of the indicated association. The vertical line represents the mean effects size.

Forest plots of overall survival by lymph node density. (Left) The horizontal lines correspond to the study-specific hazard ratio (HR) and 95 % confidence interval (CI), respectively. The area of the squares reflects the study-specific weight. The diamond represents the pooled results of HR and 95 % CI. (Right) The Begg test funnel plots for publication bias. Each point represents a separate study of the indicated association. The vertical line represents the mean effects size
Publication bias
No obvious asymmetry was evident in the Funnel plots of any contrast (Figs. 2, 3, and 4). All the p-values for the Begg and Egger tests for DFS, DSS, and OS were >0.05, providing statistical evidence of funnel plots’ symmetry. These results suggest that publication bias was not evident in this meta-analysis.
Discussion
Up to 25 % of clinically organ-confined tumors show evidence of LN metastasis at the time of surgery. Pathologic specimens from contemporary radical cystectomy series reveal that the rate of LN metastasis increases from 5 % in non-muscle-invasive bladder tumors (≤pT1), to 18 % in pT2a, 27 % in pT2b, and 45 % in pT3–4 [2]. Although LN-positivity is an adverse prognostic factor per se, some LN-positive patients experience long-term survival following radical cystectomy. Therefore, LN dissection may be curative in a selected subset of LN-positive patients [18]. However, prognostic criteria to identify this population have not been defined.
Several prognostic factors have previously been reported for LN-positive patients: (1) pathologic stage of the primary tumor [6, 31]; (2) presence of lymphovascular invasion of the primary tumor [18]; (3) pN stage using the TNM classification; (4) number of LNs involved [2,618,20,32]; (5) number of LNs removed at cystectomy [33–35]; (6) LN density [5, 6]; and (7) the presence of extracapsular extension [18, 28, 36]. However, factors predictive of survival in LN-positive patients are debated.
The pT stage of the TNM classification remains significant in LN-positive bladder cancer [6, 31]. Although differentiation between pT2 and pT3 disease seems unnecessary when LN invasion is present, Stein et al. [6] have previously shown the prognostic significance of extravesical tumor extension compared to organ-confined tumor in LN-positive patients. However, the prognostic significance of the pN stage is unclear [5, 28], although risk stratification of recurrence and survival following radical cystectomy has traditionally been based on TNM staging. The accuracy of the most recent TNM staging system has also been questioned [37, 38], as the location of positive LNs does not seem to have prognostic significance. The number of positive LNs appears to be a significant adverse prognostic factor. Some studies have demonstrated decreased DFS and OS associated with an increasing absolute number of positive LNs [2, 6, 18, 20, 32], but not all studies have confirmed these findings. In addition, the cut-off number for positive LNs that influence outcome is controversial. Furthermore, the total number of positive LNs does not reflect the tumor burden, and its significance is influenced by the extent of the LN dissection. Other studies have demonstrated that the total number of LNs removed, irrespective of LN positivity, is a significant prognostic factor [6, 33–35]. Extracapsular extension may be an independent prognostic factor for DFS and DSS in LN-positive bladder cancer and upper urothelial carcinoma [18, 28, 36].
It has been suggested that LN density is more useful in stratifying patients with LN-positive bladder cancer. Herr [5] found that a LN density cut-off of 20 % was superior to the most recent TNM staging system in predicting DSS and local recurrence, on multivariate analysis. Stephenson et al. [23] also suggested that the aggregate LN metastasis diameter, LN density, and extranodal extension should be considered as the novel predictors in a revised TNM-staging system. However, despite the attempts of multiple studies to explore the association between LN density and its potential association with disease recurrence or death, the results have been inconsistent. For example, none of the new LN-dependent markers, such as localization within the pelvic cavity, extracapsular extension, and LN density were independently significant in the prospective study by Jenson et al. [25]. To our knowledge, the present meta-analysis is the first to clarify the association between LN density and survival in LN-positive bladder cancer using meta-analysis and systematic review. In this meta-analysis, studies reporting HRs of cumulative survival rates were qualitatively summarized using standard meta-analysis techniques. Fourteen studies, with a total of 3311 LN-positive patients, stratifying DFS, DSS, and/or OS by LN density were eligible for inclusion in the meta-analysis. Higher LN density was independently associated with poorer DFS, DSS, and OS. As our meta-analysis includes 14 eligible studies, with a total of 3311 patients, it provides stronger statistical power and a more precise estimation of results than previously published reports. Moreover, our meta-analysis was mainly based on adjusted estimates, and statistical significance was observed for all three end-points, DFS, DSS, and OS.
However, to reach a convincing conclusion regarding the value of LN density for the prognosis of LN-positive bladder cancer, some issues should also be addressed. First, we considered that the definition of what constitutes a “lymph node” varies among urological pathologists in different series. This can impact the nodal yields, and therefore, the burden of lymph node density. Second, the cut-off points for LN density were arbitrarily determined retrospectively, and they have not been validated sufficiently in alternative data sets [8]. Therefore, the threshold for clinically relevant LN density varies between multiple studies and has yet to be established. Third, there is no prospectively evaluated standardized template for pelvic LN dissection. Some data support the use of LN density rather than the absolute number of positive LNs when extended pelvic LN dissection is performed [27]. On the contrary, LN density may be a less sensitive determinant of outcome following limited dissection [8]. Additionally, there were no surgical consistency and uniformity of techniques between previous studies. Therefore, different LN dissection templates, and different surgical procedures may contribute significant bias to a meaningful analysis. Fourth, the number of LNs removed may affect the value of LN density. Jeong et al. [39] demonstrated that when more than 15 LNs were removed, LN density was a predictive factor for survival. In a report by Kassouf et al., LN density proved to be a stronger prognostic factor in patients with a LN count of ≥25 (HR 4.63) than in patients with a LN count of <25 (HR 1.62) [27]. Therefore, owing to interindividual variability in pelvic LN anatomy [40], LN density may not be a prognostic factor in patients with little lymphatic tissue. Furthermore, although greater numbers of LNs removed would most likely correlate with a more extended LN dissection, LN yield is intimately related to histological processing, and to the extent of pathologic review. Fifth, it is not known whether LN density determines survival any better than currently established pN categories of the TNM system [8]. Future studies are needed before LN density can be widely accepted as a staging system or used to replace pN staging. Finally, in the present study, only 2 reports used neoadjuvant chemotherapy; and therefore, it is not enough to determine whether LN density can be a valid marker for survival following neoadjuvant chemotherapy, which may favorably alter the nodal burden [8]. Additionally, given the use of neoadjuvant chemotherapy had gained increasing acceptance for treating invasive bladder cancer, the low rate of neoadjuvant therapy in this meta-analysis may have limitation on the generalizability. Further evaluation of the impact of neoadjuvant chemotherapy on LN density would be necessary.
Several limitations of this study should be considered. First, the HRs calculated in our meta-analysis may be overestimated, as many of the included studies obtained data retrospectively. Thus, adequately designed prospective studies are needed to obtain a more precise estimate. Second, the studies retrieved for our analysis were limited to those published in English, which may result in a language bias, although the present analysis does not support publication bias. Third, varying numbers of patients, median follow-up time, and quality scale might contribute to the heterogeneity of results for DSS found in this study. Although the random-effects model considers heterogeneity, and was used to analyze the studies with heterogeneities, the conclusions drawn from this meta-analysis should be approached with caution. However, heterogeneity of results for DSS was rigorously quantified and analyzed in our meta-regression and subgroup analysis, which contributes to a more reliable conclusion.
Conclusions
In summary, the data from this meta-analysis indicate that LN density is an independent predictor of clinical outcome in LN-positive patients following radical cystectomy for bladder cancer. Although LN density may be related to histological processing and the extent of pathologic review, it is most likely a reflection of the quality and extent of pelvic LN dissection. LN density may be useful in future staging systems, thus allowing better prognostic classification of LN-positive bladder cancer following radical cystectomy. However, prospective validation would be required to define cut-off levels for LN density.
Abbreviations
- LN:
-
Lymph node
- DFS:
-
Disease-free survival
- DSS:
-
Disease-specific survival
- OS:
-
Overall survival
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- TNM:
-
Tumor-node-metastasis
References
Quek ML, Sanderson KM, Daneshmand S, Stein JP. The importance of an extended lymphadenectomy in the management of high-grade invasive bladder cancer. Expert Rev Anticancer Ther. 2004;4:1007–16.
Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. 2001;19:666–75.
Millikan R, Dinney C, Swanson D, Sweeney P, Ro JY, Smith TL, et al. Integrated therapy for locally advanced bladder cancer: Final report of a randomized trial of cystectomy plus adjuvant M-VAC versus cystectomy with both preoperative and postoperative M-VAC. J Clin Oncol. 2001;19:4005–13.
Herr HW, Donat SM. Outcome of patients with grossly node positive bladder cancer after pelvic lymph node dissection and radical cystectomy. J Urol. 2001;165:62–4.
Herr HW. Superiority of ratio based lymph node staging for bladder cancer. J Urol. 2003;169:943–5.
Stein JP, Cai J, Groshen S, Skinner DG. Risk factors for patients with pelvic lymph node metastases following radical cystectomy with en bloc pelvic lymphadenectomy: concept of lymph node density. J Urol. 2003;170:35–41.
Kassouf W, Leibovici D, Munsell MF, Dinney CP, Grossman HB, Kamat AM. Evaluation of the relevance of lymph node density in a contemporary series of patients undergoing radical cystectomy. J Urol. 2006;176:53–7.
Herr HW. The concept of lymph node density–is it ready for clinical practice? J Urol. 2007;177:1273–5.
Kassouf W, Agarwal PK, Herr HW, Munsell MF, Spiess PE, Brown GA, et al. Lymph node density is superior to TNM nodal status in predicting disease-specific survival after radical cystectomy for bladder cancer: analysis of pooled data from MDACC and MSKCC. J Clin Oncol. 2008;26:121–6.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M, Clark GM. Statistics Subcommittee of the NCI-EORTC Working Group on Cancer Diagnostics. Reporting recommendations for tumor marker prognostic studies (REMARK). J Natl Cancer Inst. 2005;97:1180–4.
de Graeff P, Crijns AP, de Jong S, Boezen M, Post WJ, de Vries EG, et al. Modest effect of p53, EGFR and HER-2/neu on prognosis in epithelial ovarian cancer: a meta-analysis. Br J Cancer. 2009;101:149–59.
Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998;17:2815–34.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–101.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Fleischmann A, Thalmann GN, Markwalder R, Studer UE. Extracapsular extension of pelvic lymph node metastases from urothelial carcinoma of the bladder is an independent prognostic factor. J Clin Oncol. 2005;23:2358–65.
Osawa T, Abe T, Shinohara N, Harabayashi T, Sazawa A, Kubota K, et al. Role of lymph node density in predicting survival of patients with lymph node metastases after radical cystectomy: a multi-institutional study. Int J Urol. 2009;16:274–8.
Wiesner C, Salzer A, Thomas C, Gellermann-Schultes C, Gillitzer R, Hampel C, et al. Cancer-specific survival after radical cystectomy and standardized extended lymphadenectomy for node-positive bladder cancer: prediction by lymph node positivity and density. BJU Int. 2009;104:331–5.
Furukawa J, Miyake H, Terakawa T, Takenaka A, Fujisawa M. Predictors of cancer-specific survival following radical cystectomy in patients with node-positive bladder cancer. Curr Urol. 2010;4:188–92.
Guzzo TJ, Resnick MJ, Canter DJ, Balandra A, Bergey MR, Magerfleisch L, et al. Impact of adjuvant chemotherapy on patients with lymph node metastasis at the time of radical cystectomy. Can J Urol. 2010;17:5465–71.
Stephenson AJ, Gong MC, Campbell SC, Fergany AF, Hansel DE. Aggregate lymph node metastasis diameter and survival after radical cystectomy for invasive bladder cancer. Urology. 2010;75:382–6.
May M, Herrmann E, Bolenz C, Tiemann A, Brookman-May S, Fritsche HM, et al. Lymph node density affects cancer-specific survival in patients with lymph node-positive urothelial bladder cancer following radical cystectomy. Eur Urol. 2011;59:712–8.
Jensen JB, Ulhøi BP, Jensen KM. Evaluation of different lymph node (LN) variables as prognostic markers in patients undergoing radical cystectomy and extended LN dissection to the level of the inferior mesenteric artery. BJU Int. 2012;109:388–93.
Morgan TM, Barocas DA, Penson DF, Chang SS, Ni S, Clark PE, et al. Lymph node yield at radical cystectomy predicts mortality in node-negative and not node-positive patients. Urology. 2012;80:632–40.
Kassouf W, Svatek RS, Shariat SF, Novara G, Lerner SP, Fradet Y, et al. Critical analysis and validation of lymph node density as prognostic variable in urothelial carcinoma of bladder. Urol Oncol. 2013;31:480–6.
Masson-Lecomte A, Vordos D, Hoznek A, Yiou R, Allory Y, Abbou CC, et al. External validation of extranodal extension and lymph node density as predictors of survival in node-positive bladder cancer after radical cystectomy. Ann Surg Oncol. 2013;20:1389–94.
Mmeje CO, Nunez-Nateras R, Nielsen ME, Pruthi RS, Smith A, Wallen EM, et al. Oncologic outcomes for lymph node-positive urothelial carcinoma patients treated with robot assisted radical cystectomy: with mean follow-up of 3.5 years. Urol Oncol. 2013;31:1621–7.
Kwon T, Jeong IG, You D, Hong B, Hong JH, Ahn H, et al. Long-term oncologic outcomes after radical cystectomy for bladder cancer at a single institution. J Korean Med Sci. 2014;29:669–75.
Vieweg J, Gschwend JE, Herr HW, Fair WR. The impact of primary stage on survival in patients with lymph node positive bladder cancer. J Urol. 1999;161:72–6.
Lerner SP, Skinner DG, Lieskovsky G, Boyd SD, Groshen SL, Ziogas A, et al. The rationale for en bloc pelvic lymph node dissection for bladder cancer patients with nodal metastases: Long-term results. J Urol. 1993;149:758–64.
Herr HW, Bochner BH, Dalbagni G, Donat SM, Reuter VE, Bajorin DF. Impact of the number of lymph nodes retrieved on outcome in patients with muscle invasive bladder cancer. J Urol. 2002;167:1295–8.
May M, Herrmann E, Bolenz C, Brookman-May S, Tiemann A, Moritz R, et al. Association between the number of dissected lymph nodes during pelvic lymphadenectomy and cancer-specific survival in patients with lymph node-negative urothelial carcinoma of the bladder undergoing radical cystectomy. Ann Surg Oncol. 2011;18:2018–25.
Wright JL, Lin DW, Porter MP. The association between extent of lymphadenectomy and survival among patients with lymph node metastases undergoing radical cystectomy. Cancer. 2008;112:2401–8.
Fajkovic H, Cha EK, Jeldres C, Donner G, Chromecki TF, Margulis V, et al. Prognostic value of extranodal extension and other lymph node parameters in patients with upper tract urothelial carcinoma. J Urol. 2012;187:845–51.
Tarin TV, Power NE, Ehdaie B, Sfakianos JP, Silberstein JL, Savage CJ, et al. Lymph node-positive bladder cancer treated with radical cystectomy and lymphadenectomy: Effect of the level of node positivity. Eur Urol. 2012;61:1025–30.
Bruins HM, Dorin RP, Rubino B, Miranda G, Cai J, Daneshmand S, et al. Critical evaluation of the American joint committee on cancer TNM nodal staging system in patients with lymph node-positive disease after radical cystectomy. Eur Urol. 2012;62:671–6.
Jeong IG, Park J, Song K, Ro JY, Song C, Hong JH, et al. Comparison of 2002 TNM nodal status with lymph node density in node-positive patients after radical cystectomy for bladder cancer: Analysis by the number of lymph nodes removed. Urol Oncol. 2011;29:199–204.
Weingärtner K, Ramaswamy A, Bittinger A, Gerharz EW, Vöge D, Riedmiller H. Anatomical basis for pelvic lymphadenectomy in prostate cancer: results of an autopsy study and implications for the clinic. J Urol. 1996;156:1969–71.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare no conflict of interest.
Authors’ contributions
JHK, CWJ, CK, and HHK participated in study conception and design, MK, and HSK carried out the acquisition of data, JHK, MK, HSK, CWJ, CK participated in the analysis and interpretation of data, JHK performed the statistical analysis, JHK, and MK drafted the manuscript, CWJ, CK, and HHK conducted the critical revision of this study. All authors have read and approved the final manuscript.
Additional file
Additonal file 1:
PRISMA 2009 checklist.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ku, J.H., Kang, M., Kim, H.S. et al. Lymph node density as a prognostic variable in node-positive bladder cancer: a meta-analysis. BMC Cancer 15, 447 (2015). https://doi.org/10.1186/s12885-015-1448-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-015-1448-x