
Abstract
Postpartum urinary incontinence may have a severe impact on women’s health. Despite pregnancy and parturition being the most recognized risk factors, methods to identify new pregnant predictor risk factors are needed. Our study investigated the Gestational Diabetes Mellitus, clinical and pelvic floor 3D-ultrasound markers in pregnant women as predictors for 6–18 months of urinary incontinence. This prospective cohort study included nulliparous pregnant women submitted to Gestational Diabetes Mellitus screening in the second trimester. Pelvic floor 3D Ultrasound was performed at the second and third trimesters of gestation to evaluate the pelvic floor muscles and functions. Clinical data, the ICIQ-SF, and ISI questionnaires for urinary incontinence were applied in the third trimester and 6–18 months postpartum. Univariate analysis (P < .20) to extract risk factors variables and multivariate logistic regression analysis (P < .05) to obtain the adjusted relative ratio for urinary incontinence were performed. A total of 93 participants concluded the follow-up. Using the variables obtained by univariate analysis and after adjustments for potential confounders, multivariate analysis revealed that Gestational Diabetes Mellitus exposure was a solid and independent risk factor for 6–18 months of urinary incontinence (Adjusted RR 8.08; 95%CI 1.17–55.87; P:0.034). In addition, a higher Hiatal area observed in distension maneuver from the second to third trimester was negatively associated (Adjusted RR 0.96; 95%CI 0.93–0.99; P:0.023). In conclusion, Gestational Diabetes Mellitus was positively associated with 6–18 months of urinary incontinence, and higher Hiatal area distension was negatively associated.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Gestational diabetes mellitus (GDM) significantly increases the adverse maternal and perinatal outcomes and the likelihood of type 2 Diabetes Mellitus, cardiovascular disease, and Urinary Incontinence (UI) [1,2,3]. GDM and UI combination seems to have hyperglycemic myopathy of the Pelvic Floor Muscle (PFM) and Rectus Abdominis Muscle (RAM) as the underlying mechanism [1, 4,5,6,7,8,9]. Current clinical and experimental studies suggest that Pregnancy Specific-UI (PS-UI) is the earliest symptom of hyperglycemic PFM and RAM myopathy during pregnancy, despite overlooked complaints during prenatal care assistance [5, 6, 8,9,10,11,12,13,14,15,16]. Nevertheless, a previous study showed that the PS-UI, the severity of long-term UI, and the negative impact of UI on quality of life are more significant among GDM pregnant women in the first year postpartum [9]. However, none of these studies correlated the clinical pregnancy data and the anatomical and functional PFM ultrasound assessment during the pregnancy as predictors of postpartum UI [9]. The translabial three-dimensional ultrasonography (3DUS) provides an adequate and reliable evaluation of anatomical and functional PFM status [17]. Besides, we previously demonstrated that GDM-pregnancy had lower Hiatal Area (HA) biometry changes from 24 to 38 weeks of gestation [7]. Therefore, it seems highly likely that GDM alters the maternal adaptation during the pregnancy of PFM structures, leading to a decreased distensibility of the PFM at the end of the third trimester [7]. Reports confirm that GDM and UI are two clinical entities with substantial social and economic burdens associated with significant direct and indirect public health costs [18, 19]. Despite these observations, the link between GDM and long-term UI remains mostly unexplored. Thus, developing 3DUS markers of hyperglycemic myopathy during pregnancy as predictors of long-term UI is necessary to further intervention propositions. Moreover, developing a predictive UI test during pregnancy collaborates to identify a high-risk population accurately. We hypothesized that GDM damages the PFM during pregnancy [7, 20, 21]. This study aimed to identify clinical and PFM 3DUS markers in the second and third trimesters of GDM and non-GDM pregnancy as 6–18 months UI predictors.
Methods
This prospective non-interventional cohort study within the prospective Diamater cohort study protocol [4] started in 2015 at the Perinatal Diabetes Research Center (PDRC), Botucatu Medical School-UNESP. Our institution’s GDM rate is 30–40% due to a tertiary referral hospital.
Regulatory approval was obtained from the Institutional Review Board of Botucatu Medical School (#1.716.895). Written informed consent was obtained from all participants, and all issues related to medical ethics met the requirements of the Helsinki Declaration. All patients involved were properly handled for their morbidities.
Nulliparous singletons over 18 years of age, submitted to GDM screening and translabial 3DUS at two-time points in the second and third trimesters of pregnancy, were enrolled. All women included in this study received prenatal care at PDRC. Exclusion criteria were loss to follow-up, pre-gestational diabetes, pre-gestational UI, severe comorbidities, inadequate GDM screening, preterm birth, use of hypoglycemic drugs in the pregnancy, or new pregnancy during the postpartum period. We also considered only pregnant women with mild GDM, regularly controlled with nutritional and lifestyle interventions, submitted to planned C-sections - the majority based on-demand particular decision, and performed before the labor onset.
Eligible women were included between 24 and 28 weeks of gestation. At enrollment, women completed a detailed questionnaire on sociodemographic information, past medical history, regular physical activity (150 min/week), tobacco use, initial pregnancy weight in Kg, height in cm, and Body Mass Index (weight in kilograms divided by height in meters squared). Ethnicity was defined as Caucasian or non-Caucasian. The researcher performed a PFM 3DUS at 24–28 and 36–40 weeks of gestation (CISF). The translabial 3DUS raw data were stored for posterior blinded and offline analysis. The follow-up continued until April 2020. The same clinical and anthropometric evaluation was done at 36–40 weeks.
Data regarding fasting plasma glucose in the first trimester, 75 g-Oral Glucose Tolerance Test (OGTT) in the second trimester of pregnancy, gestational age (in weeks) at the two-time points of 3DUS, the ISI, and the ICIQ-SF questionnaire scores for PS-UI at 36–40 weeks of pregnancy were recorded.
At 6–18 months after a planned C-section, breastfeeding duration, regular physical activity (minimum 150 min/week), postpartum smoking, newborn weight in grams, and gestational age at delivery, to classify newborn as appropriate, large or small for gestational age, and urinary incontinence (yes or not) with ISI and ICIQ-SF scores were collected.
The primary outcome was the prevalence of 6–18 months of UI development after a planned C-section. We considered the C-section a protective event, avoiding the supposed adverse effects of the parturition and vaginal birth on the pelvic floor. For this purpose, we excluded women exposed to the active labor onset and vaginal birth. We investigated the association between the primary outcome measure and the risk factors, including maternal and perinatal characteristics, the first-trimester fasting glucose negative and the OGTT results as positive or negative for GDM diagnosis, the Pregnancy Specific UI occurrence, and severity of PS-UI, and the PFM 3DUS structural and functional biometry at two-time points during pregnancy.
Women in the study met the Fasting Blood Glucose (FBG) criteria in the first trimester (1– 13 gestational weeks) lower than 92 mg/dL or 5.1 mmol/L [22]. All pregnant women underwent 75-g OGTT between 24 and 28 weeks. The cutoffs were 92, 180, and 153 mg/dL (5.1, 10.0, and 8.5 mmol/L) at fasting, one and two hours after glucose overloading. The GDM was defined by one or more values equal to or more than the respective cutoffs [23,24,25]. A glucose profile was performed during a 1-day hospital stay with the woman on a 30 kcal/Kg-diet fractionated in five meals to diagnose mild gestational hyperglycemia. Plasma glucose was measured every two hours, from 8 AM to 6 PM. The thresholds were 90 mg/dL (5.0 mmol/L) for fasting (8 h) and 130 mg/dL (7.22 mmol/L) for any postprandial level. To maintain normoglycemia, all pregnant women received the appropriate nutritional and lifestyle interventions as the cornerstone of treatment during the last pregnancy. After these instructions, when glycemia remains elevated after 1–2 weeks of lifestyle interventions, daily glucose testing was continued, pharmacological treatment was initiated, and the patient was excluded from this study.
PS-UI was defined as any urinary leakage that started during pregnancy [26]. One specific question was asked to all pregnant women about urinary leakage that started during this pregnancy. If yes, the patient was classified as having PS-UI. Pregnant women with PS-UI complete the UI occurrence and severity evaluation with ISI [27] and ICIQ-SF [20, 28] surveys at 36–40 weeks of gestation [29].
We performed the US examination according to the protocol proposed by Dietz et al. [17] at two-time points in pregnancy: 24–28 weeks (T1) and 36–40 weeks (T2). The functional maneuvers of contraction and distension were previously explained to the participants. The variables of 3DUS in T1 and T2, at rest, contraction, and distension, were collected offline after completing the study by the same observer, blinded (CISF). The measurements: Hiatal area in square cm; Antero-Posterior (AP) diameter in cm; Transversal diameter in cm; variation of AP from T1-T2 in cm; variation of Hiatal area T1-T2 in square cm; variation of Transversal diameter from T1-T2 in cm; the relationship between rest and contraction in T1, in T2 and the T1-T2 variation from all biometry; the relationship between rest and Valsalva in T1, T2, and the T1-T2 variation; the relationship between contraction and Valsalva in T1, T2, and the T1-T2 variation; the percentual variation from each biometry analysis were calculated [7, 30]. We used US equipment with a volumetric curved array three-dimensional transducer in the sagittal plane and 85° in the coronal plane. The exposition and the follow-up period were at the endpoint at 24–28 weeks of gestation (T1), 36–40 weeks (T2), birth, and 6–18 months postpartum.
The Sample Size Calculation used Cochran’s equation together with a population correction. Our estimated population size during this survey was 300 pregnant women. Thus, using a Precision Level of 5%, a Confidence Level of 95%, an estimated proportion of 10% of the exposed population, and a population size of 300 pregnant women, the appropriate sample size was 95.
Descriptive analysis was applied for the demographic characteristics described as mean, standard deviation (SD), and Minimum / Maximum (Min/Max) values and analyzed by an independent sample Student’s t-test. We first used the Cox univariate logistic regression analysis to test the association between each risk factor and long-term UI development. Then, factors with a P-value under 0.20 on the univariate analysis were included in a multivariate logistic regression analysis, using the backward stepwise method to test for independent associations between risk factors and long-term UI development. All significant maternal-pregnancy characteristics and the PFM 3DUS measurements from the univariate analysis were used as predictors. Finally, after adjustments for potential confounding factors, a multivariate logistic regression analysis was performed to identify the relationship between long-term UI and clinical plus PFM 3DUS at the second and third trimesters of pregnancy. Relative risk (RR) and 95% confidence intervals (95%CI) were reported. The RR and 95%CI were calculated for each clinical and 3DUS measure and adjusted for all variables. These variables were excluded successively (models 1 to 8) until reaching the best model, which was defined by the impossibility of excluding any other variable without significant loss in adjustment. A P-value under 0.05 was considered statistically significant for all multivariate logistic tests.
Results
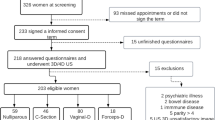
One hundred ninety-five participants were enrolled. We excluded four participants due to preterm birth, four withdrawn during prenatal care, four because of insulin therapy, and ninety participants due to vaginal birth or active labor exposition. After 6–18 months postpartum, 93 participants met the eligibility criteria. Figure 1 represents the flow chart of the study, and Table 1 represents the baseline characteristics of the participants.

Study flow chart
The mean age was 26.4 years (SD 4.8), the prepregnancy body weight was 70.2 Kg (15.8), weight gain was 10.0 Kg (4.9); the mean gestational age at T1 was 26.9 (1.0), at T2 was 36.4 (0.7), and the interval T1-T2 was 9.6 (1.1) weeks; the mean of fasting glucose at the first trimester was 83.6 (9.1) mg/dl; the 75 g-OGTT fasting (mg/dL), one hour and two hours were 81.5(12.2); 128.2 (35.2);115.0 (26.8) respectively. The ICIQ-SF gestational score was 4.9 (5.5), and ISI gestational score was 2.13 (2.28). The newborn weight was 3143 g (394), the maternal postpartum weight was 74.07 (17.49), the breastfeeding duration was 6.97 (3.49) months, and the postpartum ICIQ-SF score was 1.48 (4.04).
Table 2 reports the 3DUS measurements at rest, contraction, and distension profiles of all participants at two-time points of gestation: T1 and T2. The crucial findings were that the HA in square cm at T1 at rest, contraction, and distension was 13.5 (2.1), 12.4(3.7), and 15.1 (2.8), respectively; at T2, 14.5 (2.2), 13.8 (3.4), and 16.5 (3.0), respectively.
Table 3 demonstrates the percentual variation of 3DUS biometry from T1 to T2 pregnancy and during functional maneuvers. The primary feature is the T1-T2 percentual variation of HA from distension to contraction maneuvers, with a mean of -46.8 (SD 28.5).
Table 4 demonstrates the Cox univariate and multivariate logistic regression analysis among UI, clinical, and HA measurements.
The significant univariate results, using a P-value cutoff of 0.20, were: GDM diagnosis, pregnancy weight gain, transversal diameter at rest, HA T1-T2 at rest, percentual variation of HA from contraction to rest at T2, percentual variation of HA from distension to rest at T2, percentual variation of HA from distension to contraction at T2, percentual variation from contraction to rest of HA from T1-T2, and from distension to rest of HA from T1-T2, PS-UI, pregnancy ICIQ-SF score, pregnancy ISI score, superior education level, and newborn weight. The UI risk was 5.4 times higher in women with positive 75 g-OGTT, decreased with increased weight gain, decreased with an increased variation from T1-T2 in transversal diameter and HA at rest; was 3.6 times higher in women who had PS-UI (P < .20). The variables with a P-value under 0.20 in the univariate correlation analysis were included in the multivariate linear regression analysis using the backward stepwise method. We did not use the variable weight gain because its clinical interpretation was inconsistent in this study; univariate analysis demonstrates that a higher weight gain was related to a lower RR for 6–18 months UI, a condition not observed clinically. The multivariate logistic regression analysis was performed after adjustments for GDM, PS-UI diagnosis, superior educational level, variation from T1 to T2 of transversal diameter and HA at rest, percentual variation of HA from contraction to rest and from distension to rest at T2; percentual variation of HA from contraction to rest and from distension to rest from T1 to T2; gestational ICIQ-SF and ISI scores; and newborn weight (model 1). In the backward stepwise model, some variables were eliminated, avoiding collinearity, and after adjustments for the newborn weight (model 2, P:0.992); for gestational ICIQ-SF (model 3; P:0.778); for the percentual of HA variation from contraction to rest at T2 (model 4; P:0.576); for PS-UI (model 5; P: 0.296); for the variation from T1-T2 of transversal diameter at rest (model 6; P: 0.228); for the percentual variation from T1 to T2 of HA from contraction to rest (model 7; P:0.093). Adjusted analysis of potential confounders disclosed that UI development was significantly associated with GDM (model 8; Adjusted RR: 8.08; 95%CI (1.17–55.8); P:0.034) and the percentual variation from T1 to T2 of the HA from distension to rest (model 8; Adjusted RR:0.96; 95%CI (0.93–0.99); P:0.023).
Discussion
Mild GDM pregnancy, treated with nutritional and healthy lifestyle interventions, is a solid and independent risk factor for 6–18 months of UI development. Second, higher PF Hiatal area distension in the third trimester of pregnancy is a protective factor. Consistent with these findings, our study reports a positive relationship between GDM and increased 6–18 months UI and a negative relationship between higher HA distension and decreased UI. Thus, both markers are opposed, as GDM is a causative agent for UI development. On the other hand, as observed by PF 3DUS, higher HA distensibility is a protective agent.
GDM diagnosis finds a group of women and their offspring at higher risk of diabetes, obesity, and premature cardiovascular disease in the long term [29]. Identifying long-term UI development for mothers with GDM has yet to be fully clarified in the literature. Multivariate regression analyses revealed that GDM, even treated only with healthful dietary patterns and lifestyle intervention, without insulin or oral hypoglycemic drugs therapy, was a solid and independent risk factor for 6–18 months UI (Adjusted RR 8.08; 95% CI 1.17–55.87, P:0.034). By different approaches, previous translational studies have demonstrated that GDM models in pregnant rats are enough to cause hyperglycemic myopathy in PFM and RAM [6, 10, 11], structures directly involved in the urinary continence mechanisms. Hence, this association between GDM and future UI risk results from transient hyperglycemia exposure of the muscles involved in the continence mechanisms [4]. GDM is confirmed as a vital risk factor for UI development [4]. Furthermore, our findings add to previous clinical and experimental studies, elaborated, step by step, through translational research, suggesting hyperglycemic myopathy as the underlying mechanism between GDM and UI [4].
In this study, the PF 3DUS biometrical change assessment, from the second to the third trimester of pregnancy, detected an increase in the PF HA distensibility at the end of the third trimester of pregnancy as a protective factor against 6–18 months UI. This unexpected functional observation by 3DUS, identifying a PFM becoming more distensible or complacent at the end of the third trimester of pregnancy, is not previously reported in the literature. The higher PFM distensibility observed by 3DUS, the lower the PF lesion risk and, consequently, the lower the risk of UI development. This higher PFM distensibility at the 3DUS functional image allows us to display its natural protective role against UI development, confirming classical obstetric knowledge. The protective role of higher PFM distensibility pre-delivery is well described and attributed to physiological preparation for vaginal delivery [5,6,7].
The strengths of our study include its longitudinal design with a 1–2-year follow-up rate, considering GDM as a transient condition with lifelong sequels. All PFM 3DUS was done by the same author, with blinded offline analyses of clinical data and US raw data. By enrolling women during pregnancy, we provided selection criteria such as previous parity, labor induction and second period of labor, and vaginal delivery, which are considered relevant postpartum UI risk factors. In fact, the 93 analyzed women underwent a planned, elective C-section. All GDM patients treated with hypoglycemic drugs were excluded to register a possible maternal PFM physiological adaptation to vaginal delivery. This analysis allows us to obtain the best model after eight backward models of multivariate analyses confirming that GDM, even treated with nutritional and lifestyle intervention, is a solid predictor of 6–18 months UI despite the short period of hyperglycemic status exposure during pregnancy. In this multivariate analysis, the higher PFM distensibility at the end of pregnancy enables us to register a possible maternal PFM physiological adaptation to vaginal delivery.
Limitations: First, our results may not be generalizable and do not apply to other populations, including multiparous or GDM women treated with insulin or hyperglycemic drugs. Second, our strict inclusion criteria of GDM women-only treatment with nutritional and lifestyle interventions probably removed essential risk factors for long-term UI. Third, we do not collect data on the prepregnancy and first trimester due to the first enrollment in the second trimester of gestation.
Our results collectively suggested that universal GDM diagnosis and regular PFM 3DUS functional analysis are good clinical indexes for later UI prediction (concerning GDM diagnosis) or UI protective prediction (concerning higher distensibility of HA). In addition, pregnancy serves as a screening tool for future health risks, opening a window of opportunities to prevent two relevant diseases of our time: GDM and UI [28]. Predicting postpartum UI during pregnancy, with clinical markers like GDM and Pelvic floor biometrical changes by 3DUS, are opportunity to propose clinical interventions to mitigate or prevent postnatal urinary disorders such as UI.
Conclusion
Our results provide objective data that GDM-pregnancies are positively related to increasing the risk of 6–18 months of UI development. Thus, GDM exposure, only with nutritional and healthy lifestyle counseling, is a solid and independent risk predictor for 6–18 months UI, as observed in this cohort of nulliparous women submitted to a planned C-section. While further studies are required to elucidate the mechanism, mild GDM may represent a modifiable risk factor for 6–18 months UI. Opposite results were found for higher Hiatal area distension to rest from the second to the third trimester, related to decreasing the risk of 6–18 months UI. Further studies may determine the best pelvic floor intervention approach during GDM pregnancy to prevent later UI.
Data availability
Due to an ongoing study with preliminary results, the datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Barbosa AMP, Adriano Dias GM, Calderon IMP, RudgeI MVC, Witkin S, Dias A, et al. Urinary incontinence and vaginal squeeze pressure two years post-cesarean delivery in primiparous women with previous gestational diabetes mellitus. Clinics. 2011;66(8):1341–5.
Chuang CM, Lin IF, Horng HC, Hsiao YH, Shyu IL, Chou P. The impact of gestational diabetes mellitus on postpartum urinary incontinence: a longitudinal cohort study on singleton pregnancies. BJOG: An International Journal of Obstetrics & Gynaecology. 2012;119(11):1334–43.
Scholtens DM, Kuang A, Lowe LP, Hamilton J, Lawrence JM, Lebenthal Y, et al. Hyperglycemia and adverse pregnancy outcome follow-up study (HAPO FUS): maternal gestational diabetes Mellitus and Childhood glucose metabolism. Diabetes Care. 2019;42(3):381–92.
Rudge MVC, Souza FP, Abbade JF, Hallur RLS, Marcondes JPC, Piculo F, et al. Study protocol to investigate biomolecular muscle profile as predictors of long-term urinary incontinence in women with gestational diabetes mellitus. BMC Pregnancy Childbirth. 2020;20(1):117.
Prudencio CB, Rudge MVC, Pinheiro FA, Sartorão Filho CI, Nunes SK, Pedroni CR et al. Negative impact of gestational diabetes mellitus on progress of pelvic floor muscle electromyography activity: Cohort study. Palatnik A, editor. PLOS ONE. 2019;14(11):e0223261.
Vesentini G, Barbosa AMP, Damasceno DC, Marini G, Piculo F, Matheus SMM et al. Alterations in the structural characteristics of rectus abdominis muscles caused by diabetes and pregnancy: A comparative study of the rat model and women. Li L, editor. PLOS ONE. 2020;15(4):e0231096.
Sartorão Filho CI, Pinheiro FA, Prudencio CB, Nunes SK, Takano L, Enriquez EMA, et al. Impact of gestational diabetes on pelvic floor: a prospective cohort study with three-dimensional ultrasound during two‐time points in pregnancy. Neurourol Urodyn. 2020;39(8):2329–37.
Vesentini G, Marini G, Piculo F, Damasceno DCC, Matheus SMMMM, Felisbino SLL et al. Morphological changes in rat rectus abdominis muscle induced by diabetes and pregnancy. Braz J Med Biol Res. 2018;51(4).
Piculo F, Marini G, Vesentini G, Morceli G, Damasceno DC, Sobrevia L, et al. Pregnancy-specific urinary incontinence in women with gestational hyperglycaemia worsens the occurrence and severity of urinary incontinence and quality of life over the first year post partum. Eur J Obstet Gynecol Reprod Biol. 2020;252:336–43.
Marini G, Piculo F, Vesentini G, Damasceno DC, Delella FK, Calderon IMP, et al. The influence of hyperglycemia on the remodeling of urethral connective tissue in pregnant rats. Eur J Obstet Gynecol Reproductive Biology. 2018;221:81–8.
Piculo F, Marini G, Barbosa AMP, Damasceno DC, Matheus SMM, Felisbino SL, et al. Urethral striated muscle and extracellular matrix morphological characteristics among mildly diabetic pregnant rats: translational approach. Int Urogynecol J. 2014;25(3):403–15.
Heesakkers JPFA, Gerretsen RRR. Urinary incontinence: Sphincter Functioning from a Urological Perspective. Digestion. 2004;69(2):93–101.
Bakircioglu ME, Sievert KD, Lau A, Lin CS, Lue TF. The effect of pregnancy and delivery on the function and ultrastructure of the rat bladder and urethra. BJU Int. 2000.
Li GY, Cui WS, Zhou F, Gao ZZ, Xin H, Liu T et al. Pathology of urethral fibromuscular system related to parturition-induced stress urinary incontinence and TGF-β1/Smad pathway. Molecular and Cellular Biochemistry. 2012.
Mastrocola R, Reffo P, Penna F, Tomasinelli CE, Boccuzzi G, Baccino FM, et al. Muscle wasting in diabetic and in tumor-bearing rats: role of oxidative stress. Free Radical Biology and Medicine; 2008.
Chen B, Yeh J. Alterations in connective tissue metabolism in stress incontinence and prolapse. J Urol. 2011;186(5):1768–72.
Dietz HP. Pelvic floor Ultrasound: a review. Clin Obstet Gynecol. 2017;60(1):58–81.
Ajala O, Jensen LA, Ryan E, Chik C. Women with a history of gestational diabetes on long-term follow up have normal vascular function despite more dysglycemia, dyslipidemia and adiposity. Diabetes Res Clin Pract. 2015;110(3):309–14.
Cavassini ACM, Lima SAM, Calderon IMP, Rudge MVC. Care cost for pregnant and parturient women with diabetes and mild hyperglycemia. Rev Saude Publica. 2012.
Prudencio CB, Rudge MVC, Pinheiro FA, Sartorão Filho CI, Nunes SK, Pedroni CR et al. Negative impact of gestational diabetes mellitus on progress of pelvic floor muscle electromyography activity: Cohort study. Palatnik A, editor. PloS one. 2019;14(11):e0223261.
Vesentini G, Barbosa AMP, Floriano JF, Felisbino SL, Costa SMB, Piculo F, et al. Deleterious effects of gestational diabetes mellitus on the characteristics of the rectus abdominis muscle associated with pregnancy-specific urinary incontinence. Diabetes Res Clin Pract. 2020;166:108315.
Zhao D, Yuan S, Ma Y, An YX, Yang YX, Yang JK. Associations of maternal hyperglycemia in the second and third trimesters of pregnancy with prematurity. Medicine. 2020;99(17):e19663.
Association AD. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetesd2019. Diabetes Care. 2019;42:13–28.
Organization WH, Group WGD. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy: a World Health Organization Guideline. Diabetes Res Clin Pract. 2014;103(3):341–63.
Hod M, Kapur A, Sacks DA, Hadar E, Agarwal M, Di Renzo GC, et al. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care #. Int J Gynecol Obstet. 2015;131(S3):173.
Hvidman L, Hvidman L, Foldspang A, Mommsen S, Bugge Nielsen J. Correlates of urinary incontinence in pregnancy. Int Urogynecol J. 2002.
Casey BM, Schaffer JI, Bloom SL, Heartwell SF, McIntire DD, Leveno KJ, et al. Study protocol to investigate biomolecular muscle profile as predictors of long-term urinary incontinence in women with gestational diabetes mellitus. Acta Obstet Gynecol Scand. 2011;17(5):1334–43.
Arabin B, Baschat AA. Pregnancy: an underutilized window of opportunity to Improve Long-term maternal and Infant Health—An appeal for continuous Family Care and Interdisciplinary Communication. Front Pead. 2017;5:1.
McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nat reviews Disease primers. 2019;5(1):47.
Dietz HP. Ultrasound imaging of the pelvic floor. Part II: three-dimensional or volume imaging. Ultrasound Obstet Gynecol. 2004;23(6):615–25.
Acknowledgements
We thank all the participants enrolled in the study from the Diamater Study Group, Perinatal Diabetes Research Center, Department of Gynecology and Obstetrics, Tocogynecology Post-graduate Program Botucatu Medical School, UNESP.
Funding
Human resources and infrastructure of the PDRC Botucatu Medical School UNESP. This research was also granted by the São Paulo Research Foundation (FAPESP) #2016/09710-9.
Author information
Authors and Affiliations
Contributions
CISF is the primary author and the leading manuscript text writer. All authors contributed equally to the conception, literature review, and the central manuscript text review. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Regulatory approval was obtained from the Institutional Review Board of Botucatu Medical School (#1.716.895). Written informed consent was obtained from all participants, and all issues related to medical ethics met the requirements of the Helsinki Declaration. All patients involved were properly handled for their morbidities.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sartorao Filho, C.I., Nunes, S.K., Magyori, A.B. et al. The role of Gestational Diabetes Mellitus and pelvic floor 3D-ultrasound assessment during pregnancy predicting urinary incontinence: a prospective cohort study. BMC Pregnancy Childbirth 23, 637 (2023). https://doi.org/10.1186/s12884-023-05932-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-023-05932-8