
Abstract
Background
The Rome IV criteria have been established as an international standard for diagnosing disorders of gut–brain interaction. In this study, we aimed to examine the upper gastrointestinal (GI) endoscopic findings and symptoms of subjects with functional constipation (FC) and irritable bowel syndrome (IBS) of individuals undergoing a medical check-up.
Methods
A total of 13,729 subjects underwent a medical check-up at Osaka City University-affiliated clinic, MedCity21, between April 2018 and March 2019. Among the 5,840 subjects who underwent screening upper GI endoscopy and completed a questionnaire based on the Rome IV criteria, 5,402 subjects were consecutively enrolled after excluding subjects with a large amount of gastric residue (n = 6), those who had previously undergone partial or total gastrectomy (n = 40), or those with daily use of low-dose aspirin (n = 82), nonsteroidal anti-inflammatory drugs (n = 63), or acid secretion inhibitors (n = 308).
Results
Robust Poisson regression analyses adjusted for age, sex, Helicobacter pylori infection status, alcohol intake, and smoking habits showed a significant association between FC and corpus erosion (adjusted prevalence ratio [aPR], 2.93; 95% confidence interval [CI], 1.51–5.67; p < 0.01) and red streaks (aPR, 3.83; 95% CI, 2.53–5.79; p < 0.01), whereas IBS was significantly associated with erosive gastritis (aPR, 8.46; 95% CI, 4.89–14.67; p < 0.01) and duodenitis (aPR, 7.28; 95% CI, 3.64–14.59; p < 0.01). Red streaks tended to be associated with IBS (aPR, 1.96; 95% CI, 1.00–3.83; p = 0.05). Subjects with IBS were the most to complain of both upper and lower GI symptoms and psychological symptoms, followed by those with FC and controls. IBS subjects with erosive gastritis or duodenitis had significantly more complaints of stomachache and feeling stressed than those without erosive gastritis or duodenitis (54.5% vs. 18.8%; p = 0.03 and 66.7% vs. 25.0%; p = 0.01).
Conclusions
Subjects with FC and IBS had a variety of upper GI and psychological symptoms. In the upper GI endoscopic findings, corpus erosion and red streaks were associated with FC, and erosive gastritis, duodenitis, and possibly red streaks were associated with IBS.
Similar content being viewed by others


Background
The Rome IV criteria were established in 2016 as an international standard for diagnosing functional gastrointestinal (GI) disorders, which were recently referred to as disorders of gut–brain interaction (DGBI) [1,2,3]. DGBI is a group of disorders classified by GI symptoms related to a combination of various pathophysiology, such as motility disturbance, visceral hypersensitivity, altered mucosal and immune function, altered gut microbiota, and altered central nervous system processing [4, 5]. Among the DGBI, functional constipation (FC) and irritable bowel syndrome (IBS) are two major categories representing bowel disorders. FC is a bowel disorder in which symptoms of difficult, infrequent, or incomplete defecation predominate, and subjects with FC should not meet the diagnostic criteria for IBS [6]. Meanwhile, IBS is a bowel disorder that leads to recurrent abdominal pain associated with defecation or changes in bowel habits [6]. Although it is known that subjects with IBS frequently have upper GI symptoms [7], few studies have examined the upper GI endoscopic findings in subjects with FC and IBS as both are considered to be associated with the lower GI tract.
Functional dyspepsia (FD) is a gastroduodenal disorder that is characterized by symptoms of postprandial fullness, early satiation, epigastric pain, and epigastric burning associated with the upper GI tract [8]. There have been some reports on the upper GI endoscopic findings in subjects with FD. Chen et al. reported that FD subjects with gastric red streaks exhibited increased somatization and more stressful life events [9], and we previously reported that gastric depressive erosion is more likely to be found in subjects with FD than in healthy controls during a medical check-up [10]. Red streaks, which were originally named Kammrötung in German and has been called variously, such as comb-like redness or linear redness, can be seen from the lesser curvature to the greater curvature of antrum and corpus, and the degree of redness differs depending on the cases. According to the Kyoto Classification of Gastritis that was proposed in 2014 to standardize the upper GI endoscopic diagnosis of gastritis in Japan [11], red streaks are relatively common in Helicobacter pylori-uninfected mucosa, but can also be observed after H. pylori eradication and sometimes in H. pylori-infected mucosa. Depressive erosion is one of the erosive gastritis and can be observed in H. pylori-infected and uninfected mucosa and after H. pylori eradication. Although it has been generally considered that red streaks and depressive erosion are gastric acid-related lesions, they may appear with GI dysfunction. It is possible that they are also associated with other functional GI disorders, known as DGBI.
Therefore, in this study, we aimed to examine the upper GI endoscopic findings and symptoms in subjects with FC and IBS who were diagnosed using a questionnaire based on the Rome IV criteria in a large-scale survey during a medical check-up.
Methods
Study design
This was a single-center, cross-sectional survey of prospective participants.
Study population
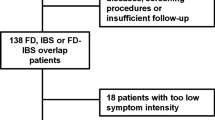
A total of 13,729 subjects underwent a medical check-up at Osaka City University-affiliated clinic, MedCity21, which provides medical examinations and health screening from the perspective of preventive medicine, between April 2018 and March 2019. Among the 5,840 subjects who underwent upper GI endoscopy screening and completed a questionnaire including the Rome IV criteria for FC and IBS with written informed consent, 5,402 subjects were consecutively enrolled after excluding subjects with a large amount of gastric residue (n = 6), those who had previously undergone partial or total gastrectomy (n = 40), or those with daily use of low-dose aspirin (LDA) (n = 82), nonsteroidal anti-inflammatory drugs (NSAIDs) (n = 63), or acid secretion inhibitors (potassium-competitive acid blockers, proton pump inhibitors, or histamine H2 receptor antagonists) (n = 308) (Fig. 1). None of the participants had advanced cancer. The clinical data of the participants were obtained from their medical records and general questionnaires that inquired about lifestyle habits and symptoms during a medical check-up.

Schematic diagram of the study flow. Abbreviations: GI, gastrointestinal; FC, functional constipation; IBS, irritable bowel syndrome; LDA, low-dose aspirin; NSAIDs, nonsteroidal anti-inflammatory drugs
Diagnosis of functional constipation and irritable bowel syndrome
FC was diagnosed based on the Rome IV criteria, as follows: 1) the presence of more than two of the following: straining, lumpy or hard stools (Bristol Stool Form Scale type 1 or 2), sensation of incomplete evacuation, sensation of anorectal obstruction/blockage, manual maneuvers to facilitate defecation during more than one-fourth of defecation episodes, or fewer than three spontaneous bowel movements per week; 2) loose stools rarely present without the use of laxatives; 3) insufficient criteria for IBS; and 4) fulfillment of the criteria for the last 3 months with symptom onset at least 6 months prior.
IBS was diagnosed based on the Rome IV criteria, as follows: 1) recurrent abdominal pain occurring, on average, at least 1 day per week for the last 3 months and associated with more than two of the following: abdominal pain related to defecation, abdominal pain associated with a change in stool frequency, or abdominal pain associated with a change in stool form (appearance), and 2) fulfillment of the criteria for the last 3 months with symptom onset at least 6 months prior.
Examinations of H. pylori infection
We used the anti-H. pylori antibody for serological diagnosis of H. pylori infection (E plate ‘Eiken’ H. pylori antibody; Eiken Chemical Co., Ltd., Tochigi, Japan). Information on H. pylori eradication history of subjects was obtained from their medical records or directly from them during a medical check-up.
Upper gastrointestinal endoscopic findings
Screening with upper GI endoscopy was performed by several expert endoscopists using a 5.4 mm-diameter endoscope for upper GI endoscopy (GIF-XP290N; Olympus Medical Systems Co. Ltd., Tokyo, Japan). The endoscopic procedure was performed without sedation, and esophagus, stomach, and duodenum were observed using white-light imaging with indigo carmine as needed. The endoscopic findings were retrospectively double-checked and determined by one experienced endoscopist with more than 20,000 cases of interpretation to reduce inter-observer variance.
We used the Kimura-Takemoto Classification to evaluate the progress of atrophic gastritis [12]. If the atrophic border did not reach the cardia, the atrophic pattern was classified as closed-type. When the atrophic border extended beyond the cardia, it was classified as open-type.
Erosive gastritis is gastritis with tissue loss in the mucosal layer that penetrates no deeper than the lamina muscularis mucosae (Ul-I). According to the Kyoto Classification of Gastritis, erosive gastritis is further classified into raised erosion, depressive erosion, and corpus erosion. Raised erosion, also known as verrucous gastritis, is an elevated lesion with a shallow central depression that resembles an octopus sucker (Fig. 2A). Depressive erosion is a lesion in which the epithelium is deficient and the epithelial cells around the deficient area are flat (Fig. 2B). In this study, we defined raised erosion and depressive erosion as lesions located in the antrum, to be distinguished from the following corpus erosion. Corpus erosion includes longitudinal or linear depressive erosion or raised erosion located on the ridge of a fold or an extension line in the corpus (Fig. 2C, E). Red streaks are red lines on the mucosal surface that run longitudinally along the crests of the fold almost in parallel (Fig. 2D, E). Duodenitis is an inflammatory change in the duodenal mucosa and spotty, patchy, or band-like redness or erosion without ulceration can be observed (Fig. 2F).

Typical endoscopic images of erosive gastritis, red streaks, and duodenitis. A Raised erosion, B Depressive erosion, C Corpus erosion, D Red streaks, E Corpus erosion on red streaks, F Duodenitis
Objectives
The primary objective of this study was to examine the upper GI endoscopic findings associated with FC or IBS. The secondary objectives were the frequency of GI and psychological symptoms in subjects with FC, those with IBS, and controls and the relationship between symptoms and upper GI endoscopic findings associated with FC or IBS.
Statistical analysis
Data are expressed as median and interquartile range (IQR) for continuous variables and as numbers and percentages for categorical variables. Robust Poisson regression analysis was performed to identify the upper GI endoscopic findings associated with FC or IBS, and the prevalence ratio and 95% confidence interval (CI) were estimated for each variable. The E-value represents the minimum strength for an unmeasured confounder that was associated with both the variables and the outcome, above and beyond the measured confounders, to explain away the association of the variables with the outcome [13]. E-values were calculated using the online E-value calculator (https://www.evalue-calculator.com/) [14]. Symptoms were compared using Pearson’s chi-square test or Fisher’s exact test to compare symptoms between two groups. Statistical calculations and analyses were performed using IBM SPSS Statistics Version 26 (IBM Corporation, Armonk, NY, USA) or R software, version 4.0.2 (The R Foundation for Statistical Computing, Vienna, Austria). P-values < 0.05 were considered statistically significant.
Results
Baseline characteristics of subjects with functional constipation, those with irritable bowel syndrome, and controls
The numbers of subjects who fulfilled the diagnostic criteria for FC and IBS were 108 and 49, respectively. The median ages of subjects with FC, IBS, and controls who had neither FC nor IBS were 51.0 (IQR, 44.0–59.0) years, 49.0 (IQR, 39.0–56.0) years, and 51.0 (IQR, 44.0–60.0) years, respectively. Females were the most frequent in subjects with FC, followed by those with IBS and controls (85.2%, 63.3%, and 50.4%, respectively). The median body mass index was lower in subjects with FC, followed by that in controls and subjects with IBS (21.0, IQR, 19.5–23.3; 22.3, IQR, 20.3–24.7; and 22.4, IQR, 20.0–25.2, respectively). There were no differences in H. pylori infection status among the subjects with FC, those with IBS, and controls.
Among the lifestyle habits in subjects with FC, drinking alcohol more than 5 days a week was the least common in subjects with FC, followed by that in those with IBS and controls (13.0%, 26.5%, and 26.7%). Exercising for ≥ 30 min at least twice a week for ≥ 1 year was the least common in subjects with FC, followed by that in those with IBS and controls (16.7%, 20.4%, and 26.6%, respectively). As for the lifestyle habits of subjects with IBS, getting enough rest by sleeping was the least common in subjects with IBS, followed by that in those with FC and controls (32.7%, 48.1%, and 59.3%, respectively). Subjects who skipped breakfast ≥ 3 times a week were more likely to have IBS, followed by controls and subjects with FC (26.5%, 13.7%, and 13.0%, respectively). Subjects who ate 2 h before going to bed ≥ 3 times a week were more likely to have IBS, followed by controls and subjects with FC (46.9%, 27.6%, and 22.2%, respectively) (Table 1).
These characteristics of subjects with FC and IBS were consistent with our previous studies [15, 16].
Upper gastrointestinal endoscopic findings associated with functional constipation or irritable bowel syndrome
Erosive gastritis, including raised erosion, depressive erosion, and corpus erosion (51.0%, 30.6%, 10.2%, and 18.4%, respectively) and duodenitis (24.5%) were the most common in subjects with IBS. In contrast, red streaks (48.1%) were the most common in subjects with FC (Table 2).
Robust Poisson regression analyses adjusted for age, sex, H. pylori infection status, alcohol intake, and smoking habits showed a significant association between FC and corpus erosion (adjusted prevalence ratio [aPR], 2.93; 95% CI, 1.51–5.67; p < 0.01) and red streaks (aPR, 3.83; 95% CI, 2.53–5.79; p < 0.01) (Table 3). Adjusted robust Poisson regression analyses revealed that erosive gastritis (aPR, 8.46; 95% CI, 4.89–14.67; p < 0.01) and duodenitis (aPR, 7.28; 95% CI, 3.64–14.59; p < 0.01) were significantly associated with IBS. Even in separate analyses of erosive gastritis, raised erosion (aPR, 6.70; 95% CI, 3.66–12.26; p < 0.01), depressive erosion (aPR, 5.28; 95% CI, 2.19–12.71; p < 0.01), and corpus erosion (aPR, 6.92; 95% CI, 3.42–13.98; p < 0.01) were all significantly associated with IBS. Red streaks tended to be associated with IBS (aPR, 1.96; 95% CI, 1.00–3.83; p = 0.05), although it was not statistically significant (Table 4).
Sensitivity analysis
We calculated the E-value for aPR and the corresponding lower limit of the 95% CI as a sensitivity analysis to evaluate robustness. In association with FC, the E-value was 5.31 (E-value for the lower limit of 95% CI = 2.39) for corpus erosion and 7.12 (E-value for the lower limit of 95% CI = 4.50) for red streaks. In association with IBS, the E-value was 16.40 (E-value for the lower limit of 95% CI = 9.25) for erosive gastritis, 3.33 (E-value for the lower limit of 95% CI = 1.00) for red streaks, and 14.04 (E-value for the lower limit of 95% CI = 6.74) for duodenitis.
Gastrointestinal and psychological symptoms in subjects with functional constipation, those with irritable bowel syndrome, and controls
Subjects with IBS were the most to complain of both upper GI symptoms, such as heartburn, nausea, stomachache, and heavy stomach (10.2%, 8.2%, 42.9%, and 28.6%, respectively), and lower GI symptoms, such as abdominal pain and abdominal bloating/distension (100.0% and 42.9%, respectively), followed by those with FC and controls (Fig. 3A). Furthermore, subjects with IBS were the most to complain of psychological symptoms, such as feeling stressed, annoyance, lack of motivation, fatigue upon waking, and feeling depressed (53.1%, 26.5%, 24.5%, 40.8%, and 28.6%, respectively), followed by those with FC and controls (Fig. 3B).

Gastrointestinal and psychological symptoms in subjects with functional constipation, irritable bowel syndrome, and controls. A Gastrointestinal symptoms, B Psychological symptoms, C Symptoms with or without corpus erosion or red streaks in subjects with functional constipation, D Symptoms with or without erosive gastritis or duodenitis in subjects with irritable bowel syndrome; Abbreviations: IBS, irritable bowel syndrome; FC, functional constipation; *P < 0.05
The relationship between symptoms and upper gastrointestinal endoscopic findings associated with functional constipation or irritable bowel syndrome
We further investigated whether GI and psychological symptoms differed with or without corpus erosion or red streaks in subjects with FC, and the symptoms were not remarkably different depending on the presence of corpus erosion or red streaks (Fig. 3C). We then investigated whether GI and psychological symptoms differed with or without erosive gastritis or duodenitis in subjects with IBS. IBS subjects with erosive gastritis or duodenitis had significantly more complaints of stomachache and feeling stressed than those without erosive gastritis or duodenitis (54.5% vs. 18.8%; p = 0.03 and 66.7% vs. 25.0%; p = 0.01) (Fig. 3D).
Discussion
It was notably identified in this study that erosive gastritis, red streaks, and duodenitis, which were the upper GI endoscopic findings considered to be caused by gastric acid or other etiologies, were associated with FC or IBS, although they are classified as bowel disorders in DGBI, according to the Rome IV criteria. No significant differences in the H. pylori infection status were present among the subjects with FC, IBS, and controls, and variables of age, sex, H. pylori infection status, alcohol intake, and smoking habits that may influence these endoscopic findings were adjusted in multivariate analyses. Moreover, we excluded participants who were taking LDA or NSAIDs that could cause erosive gastritis, red streaks, and duodenitis and those who were taking acid secretion inhibitors that could heal the lesions that would have appeared with FC or IBS. Thus, it is suggested that these endoscopic findings are closely associated with FC or IBS.
Red streaks were significantly associated with FC and had a tendency to be associated with IBS. Corpus erosion was significantly associated with both FC and IBS. Therefore, red streaks and corpus erosion may be common upper GI findings in subjects with FC and IBS. Although the etiology of the red streaks is unknown, it is considered that functional abnormality in GI tract is possible. Red streaks appear on the longitudinal folds, and mucosa on the ridge of folds is highly exposed to abnormal gastric peristalsis and gastric acid. Red streaks may be caused by local congestion on the ridge of folds during peristalsis as superficial blood vessels are observed, while inflammatory cell infiltration is not observed in the histopathological findings of the lesion [17]. Motility disturbance is the major pathophysiology of FC, and autonomic dysfunction, degeneration of the myenteric plexus, and decreased levels of neurotransmitters, such as serotonin, substance P, nitric oxide, vasoactive intestinal peptide, and calcitonin gene-related peptide, have been observed in patients with slow-transit constipation [6, 18,19,20,21,22,23,24]. These factors involved in FC can also cause motility disturbance in IBS, affecting not only the lower GI motility but also gastric motility. Corpus erosion is found in both H. pylori-positive and negative mucosa, and sometimes appears as longitudinal or linear erosion, accompanied by red streaks in the corpus. Therefore, it is reasonable to assume that corpus erosion is also associated with FC and IBS. In the lower GI tract, Gupta et al. reported that constipation did not show any increased risk of significant findings on colonoscopy from a retrospective review of the national endoscopic database [25]. To our knowledge, this is the first report demonstrating the upper GI findings of FC.
Meanwhile, duodenitis and other components of erosive gastritis, such as raised erosion and depressive erosion, were also significantly associated with IBS. Consistent with our results, Loosen et al. reported that the most common overlapping GI diagnoses with IBS are intestinal infectious diseases, gastritis/duodenitis, esophageal diseases, FD, and other diseases of the stomach and duodenum in subjects with IBS using the disease analyzer database in Germany [26]. There are reports demonstrating the dysbiosis of mucosa-associated microbiota in duodenum in subjects with IBS [27, 28], suggesting that altered duodenal microbiota can be one of the causes of duodenitis in subjects with IBS.
Furthermore, we examined the symptoms in subjects with FC and IBS. Although FC and IBS are classified as bowel disorders, a substantial proportion of subjects with both disorders had upper GI symptoms. Subjects with FC complained more of a variety of GI and psychological symptoms than control group, suggesting that this disease is one of the DGBI. Similarly, Wald et al. reported that the psychological distress score was high in patients with normal-transit constipation [29]. Considering that there were no significant differences in GI and psychological symptoms between FC subjects with corpus erosion or red streaks and those without corpus erosion or red streaks in this study, these endoscopic findings were not responsible for symptoms in subjects with FC, and endoscopic findings and symptoms may independently originate from motility disturbance or psychological distress. On the other hand, subjects with IBS more complained of GI and psychological symptoms than those with FC and controls. Consistent with our results, it has been reported that subjects with IBS frequently have upper GI and mental symptoms in addition to lower GI symptoms [7] and GI symptoms are generally more severe in subjects with IBS than in those with constipation [30]. Among the upper GI symptoms, stomachache was more common in subjects with erosive gastritis or duodenitis, suggesting that low-grade inflammation and immunological alterations may manifest as stomachache in IBS subjects with visceral hypersensitivity [31, 32]. Visceral hypersensitivity includes allodynia and hyperalgesia, and subjects with IBS experience strong visceral pain even with stimuli that do not cause pain or only mild pain in healthy individuals [33]. Altered central nervous system or brain function has been demonstrated in patients with IBS using brain imaging [34], and it may partially explain the symptoms in subjects with IBS. Lee et al. reported that patients with IBS had higher level of psychological symptoms, such as depression or anxiety [35], and those with more severe symptoms might meet the diagnostic criteria for psychiatric comorbidities, such as depressive or anxiety disorders. Among the psychological symptoms in subjects with IBS, feeling stressed was more common in subjects with erosive gastritis or duodenitis. Strong stress could be a cause of erosive gastritis and duodenitis in subjects with IBS since it has been shown that stress increases the level of gastric acid and decreases the motility in animal studies [36, 37]. In addition, subjects with IBS had more disturbed lifestyle habits such as inability to get enough rest by sleep in this study, which is consistent with previous reports that noted the prevalence of sleep disorders to be higher in patients with IBS [38, 39]. These symptoms and disturbed lifestyle habits may result in impairment of quality of life in subjects with IBS [40].
This study had some limitations. First, it was conducted at a single medical check-up institution, and the characteristics of the subjects might have been biased. The participants who underwent a medical check-up were highly conscious of their health, and their overall health status was generally good. Moreover, very elderly and very young individuals usually do not undergo medical check-ups. Therefore, the prevalence of FC and IBS in this study was lower than that in outpatients with FC and IBS in a hospital setting. Second, the questionnaire used in this study was based on self-reported measures by participants, and issues such as missed reporting and providing inaccurate information were unavoidable. Third, IBS subtypes cannot be diagnosed in this study since a questionnaire used for diagnosing FC and IBS did not inquire about IBS subtyping. Fourth, accurate H. pylori infection status is difficult to be determined because only anti-H. pylori antibody is measured during a single medical check-up. Although anti-H. pylori antibody ≥ 10 U/mL without eradication therapy generally indicates current H. pylori infection, it is ideal to perform more than two types of examinations to increase the accuracy. However, our study has strengths in that the cross-sectional survey was conducted prospectively for all participants to avoid selection bias and FC and IBS were strictly diagnosed baesd on the latest international standard Rome IV criteria. This large-scale survey could accurately assess the upper GI endoscopic features of FC and IBS in subjects during a medical check-up.
Conclusions
In conclusion, in the upper GI endoscopic findings, corpus erosion and red streaks were significantly associated with FC, and erosive gastritis and duodenitis were significantly associated with IBS. Red streaks were also possibly associated with IBS. A substantial proportion of subjects with FC and IBS had a variety of GI and psychological symptoms, and IBS subjects with erosive gastritis or duodenitis significantly complained of stomachache and feeling stressed. These findings suggest that some subjects with these minor abnormalities in the upper GI endoscopy in addition to troublesome symptoms may have FC or IBS. Therefore, we should not overlook these subjects during a medical check-up.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- GI:
-
Gastrointestinal
- DGBI:
-
Disorders of gut–brain interaction
- FC:
-
Functional constipation
- IBS:
-
Irritable bowel syndrome
- FD:
-
Functional dyspepsia
- LDA:
-
Low-dose aspirin
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- IQR:
-
Interquartile range
- CI:
-
Confidence interval
- aPR:
-
Adjusted prevalence ratio
References
Drossman DA, Hasler WL. Rome IV-functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–61.
Schmulson MJ, Drossman DA. What is new in Rome IV. J Neurogastroenterol Motil. 2017;23(2):151–63.
Suzuki H. The application of the Rome IV criteria to functional esophagogastroduodenal disorders in Asia. J Neurogastroenterol Motil. 2017;23(3):325–33.
Drossman DA. Functional gastrointestinal disorders: history, pathophysiology, clinical features and Rome IV. Gastroenterology. 2016;150(6):1262-79.
Takagi T, Naito Y, Inoue R, Kashiwagi S, Uchiyama K, Mizushima K, et al. Differences in gut microbiota associated with age, sex, and stool consistency in healthy Japanese subjects. J Gastroenterol. 2019;54(1):53–63.
Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, et al. Bowel disorders. Gastroenterology. 2016;150(6):1393-407.
Svedlund J, Sjodin I, Dotevall G, Gillberg R. Upper gastrointestinal and mental symptoms in the irritable bowel syndrome. Scand J Gastroenterol. 1985;20(5):595–601.
Stanghellini V, Chan FK, Hasler WL, Malagelada JR, Suzuki H, Tack J, et al. Gastroduodenal Disorders. Gastroenterology. 2016;150(6):1380–92.
Chen TS, Luo JC, Chang FY. Psychosocial-spiritual factors in patients with functional dyspepsia: a comparative study with normal individuals having the same endoscopic features. Eur J Gastroenterol Hepatol. 2010;22(1):75–80.
Tanaka F, Tominaga K, Fujikawa Y, Morisaki T, Otani K, Hosomi S, et al. Association between functional dyspepsia and gastric depressive erosions in Japanese subjects. Intern Med. 2019;58(3):321–8.
Haruma K, Kato M, Inoue K, Murakami K, Kamada T. Kyoto Classification of gastritis: Nihon Medical Center; 2017.
Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy. 1969;1(3):87–96.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: Introducing the E-Value. Ann Intern Med. 2017;167(4):268–74.
Mathur MB, Ding P, Riddell CA, VanderWeele TJ. Web Site and R package for computing E-values. Epidemiology. 2018;29(5):e45–7.
Otani K, Watanabe T, Takahashi K, Nadatani Y, Fukunaga S, Hosomi S, et al. Prevalence and risk factors of functional constipation in the Rome IV criteria during a medical check-up in Japan. J Gastroenterol Hepatol. 2021;36(8):2157–64.
Otani K, Watanabe T, Takahashi K, Ominami M, Nadatani Y, Fukunaga S, et al. a questionnaire-based survey on the etiopathogenesis of chronic constipation during a medical check-up in Japan. J Clin Biochem Nutr. 2022;70(2):205–11.
Kawabe TM, S.; Ogura, K.; Yamaji, Y.; Okamoto, M.; Yoshida, H.; Shiratori, Y.; Omata, M. Antral red streaking is a negative endoscopic sign for helicobacter pylori infection. Dig Endosc. 2002;14:87–92.
Shekhar C, Monaghan PJ, Morris J, Issa B, Whorwell PJ, Keevil B, et al. Rome III functional constipation and irritable bowel syndrome with constipation are similar disorders within a spectrum of sensitization, regulated by serotonin. Gastroenterology. 2013;145(4):749–57; quiz e13–4.
Knowles CH, Scott SM, Wellmer A, Misra VP, Pilot MA, Williams NS, et al. Sensory and autonomic neuropathy in patients with idiopathic slow-transit constipation. Br J Surg. 1999;86(1):54–60.
Krishnamurthy S, Schuffler MD, Rohrmann CA, Pope CE 2nd. Severe idiopathic constipation is associated with a distinctive abnormality of the colonic myenteric plexus. Gastroenterology. 1985;88(1 Pt 1):26–34.
Tzavella K, Riepl RL, Klauser AG, Voderholzer WA, Schindlbeck NE, Muller-Lissner SA. Decreased substance P levels in rectal biopsies from patients with slow transit constipation. Eur J Gastroenterol Hepatol. 1996;8(12):1207–11.
Cortesini C, Cianchi F, Infantino A, Lise M. Nitric oxide synthase and VIP distribution in enteric nervous system in idiopathic chronic constipation. Dig Dis Sci. 1995;40(11):2450–5.
El-Salhy M, Norrgard O, Spinnell S. Abnormal colonic endocrine cells in patients with chronic idiopathic slow-transit constipation. Scand J Gastroenterol. 1999;34(10):1007–11.
Sjolund K, Fasth S, Ekman R, Hulten L, Jiborn H, Nordgren S, et al. Neuropeptides in idiopathic chronic constipation (slow transit constipation). Neurogastroenterol Motil. 1997;9(3):143–50.
Gupta M, Holub J, Knigge K, Eisen G. Constipation is not associated with an increased rate of findings on colonoscopy: results from a national endoscopy consortium. Endoscopy. 2010;42(3):208–12.
Loosen SH, Kostev K, Jordens MS, Luedde T, Roderburg C. Overlap between irritable bowel syndrome and common gastrointestinal diagnoses: a retrospective cohort study of 29,553 outpatients in Germany. BMC Gastroenterol. 2022;22(1):48.
Li G, Yang M, Jin Y, Li Y, Qian W, Xiong H, et al. Involvement of shared mucosal-associated microbiota in the duodenum and rectum in diarrhea-predominant irritable bowel syndrome. J Gastroenterol Hepatol. 2018;33(6):1220–6.
Giamarellos-Bourboulis E, Tang J, Pyleris E, Pistiki A, Barbatzas C, Brown J, et al. Molecular assessment of differences in the duodenal microbiome in subjects with irritable bowel syndrome. Scand J Gastroenterol. 2015;50(9):1076–87.
Wald A, Hinds JP, Caruana BJ. Psychological and physiological characteristics of patients with severe idiopathic constipation. Gastroenterology. 1989;97(4):932–7.
Shah ED, Almario CV, Spiegel BMR, Chey WD. Lower and upper gastrointestinal symptoms differ between individuals with irritable bowel syndrome with constipation or chronic idiopathic constipation. J Neurogastroenterol Motil. 2018;24(2):299–306.
Ohman L, Simren M. Pathogenesis of IBS: role of inflammation, immunity and neuroimmune interactions. Nat Rev Gastroenterol Hepatol. 2010;7(3):163–73.
Enck P, Aziz Q, Barbara G, Farmer AD, Fukudo S, Mayer EA, et al. Irritable bowel syndrome. Nat Rev Dis Primers. 2016;2:16014.
Simren M, Tornblom H, Palsson OS, Van Oudenhove L, Whitehead WE, Tack J. Cumulative effects of psychologic distress, visceral hypersensitivity, and abnormal transit on patient-reported outcomes in irritable bowel syndrome. Gastroenterology. 2019;157(2):391–402 e2.
Tillisch K, Mayer EA, Labus JS. Quantitative meta-analysis identifies brain regions activated during rectal distension in irritable bowel syndrome. Gastroenterology. 2011;140(1):91–100.
Lee C, Doo E, Choi JM, Jang SH, Ryu HS, Lee JY, et al. The increased level of depression and anxiety in irritable bowel syndrome patients compared with healthy controls: systematic review and meta-analysis. J Neurogastroenterol Motil. 2017;23(3):349–62.
Nahata M, Saegusa Y, Sadakane C, Yamada C, Nakagawa K, Okubo N, et al. Administration of exogenous acylated ghrelin or rikkunshito, an endogenous ghrelin enhancer, improves the decrease in postprandial gastric motility in an acute restraint stress mouse model. Neurogastroenterol Motil. 2014;26(6):821–31.
Hayase M, Takeuchi K. Gastric acid secretion and lesion formation in rats under water-immersion stress. Dig Dis Sci. 1986;31(2):166–71.
Miglis MG. Autonomic dysfunction in primary sleep disorders. Sleep Med. 2016;19:40–9.
Tobaldini E, Costantino G, Solbiati M, Cogliati C, Kara T, Nobili L, et al. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci Biobehav Rev. 2017;74(Pt B):321–9.
Kawamura Y, Yamamoto S, Funaki Y, Ohashi W, Yamamoto K, Ozeki T, et al. Internet survey on the actual situation of constipation in the Japanese population under 70 years old: focus on functional constipation and constipation-predominant irritable bowel syndrome. J Gastroenterol. 2020;55(1):27–38.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
KO designed the study, analyzed the data, and drafted the paper; TW supervised this study, and revised the paper; KT (Kanae Takahashi) analyzed the data; YN (Yuji Nadatani), MO, SF (Shusei Fukunaga), SH, NK, FT, YN (Yasuaki Nagami), KT (Koichi Taira), TK, SF (Shinya Fukumoto), and YF reviewed the manuscript and provided valid inputs regarding the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of Osaka City University Graduate School of Medicine (No. 3928) on December 27, 2017. Written informed consent was obtained from each participant included in the study. We disclosed information about this study on the webpage of the institution, and the participants had the opportunity to opt out. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki for medical research involving human subjects and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Otani, K., Watanabe, T., Takahashi, K. et al. Upper gastrointestinal endoscopic findings in functional constipation and irritable bowel syndrome diagnosed using the Rome IV criteria: a cross-sectional survey during a medical check-up in Japan. BMC Gastroenterol 23, 140 (2023). https://doi.org/10.1186/s12876-023-02784-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-023-02784-6