
Abstract
Background
Our aim was to evaluate the influence of staged goal directed therapy (GDT) on postoperative pulmonary complications (PPCs), intraoperative hemodynamics and oxygenation in patients undergoing Mckeown esophagectomy.
Methods
Patients were randomly divided into three groups, staged GDT group (group A, n = 56): stroke volume variation (SVV) was set at 8–10% during the one lung ventilation (OLV) stage and 8–12% during the two lung ventilation (TLV) stage, GDT group (group B, n = 56): received GDT with a target SVV of 8–12% During the entire surgical procedure, and control group (group C, n = 56): conventional fluid therapy was administered by mean arterial pressure (MAP), central venous pressure (CVP), and urine volume. The primary outcome was the incidence of postoperative pulmonary complications within Postoperative days (POD) 7. The secondary outcomes were postoperative lung ultrasound (LUS) B-lines artefacts (BLA) scoring, incidence of other complications, the length of hospital stay, intraoperative hemodynamic and oxygenation indicators included mean arterial pressure (MAP), heart rate (HR), cardiac index (CI), cardiac output (CO), oxygenation index (OI), respiratory indices (RI), alveolar-arterial oxygen difference (Aa-DO2).
Results
Patients in group A and group B had a lower incidence of PPCs (7/56 vs. 17/56 and 9/56 vs. 17/56, p < 0.05), and a fewer B-lines score on postoperative ultrasound (4.61 ± 0.51 vs. 6.15 ± 0.74 and 4.75 ± 0.62 vs. 6.15 ± 0.74, p < 0.05) compared to group C. The CI, CO, MAP, and OI were higher in group A compared to group B and group C in the stage of thoracic operation. During the abdominal operation stage, patients in group A and group B had a better hemodynamic and oxygenation indicators than group C.
Conclusions
In comparison to conventional fluid therapy, intraoperative staged GDT can significantly reduce the incidence of postoperative pulmonary complications in patients undergoing McKeown esophagectomy, facilitating patient recovery. Compared to GDT, it can improve intraoperative oxygenation and stabilize intraoperative hemodynamics in patients.
Trial registration
This study was registered in the Chinese Clinical Trial Registry on 24/11/2021 (ChiCTR2100053598).
Similar content being viewed by others

Introduction
The incidence of esophageal cancer in East Asia is approximately 9–21 per 100,000 [1]. Currently, surgical treatment remains the primary method for resectable esophageal cancer. However, esophageal cancer surgery generally entails significant trauma and prolonged duration, with a high proportion of elderly patients and a greater incidence of comorbidities such as cardiorespiratory conditions. Consequently, the incidence of postoperative complications and mortality are relatively high. According to the research by Finks et al. in 2011, the 30-day mortality rate after esophagectomy in Western U.S. hospitals ranged from 7 − 9%, with a 90-day mortality rate as high as 13% [2]. Among these patients, approximately 50% of those undergoing radical esophagectomy died due to postoperative pulmonary complications (PPCs) [3].
Excessive intraoperative fluid loading may lead to respiratory failure, intestinal dysfunction, and anastomotic leakage [4]. Low blood volume can increase the incidence of perioperative complications, such as cardiac ischemia and renal failure, and may jeopardize the healing of newly constructed anastomoses [5]. Goal-directed therapy (GDT) is a perioperative fluid replacement method that predicts positive responses to volume expansion based on dynamic hemodynamic parameters and optimizes total blood volume and tissue oxygenation by administering fluids and vasoactive drugs (positive inotropic agents, vasopressors, and vasodilators) according to set parameters. In recent years, some dynamic parameters, such as stroke volume variation (SVV) and pulse pressure variation, have been used in GDT to reduce postoperative complications and improve patient outcomes [5]. In a multi-center study by Mukai et al., the SVV-guided GDT (targeting an SVV of 8 − 12%) was applied to esophagectomy, and the results showed that the incidence of postoperative complications and mortality in the experimental group were significantly lower compared to the control group (systolic pressure > 90 mmHg) [6].
Phased GDT is primarily applied in surgeries where patients exhibit significant pathophysiological changes during the procedure. Kazuyuki et al. adopted a phased GDT approach in liver transplantation surgeries and demonstrated that it could reduce intraoperative bleeding [7]. In the study conducted by Hao Xiaoyan et al., phased GDT was shown to be beneficial for the recovery of renal function after kidney transplantation [8].
In recent years, with the advancement of minimally invasive surgery, the McKeown radical esophagectomy has been increasingly utilized for the treatment of upper esophageal cancer above the tracheal bifurcation. This procedure involves three incisions through the right chest, upper abdomen, and left neck [9]. The main steps of the McKeown esophagectomy are as follows: first, under one-lung ventilation (OLV), the thoracic segment of the esophagus is freed using a thoracoscope and mediastinal lymph nodes are dissected. Subsequently, the patient is placed in the supine position with two-lung ventilation, and a laparoscope is used to free the stomach. Finally, the cervical esophagus is dissected and cut off, followed by an esophagogastric left cervical anastomosis. The intraoperative ventilation methods and body positions can exert different influences on the value of SVV. Studies have shown that SVV decreases during protective one-lung ventilation in thoracic surgery, and a lower threshold is recommended when using goal-directed fluid therapy [10]. The optimal threshold for predicting fluid responsiveness during OLV is 10% [11]. During abdominal surgery stages, CO2 pneumoperitoneum and the reverse Trendelenburg position can cause significant hemodynamic changes, specifically a reduction in cardiac output, an increase in systemic and pulmonary vascular resistance, a rise in arterial pressure, and a decrease in venous return leading to an elevation in SVV. Studies have reported that the optimal threshold for predicting fluid responsiveness during laparoscopic surgery is 12% [12].
Therefore, this study aims to explore the impact of different surgical stages on SVV, proposing a staged GDT approach, with the target SVV set at 8–10% during single-lung ventilation and 10–12% during bi-lateral ventilation. The study will compare the staged GDT with single-stage GDT and conventional fluid therapy, aiming to observe any differences in intraoperative hemodynamic parameters, oxygenation functions, and postoperative PPCs occurrence.
Methods
Study design
This study was approved by the Ethics Committee of the First Affiliated Hospital of China University of Science and Technology (Ref:2022-ky-027). This study was registered in the Chinese Clinical Trial Registry on 24/11/2021 (ChiCTR2100053598). We used the CONSORT checklist when writing our report. 180 patients from February 2022 to September 2022. All patients were assigned in a 1:1:1 ratio to the staged GDT group (group A), GDT group (group B), and conventional fluid therapy group (group C). The randomization was stratified by sequential blocking based on the computer random number generator. The anesthesiologists responsible for intraoperative management were informed of the patient’s’ grouping, whereas the rest of the research team and the patients were blinded to the grouping.
Inclusion criteria were as follows: (1) those who were classified ASA II–III, (2) those who were scheduled for McKeown esophagectomy. Exclusion criteria were as follows: (1) patients with severe liver or kidney dysfunction (Blood creatinine > 442µmol/L, Child C), (2) those with cardiac dysfunction (New York Heart Association (NYHA) III-V) or abnormal preoperative pulmonary function (forced expiratory volume in 1 s < 50% of predicted), (3) those with severe arrhythmia, (4) those with intraoperative blood loss > 500 mL or those who required blood transfusion.
Anesthesia procedure
The patients received a restricted diet 6–8 h prior to surgery. Before the induction of anesthesia, a standardized catheterization of the right internal jugular vein was performed, and a 20-G arterial catheter (B. Braun Medical Inc, Bethlehem, PA, USA) was inserted into the radial artery of the left forearm. Physiological parameters such as heart rate (HR), mean arterial pressure (MAP), central venous pressure (CVP), pulse oximetry (SpO2), partial pressure of end-tidal carbon dioxide (PetCO2), body temperature, and bispectral index (BIS) were continuously monitored and recorded. In addition, the LiDCO system (LiDCO, Ltd, London, UK) was utilized to continuously monitor SVV, cardiac index (CI), CO, and stroke volume (SV). Then etomidate 0.3–0.4 mg·kg-1, sufentanil 0.5–0.7 µg·kg-1, and rocuronium 1.0 mg·kg-1 were administered intravenously for induction of general anesthesia. Intravenous infusion of propofol (3–6 mg·kg-1·h-1) and remifentanil (0.1–0.3 µg·kg-1·min-1) were maintained throughout the procedure to achieve the BIS target value of 45–60. After the induction of anesthesia, a right bronchial occluder (Yichang Humanwell, China) was located by bronchoscopy. Ventilation mode was set to volume controlled mode, the ventilation parameters are set as follows. In OLV, tidal volume (VT): 7 mL·kg-1; FiO2: 100%; expiratory time ratio (I/E):1:1.5. In TLV, tidal volume (VT): 8 mL·kg-1; FiO2: 50%; expiratory time ratio (I/E):1:2. Positive end-expiratory pressure (PEEP) of 5 cmH2O was applied. The ventilation parameter were adjusted to maintain PetCO2 at 35–45 mmHg, and the nasopharynx temperature was maintained at > 36 °C by a fluid warmer and medical warming blanket. As needed, additional muscle relaxants and analgesics were intermittently administered, and all patients used patient-controlled intravenous analgesia (PCIA) postoperatively.
Surgical procedures
First, the patient is placed in the left lateral position with OLV, and thoracic procedures are performed under thoracoscopy, including the dissection of the azygos vein arch and the thoracic esophagus. Lymph nodes in the paraesophageal, subcarinal, bilateral recurrent laryngeal nerve, and inferior pulmonary ligament are removed based on the tumor location and extent of invasion. Subsequently, the patient is placed in the reverse Trendelenburg position with TLV, and laparoscopy is used to free the stomach and create a tubular stomach. Finally, an incision is made in front of the left sternocleidomastoid muscle to complete the dissection, severance of the cervical esophagus, and esophagogastric anastomosis.
Intraoperative hemodynamic management protocols
Groups A, B, and C received a continuous infusion of lactated Ringer’s solution at a rate of 3 mL·kg-1·h-1 after induction of anesthesia. Group A followed the protocol illustrated in Fig. 1. During OLV, when SVV ≥ 10% persisted for more than 3 min, colloid 4 ml·kg-1 (6% hydroxyethyl starch 130/0.4, Fresenius Kabi AG, Bad Homburg, Germany) was administered over 15 min. The above process was repeated until the SVV < 10%. An infusion of dobutamine was given at 3–5 µg·kg-1·min-1 if SVV drop < 2% after infusion or SVV < 10% with concurrent CI < 2.5 L·min-1·m-2. Additionally, norepinephrine was pumped at 4–10 µg·min-1 if the MAP fell below 65 mmHg after fluid infusion and CI ≥ 2.5 L·min·m2. The infusion was slowed or stopped when SVV < 8%. Furthermore, hemodynamic parameters were evaluated every 5 min. During the TLV, above protocol was applied with the target SVV set at 8–12%. Similarly, group B followed the same protocol as group A, with the exception that the target SVV range was set at 8–12% during the whole surgery. Conversely, in group C, hemodynamic management was determined by the discretion of the attending anesthesiologist, if necessary, aiming at MAP > 65 mmHg, HR 60,100 bpm, CVP 6–12 mmH2O, and the urine output > 0.5 mL/kg/h.
MAP, HR, CI, and CO were recorded before surgery (T0), 30 min after OLV (T1), 60 min after OLV (T2), 30 min after TLV (T3), and at the end of surgery (T4). In addition to these parameters, the total infusions of crystalloids and colloids, blood loss, urine output, and vasoactive drug requirements were recorded and analyzed.

Goal-directed fluid therapy protocol. SVV, stroke volume variation; CI, cardiac index; MAP, mean arterial pressure
Primary outcomes
The primary outcome was the incidence rate of pulmonary complications within 7 d after surgery. The occurrence of pulmonary complications was assessed using the Melbourne Group Scale Version 2 (MGS-2), which comprises eight parameters. The diagnosis of pulmonary complications was confirmed if four or more of the following criteria were met: (1) body temperature > 38 °C, (2) white blood cell count > 11.0 × 109 L-1 or administration of antibiotics for respiratory infections, (3) pneumonia or pulmonary infection diagnosed by physicians, (4) chest radiograph showing atelectasis/consolidation, (5) yellow-green sputum of a different nature from the preoperative one, (6) positive sputum culture results, (7) blood oxygen saturation (SpO2) < 90% on room air. or (8) readmission to the intensive care unit (ICU) for respiratory problems or staying in the ICU for > 36 h [13].
Blood gas analysis
Radial artery blood was collected at T0, T1, T2, T3, and T4. Additionally, the oxygenation index (OI = PaO2 / FiO2), alveolar (A) - arterial (a) oxygen partial pressure difference (PA-aDO2 = FiO2 (PB - PH2O) - PaCO2 / R - PaO2, PB, Atmospheric Pressure; R, respiratory quotient), and respiratory index (RI = PA - aDO2 / PaO2) were calculated and recorded.
Lung ultrasonography (LUS)
At T0, 2 h after surgery (T5), and 48 h after surgery (T6), LUS was performed according to international evidence-based recommendations for point-of-care LUS based on a simplified four-sector scan [14] by a skilled operator using a portable ultrasound device. The left thorax was examined to avoid potential confounding factors from subcutaneous emphysema and surgical effects. The thorax was partitioned into four areas on one side: upper anterior, upper lateral, lower anterior, and lower lateral, delimited by the anterior axillary line and the fourth intercostal space. B-lines artifacts (BLAs) are defined as vertical, laser-like, hyperechoic images that originate from the pleural line and move with respiration. The number of B-lines detected in each area was tallied and subsequently scored. A score of 0 points was assigned for no BLA, 1 point for 1–3 BLAs, 2 points for 3–5 BLAs, and 3 points for > 5 BLAs. The total B-lines score was calculated as the sum of the scores of the four areas.
Statistical analysis
This study is a randomized controlled trial, with the incidence of postoperative pulmonary complications as the primary endpoint. Based on previous research reports on similar cases, the incidence of pulmonary complications in esophagectomy cases treated with conventional fluid therapy is approximately 35%. Similarly, the incidence of pulmonary complications after GDT is approximately 10%.The estimated incidence of pulmonary complications in the staged GDT group is 5%.the sample size was calculated using PASS V.15 software, setting α = 0.05 (two-tailed) and (1-β) = 0.99. The total sample size required was found to be 165 cases. Taking into account potential dropouts, the sample size was increased to 180 cases, with 60 cases in each group.
Statistical analysis was conducted using SPSS 15.0. Continuous data are presented as mean ± standard deviation, and their normality was assessed using the Kolmogorov-Smirnov test. For normally distributed continuous data, t-tests (paired or unpaired) were used for analysis, while for non-normally distributed continuous data, the Mann-Whitney U test and Wilcoxon signed-rank test were employed for unpaired and paired analyses, respectively. Repeated measures one-way analysis of variance (ANOVA) and Bonferroni-correction was used to assess significant differences among three groups. The analysis of categorical data employed the chi-square test or Fisher’s exact test. P < 0.05 was considered statistically significant.
Results
Patient demographic characteristics
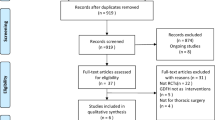
This study initially included 212 patients underwent McKeown esophagectomy. However, 32 patients were later excluded from the study (Fig. 2). Ultimately, a total of 168 patients(70.3% male; age range 41–84 years) completed the study protocol and were ultimately enrolled in this study.

CONSORT flow diagram of participants allocation
Table 1 summarizes the preoperative demographic and laboratory characteristics of the enrolled patients. It was found that baselined characteristics showed no statistically significant differences observed among the three groups.
Postoperative outcomes
The primary outcomes of this study are presented in Table 2. Among 168 patients, 33 developed PPCs on POD 7. The incidence of PPCs was significantly lower in groups A and B than in group C (7/56 vs. 17/56, and 9/56 vs. 17/56, p < 0.05), while no differences were observed between groups A and B (7/56 vs. 9/56, p = 0.29). No differences were seen among the three groups with respect to other postoperative complications or the initiation of oral intake. Notably, in group C, 4 patients were readmitted to the ICU postoperatively, and 2 patients died due to wound infections. Furthermore, there was no differences on postoperative hospital stays in three groups (8.7 ± 0.8 vs. 9.0 ± 0.9 vs. 9.0 ± 1.2, p = 0.74).
Intraoperative data and fluid management
Table 3 summarizes the intraoperative data, fluid management, and vasoactive drug administration in groups A, B, and C. No significant differences were observed in the operation time, anesthesia time, OLV time, time to extubation, blood loss, transfusion, or urine output among the three groups. Group C received a significantly higher volume of crystalloid infusion than groups A and B (1121.4 ± 371.1 vs. 1801.8 ± 373.4 and 1108.9 ± 351.2 vs. 1801.8 ± 373.4, p < 0.05). In contrast, the volume of colloids was significantly higher in groups A and B than in group C (944.6 ± 295.4 vs. 551.8 ± 120.6 and 775.0 ± 196.6 vs. 551.8 ± 120.6, p < 0.05). The dose of dobutamine was more in groups A and B than in group C (14.1 ± 2.7 vs. 4.2 ± 1.5 and 15.4 ± 3.0 vs. 4.2 ± 2.2, p < 0.05). Conversely, the bolus of noradrenaline usage in groups A and B was lower than that in group C (175.4 ± 59.1 vs. 234.2 ± 73.9 and 179.1 ± 52.1 vs. 234.2 ± 73.9, p < 0.05). The volume of colloids administered during OLV was the highest in group A, followed by group B, and the lowest in group C (614.3 ± 128.5 vs. 487.5 ± 196.6 vs. 276.8 ± 89.3, p < 0.05). The volume of crystalloids administered during OLV was significantly higher in group C than in groups A and B (533.9 ± 163.2 vs. 835.7 ± 179.3 and 530.4 ± 133.4 vs. 835.7 ± 179.3, p < 0.05). Furthermore, there were no significant differences in the volumes of noradrenaline and dobutamine administered during OLV between groups A and B.
Blood gas analysis and intraoperative hemodynamic data
Table 4 presents the results of blood gas analysis data. During OLV, groups A and B experienced a significant decrease in the OI compared with baseline data (p < 0.05), along with significant increases in the PA-aDO2 and RI. Compare with group C the PaO2/FiO2 and RI were significantly higher than those in groups A and B At T1, T2, and T3 (p < 0.05), whereas the PaO2/FiO2 was higher in group A than that in group B during OLV (p < 0.05).
As shown in Fig. 3, the HR was comparable among the three groups at all time points. However, In group C, the CI, and CO were significantly lower than in groups A and B (p < 0.05). Additionally, at T1 and T2, the, CI and CO were higher in group A than in group B ( (p < 0.05).

Variables of Intraoperative hemodynamic data. (A) HR; (B) MAP; (C) CI; (D) CO. Data are represented as mean ± SD. HR, heart rate; MAP, mean arterial pressure; CI, cardiac index; CO, cardiac output.* Group A versus group B(p < 0.05), † Group A versus group C (p < 0.05), ‡ Group B versus group C (p < 0.05)
LUS results
As depicted in Fig. 4, LUS for preoperative baseline revealed no BLAs in any of the four thoracic regions (score = 0). At T5, all groups demonstrated an elevated B-lines score. However, the B-lines score in groups A and B was significantly lower than that in group C at T5 (4.52 ± 0.63 vs. 5.93 ± 0.71 and 4.95 ± 0.88 vs. 5.93 ± 0.71, p < 0.05). Notably, a decrease in the B-lines score was observed at T6(4.14 ± 0.55 vs. 4.18 ± 0.54 vs. 3.95 ± 0.45, p = 0.41), and no significant differences were observed between groups A and B at all time points.

Postoperative BLA scores. T5, 2 h after operative; T6, 48 h after operative
Discussion
Esophagectomy remains a challenging surgical procedure for both surgeons and anesthesiologists. A growing body of evidence indicates that Enhanced Recovery After Surgery (ERAS) can improve postoperative outcomes for numerous major surgeries, including esophagectomy [15], with perioperative fluid management being a key component. Insufficient fluid administration may lead to insufficient tissue perfusion, potentially resulting in anastomotic leakage [16], while excessive fluid administration may increase the incidence of pulmonary complications [17]. It has been reported that anastomotic leakage and pulmonary complications account for 80% of all postoperative complications following esophagectomy [18]. GDT is a perioperative fluid replacement method that predicts positive responses after volume expansion based on dynamic hemodynamic parameters and optimizes total blood volume and tissue oxygenation by administering fluids and vasoactive drugs (positive inotropic agents, vasopressors, and vasodilators) according to parameters. GDT is primarily used for high-risk patients during the perioperative period, targeting certain dynamic hemodynamic parameters and achieving objectives through the administration of fluids and vasoactive drugs (positive inotropic agents, vasopressors, and vasodilators) to optimize cardiac output and tissue perfusion. In past studies, GDT has been extensively applied in general surgery, orthopedics, cardiothoracic surgery, and vascular surgery, demonstrating a positive impact on accelerating patient recovery.
In the past decade, SVV has been the most frequently recommended and the most suitable target parameter for GDT. It can dynamically reflect blood volume and effectively predict the body’s response to fluid challenges. The generation of SVV is a result of changes in intra-thoracic pressure during positive pressure ventilation, leading to variations in arterial pressure between the inspiratory and expiratory phases. Compared to currently commonly used indicators for monitoring patient volume, such as central venous pressure and mean arterial pressure, it is less affected by factors such as posture and pneumoperitoneum, thus its reliability and sensitivity are higher than those of these traditional indicators [19]. Since the McKeown esophagectomy requires the opening of the chest, there has been debate about whether SVV can be applied to open-heart surgery. However, studies have shown that even under open-chest conditions, SVV can still accurately predict fluid responsiveness [20]. This is because SVV is primarily influenced by blood flow from the non-operating side. During open-heart surgery, the surgeon opens the chest on the operating side, compromising its integrity. In addition, due to hypoxic pulmonary vasoconstriction and the effects of left lateral positioning, the lung on the operating side collapses, reducing blood flow. This results in less influence on SVV from the operating side. Conversely, the non-operating side maintains its integrity throughout the procedure. Under the influence of mechanical ventilation, periodic changes occur in intra-thoracic pressure, causing corresponding periodic changes in venous return, leading to changes in SVV.
The normal range for SVV is typically less than 10 − 13%, with values exceeding this range potentially indicating insufficient capacity. This critical threshold may vary under different surgical conditions. In McKeown esophagectomy, single-lung ventilation (OLV) techniques are required to provide the surgeon with a clear view and adequate space for maneuverability. During OLV, a low tidal volume ventilation strategy is commonly adopted to avoid lung injury caused by mechanical ventilation. The size of the tidal volume is a key factor affecting SVV. Numerous studies have shown that the absolute value of SVV is directly related to it, and both values greater than 10 ml/kg and less than 5 ml/kg decrease the accuracy of SVV [21]. Therefore, in this study, a tidal volume of 7 ml/kg was used during OLV. Although a lower tidal volume may lead to a reduction in the value of SVV and affect its accuracy in predicting fluid responsiveness, studies have shown that a low tidal volume (6 ml/kg) during OLV does not statistically affect the value of SVV [22]. In an earlier study that used SVV to differentiate fluid responsiveness during OLV, the optimal threshold was > 10% [11]. Therefore, in this study, the target SVV threshold for Group A during OLV was set at a lower range of > 10%. Dynamic indicators based on fluid responsiveness and other optimization parameters are more effective than any one of them alone [23]. Therefore, this study used both CI and SVV as target parameters for GDT to achieve an appropriate fluid load. Fluid responsiveness is generally defined as an increase in SVI or CI by 15–20% after the administration of 250 to 500 ml of fluid in most cases [24]. Considering that changes in stroke volume caused by respiration are essentially unchanged, after conversion, the value of SVV decreases by approximately 2%. Therefore, this study selected a 2% decrease in SVV as an indicator of fluid responsiveness.
OLV can cause ventilation-related lung injury. Research has analyzed the predictive factors for postoperative complications in patients undergoing McKeown esophagectomy and found that the incidence of postoperative complications in patients with OLV < 150 min is lower than that in patients with OLV ≥ 150 min [25]. In this study, we used an occluder as a means of pulmonary isolation, but the surgical procedure can sometimes lead to its displacement. We aimed to avoid severe hypoxemia during the adjustment process, so we used 100% FiO2 during OLV, Parameters such as OI, PA-aDO2, and RI can better reflect pulmonary oxygenation and gas exchange functions [26]. In this study, at time points T1, T2, and T3, patients in groups A and B were superior to those receiving conventional fluid therapy in these parameters. This suggests that in McKeown esophagectomy, compared to traditional fluid management, GDT can improve intraoperative alveolar gas exchange efficiency. In previous studies, GDT protocols have been shown to reduce pulmonary vascular resistance and protect right ventricular function in patients with severe pulmonary hypertension [27, 28]. Therefore, it is speculated that GDT improves pulmonary oxygenation and gas exchange by reducing pulmonary vascular resistance and minimizing hydrostatic pressure. In this study, it was observed that the OI during OLV in group A was higher than that in group B. This may be due to the maintenance of a lower SVV level (8–10%) in group A, as well as a higher cardiac output, ultimately improving intrapulmonary shunt flow and reducing venous mixing. This result suggests that maintaining a higher SVV during OLV may lead to insufficient tissue perfusion. Low microcirculatory perfusion and tissue hypoxia in the anastomotic region during McKeown esophagectomy are considered important factors for gastroesophageal anastomotic failure [29, 30].
Extravascular lung water accumulation is a manifestation of Acute Respiratory Distress Syndrome (ARDS), and it is considered a marker of pulmonary edema [31]. Research by Philipp et al. demonstrated a good correlation between the number of ultrasound B-lines and extravascular lung water [32, 33]. In previous studies, higher LUS has been reported as a predictor for PPCs [34]. In this study, both Group A and Group B showed lower BLA. This may be attributed to the reduction in total fluid intake, particularly crystalloid fluid, caused by GDT, as well as the maintenance of better tissue perfusion intraoperatively. Previous research has indicated that excessive fluid input can lead to the degradation of endothelial glycocalyx, increased vascular permeability, and subsequent fluid leakage, resulting in an increase in extravascular lung water [35]. The reason for choosing hydroxyethyl starch as the fluid for volume expansion in this study is that animal experiments have shown that hydroxyethyl starch can reduce the degradation of endothelial glycocalyx and protect vascular endothelial cell function compared to crystalloid fluids [36]. Moreover, hydroxyethyl starch solutions are easier to maintain gastrointestinal microcirculatory perfusion and oxygen partial pressure than crystalloids [37]. The use of hydroxyethyl starch (HES) In a recent study, it was reported that HES may increase the risk of kidney injury in critically ill patients [38], and research by John et al. showed that HES has no advantage over crystalloid solutions in reducing mortality in critical patients [39]. However, a recent large cohort study showed no significant correlation between the use of HES and the incidence of postoperative acute kidney injury [40]. In this study, no patients were found to have renal failure.
In this study, the MGS-2 diagnostic tool was utilized to assess Postoperative Complications (PPCs), aiming to minimize the impact of vague definitions. The MGS-2 tool demonstrated high reliability and effectiveness in diagnosing PPCs during thoracotomy [41]. The findings of this study indicate that both the single-stage GDT and the staged GDT groups exhibited positive effects in reducing PPCs when compared to traditional fluid therapy. This is somewhat similar to the results of the study by Mukai A et al. on the impact of perioperative GDT combined with ERAS on the outcomes after esophagectomy [6]. In this study, the incidence rate of postoperative pneumonia was significantly reduced in both the single-stage GDT and the staged GDT groups. Previous research has shown that postoperative pneumonia is independently associated with higher hospital mortality rates and poorer long-term survival [42]. There were no significant differences among the three groups in terms of hospital length of stay or time to first meal. This may be because the duration of hospital stay after esophagectomy is a complex and multifaceted outcome, related to anastomotic healing conditions, gastrointestinal function recovery, and other complications. PPCs are not the sole factor influencing the duration of hospital stay after surgery.
The findings of this study indicate that the fluid input in Group A and Group B patients was significantly reduced. When expanding the blood volume under conditions of normal blood volume, approximately two-thirds of the infused volume rapidly shifts to the interstitial space [43]. This suggests that GDT can prevent unnecessary fluid input and reduce fluid leakage during surgery, thereby lowering the incidence of postoperative pulmonary complications. Additionally, there were differences in the use of vasoactive drugs among the three groups, with higher doses of norepinephrine observed in Group C, and higher doses of dobutamine observed in Group A and Group B. This may be a result of the less clarified indications in the group C. In McKeown esophagectomies, the gastric conduit top is dependent on microcirculation, posing a risk of ischemia. All tissue perfusion studies showed a significant decrease in blood flow to the gastric region at the anastomosis, tissue oxygenation, or both [44]. Although the reasons remain unclear, vasoconstrictor drugs have long been considered a potential cause of impaired microvascular blood flow and gastric anastomotic failure due to hypoxemia [45]. We believe that accurately administering different types and doses of fluids and vasoactive drugs at various time points based on changes in patient condition can prevent excessive fluid input while better maintaining tissue perfusion.
This study presents several limitations. Firstly, this research is a single-center study, and the findings may require broader applicability to other medical settings. Multicenter studies could address this issue and provide more representative samples for the research of phased GDT. Secondly, in designing the objectives for different stages of phased GDT, the primary focus was on the impact of ventilation methods on SVV, without considering other factors such as body position and pneumoperitoneum. Thirdly, this study employed hydroxyethyl starch as an embolic agent, the usage approval of which has been revoked in many countries recently, thereby limiting the study’s results to a certain extent. Lastly, the assessment of pulmonary complications was limited to the first 7 days post-surgery, without long-term follow-up.
Conclusions
In comparison to conventional fluid therapy, intraoperative staged GDT can significantly reduce the incidence of postoperative pulmonary complications in patients undergoing McKeown esophagectomy, facilitating patient recovery. Compared to GDT, it can improve intraoperative oxygenation and stabilize intraoperative hemodynamics in patients.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BIS:
-
Bispectral Index
- BLA:
-
B-Lines Artifacts
- CI:
-
Cardiac Index
- CO:
-
Cardiac output
- ERAS:
-
Enhanced Recovery After Surgery
- FiO2 :
-
Fraction of inspired oxygen
- GDT:
-
Goal Directed Therapy
- LUS:
-
Lung Ultrasound Examination
- MGS:
-
Melbourne Group Scale
- OLV:
-
One Lung Ventilation
- POD:
-
Postoperative days
- PPCs:
-
Postoperative Pulmonary Complications
- RI:
-
Respiratory Index
- SVV:
-
Stroke Volume Variation
References
Manabe N, Matsueda K, Haruma K. Epidemiological Review of Gastroesophageal Junction Adenocarcinoma in Asian countries [J]. Digestion. 2022;103(1):29–36.
Finks JF, Osborne NH, Birkmeyer JD. Trends in hospital volume and operative mortality for high-risk surgery [J]. N Engl J Med. 2011;364(22):2128–37.
D’Journo XB, Boulate D, Fourdrain A, et al. Risk prediction model of 90-Day mortality after esophagectomy for Cancer [J]. JAMA Surg. 2021;156(9):836–45.
Salling SL, Jensen JH, Mosegaard SB, et al. Risk stratification for postoperative pulmonary complications following major cardiothoracic or abdominal surgery: validation of the PPC risk prediction score for physiotherapist’s clinical decision making. [J] Clin Respir J. 2023;17(3):229–40.
Aaen AA, Voldby AW, Storm N, et al. Goal directed fluid therapy in emergency abdominal surgery: a randomised multicentre trial [J]. Br J Anaesth. 2021;127(4):521–31.
Mukai A, Suehiro K, Watanabe R, et al. Impact of intraoperative goal-directed fluid therapy on major morbidity and mortality after transthoracic oesophagectomy: a multicentre, randomised controlled trial [J]. Br J Anaesth. 2020;125(6):953–61.
Mizunoya K, Fujii T, Yamamoto M et al. Two-stage goal-directed therapy protocol for non-donor open hepatectomy: an interventional before-after study [J]. J Anesth 2019 Dec, 33(6): 656–64.
Xiaoyan H, Hui W, Shoulin G. Application of phased goal-Directed Fluid Management in Anesthesia for renal transplant surgery [J]. Int J Anesth Resusc. 2019;40(10):42–4.
Ju WM, Shu GG, Xue Q, et al. Comparison of short-term outcomes and three years urvival between total minimally invasive McKeown and dualincision esophagectomy [J]. Thorac Cancer. 2017;8(2):80–7.
Lema Tome M, De la Gala FA, Piñeiro P, et al. Behaviour of stroke volume variation in hemodynamic stable patients during thoracic surgery with one-lung ventilation periods [J]. Braz J Anesthesiol. 2018;68(3):225–30.
Fu Q, Duan M, Zhao F. Evaluation of stroke volume variation and pulse pressure variation as predictors of fluid responsiveness in patients undergoing protective one-lung ventilation [J]. Drug Discov Ther. 2015;9(4):296–302.
Zlicar M, Novak-Jankovic V, Blagus R, et al. Predictive values of pulse pressure variation and stroke volume variation for fluid responsiveness in patients with pneumoperitoneum [J]. J Clin Monit Comput. 2018;32(5):825–32.
Reeve JC, Nicol K, Stiller K, et al. Does physiotherapy reduce the incidence of postoperative complica-tions in patients following pulmonary resection via thoracotomy? A protocol for a randomised controlled trial [J]. Cardiothorac Surg. 2008;3:48.
Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence-based recommendations for point-of-care lung ultrasound [J]. Intensive Care Med. 2012;38:577–91.
Ding H, Xu J, You J, et al. Effects of enteral nutrition support combined with enhanced recovery after surgery on the nutritional status, immune function, and prognosis of patients with esophageal cancer after Ivor-Lewis operation [J]. J Thorac Dis. 2020;12(12):7337–45.
Wu H, Wang W, Zhao G, et al. Effect of intraoperative fluid administration on perioperative outcomes in patients undergoing McKeown esophagogastrectomy [J]. Chin J Cancer Res. 2019;31(5):742–8.
Giglio M, Biancofiore G, Corriero A, et al. Perioperative goal-directed therapy and postoperative compli-cations in different kind of surgical procedures: an updated meta analysis [J]. J Anesth Analg Crit Care. 2021;15(1):26.
Geropoulos G, Moschonas S, Fanariotis G, et al. Anastomotic leak and perioperative outcomes of Esophagectomy for Esophageal Cancer during the COVID-19 pandemic: a systematic review and Meta-analysis [J]. Med (Kaunas). 2023;60(1):31.
Xu H, Shu SH, Wang D, Chai XQ, et al. Goal-directed fluid restriction using stroke volume variation and cardiac index during one-lung ventilation: a randomized controlled trial [J]. J Thorac Dis. 2017;9(9):2992–3004.
Zhang J, Chen CQ, Lei XZ, et al. Goal-directed fluid optimization based on stroke volume variation and cardiac index during one-lung ventilation in patients undergoing thoracoscopy lobectomy operations: a pilot study [J]. Clin (Sao Paulo). 2013;68:1065–70.
He F, Li X, Thapa S, et al. Evaluation of volume responsiveness by pulse pressure variability and inferior vena cava dispensability index at different tidal volumes by mechanical ventilation [J]. Braz J Med Biol Res. 2019;52(9):27–8.
Alvarado Sánchez JI, Caicedo Ruiz JD, Diaztagle Fernández JJ, et al. Predictors of fluid responsiveness in critically ill patients mechanically ventilated at low tidal volumes: systematic review and meta-analysis [J]. Ann Intensive Care. 2021;11(1):28.
Huan S, Dai J, Song S, Zhu G, Ji Y, Yin G. Stroke volume variation for predicting responsiveness to fluid therapy in patients undergoing cardiac and thoracic surgery: a systematic review and meta-analysis [J]. BMJ Open. 2022;12(5):e051112.
Marik PE, Cavallazzi R, Vasu T, et al. Dynamic changes in arterial waveform derived variables and fluid responsiveness inmechanically ventilated patients: a systematic review of the literature [J]. Crit Care Med. 2009;37:2642–7.
Horinouchi T, Yoshida N, Shiraishi S, et al. Relationship between the severity of emphysematous change in the lung and morbidity after esophagectomy for esophageal cancer: a retrospective study on a novel strategy for risk prediction [J]. Thorac Cancer. 2024;15(1):15–22.
Howe CA, MacLeod DB, Wainman L, et al. Validation of a Noninvasive Assessment of Pulmonary Gas Exchange during Exercise in Hypoxia [J]. Chest. 2020;158(4):1644–50.
Taniguchi H, Sasaki T, Fujita H, et al. Effects of goal-directed fluid therapy on enhanced postoperative recovery: an interventional comparative observational study with a historical control group on oesoph-agectomy combined with ERAS program [J]. Clin Nutr ESPEN. 2018;23:184–93.
Liu J, Nahrwold DA, Serdiuk AA, et al. Intraoperative goal-Directed Anesthetic Management of the patient with severe pulmonary hypertension [J]. Am J Case Rep. 2019;20:998–1001.
Zehetner J, DeMeester SR, Alicuben ET, et al. Intraoperative Assessment of Perfusion of the gastric graft and correlation with anastomotic leaks after esophagectomy [J]. Ann Surg. 2015;262(1):74–8.
Jogiat UM, Sun WYL, Dang JT, et al. Gastric ischemic conditioning prior to esophagectomy reduces anastomotic leaks and strictures: a systematic review and meta-analysis. Surg Endosc [J]. 2022;36(7):5398–407.
Gavelli F, Shi R, Teboul JL, et al. Extravascular lung water levels are associated with mortality: a systematic review and meta-analysis [J]. Crit Care. 2022;26(1):202.
Nair S, Sauthoff H. Assessing Extravascular Lung Water with Ultrasound: A Tool to individualize Fluid Management? [J]. J Intensive Care Med. 2020;35(11):1356–62.
Shyamsundar M, Attwood B, Keating L, et al. Clinical review: the role of ultrasound in estimating extra-vascular lung water [J]. Crit Care. 2013;17:237.
Szabó M, Bozó A, Darvas K, et al. The role of ultrasonographic lung aeration score in the prediction of postoperative pulmonary complications: an observational study [J]. BMC Anesthesiol. 2021;21(1):19.
Zhao H, Zhu Y, Zhang J, et al. The Beneficial Effect of HES on Vascular Permeability and its relation-ship with endothelial glycocalyx and intercellular Junction after hemorrhagic shock [J]. Front Pharmacol. 2020;11:597.
Ando T, Uzawa K, Yoshikawa T, et al. The effect of tetrastarch on the endothelial glycocalyx layer in early hemorrhagic shock using fluorescence intravital microscopy: a mouse model [J]. J Anesth. 2023;37(1):104–18.
Behem CR, Friedheim T, Holthusen H, et al. Goal-directed colloid versus crystalloid therapy and microcirculatory blood flow following ischemia/reperfusion [J]. Microvasc Res. 2024;152:154.
Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis [J]. N Engl J Med. 2012;367(2):124–34.
Myburgh JA, Finfer S, Bellomo R, et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care [J]. N Engl J Med. 2016;374(13):1298.
Yang MJ, Chen N, Ye CY, et al. Association between hydroxyethyl starch 130/0.4 administration during noncardiac surgery and postoperative acute kidney injury: a propensity score-matched analysis of a large cohort in China [J]. J Clin Anesth. 2024;96:111493.
Agostini P, Naidu B, Cieslik H, et al. Comparison of recognition tools for postoperative pulmonary complications following thoracotomy [J]. Physiotherapy. 2011;97(4):278–83.
Xi-Zeng QD-WZ, Zhen-Tao Y, et al. Analysis of early mortality rate and composition of death causes after esophageal carcinoma surgery [J]. J Practical Oncol. 2008;5:456–8.
Rehm M, Haller M, Orth V, et al. Changes in blood volume and hematocrit during acute preoperative volume loading with 5% albumin or 6% hetastarch solutions in patients before radical hysterectomy [J]. Anesthesiology. 2011;95:849–56.
Davies SJ, Mythen M. Hemodynamic and intestinal microcirculatory changes in a phenylephrine corrected Porcine Model of hemorrhage [J]. Anesth Analg. 2021;133(4):1060–9.
Fang WT, Chen WH, Fan LM, et al. Causes and prevention of anastomotic leakage after esophagectomy and reconstruction through different routes for esophageal cancer. [J]. Zhonghua Wei Chang Wai Ke Za Zhi. 2015;8(3):217–9.
Acknowledgements
Not applicable.
Funding
This study was funded by the Hubei Chen Xiaoping science and Technology Development Foundation (CXPJJH121003-2216).
Author information
Authors and Affiliations
Contributions
MZ and YHX designed the study protocol. CY and YJS analyzed the data and wrote the manuscript.YY and CY collected the data. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of China University of Science and Technology (Ref:2022-ky-027). The written informed consents were obtained from all patients before participation.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, C., Shi, Y., Zhang, M. et al. Impact of staged goal-directed fluid therapy on postoperative pulmonary complications in patients undergoing McKeown esophagectomy: a randomized controlled trial. BMC Anesthesiol 24, 330 (2024). https://doi.org/10.1186/s12871-024-02719-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-024-02719-y