
Abstract
Background
Decreased bioavailability of nitric oxide (NO) under hypoxic conditions can lead to endothelial dysfunction. NO supplementation may protect endothelial function in ischemia-reperfusion (IR) injury. Therefore, a meta-analysis of randomized controlled trials (RCTs) was performed to verify the protective effect of NO donors on endothelium in IR injury.
Methods
Medline, Embase, Cochrane Library, and Web of Science databases were searched from inception to April 1, 2023. The specific inclusion criteria were as follows: (1) RCTs; (2) trials comparing NO donors with placebo control groups; and (3) trials reporting the effects of these interventions on vascular endothelial functional outcomes in IR injury. Random-effects models were used to assess pooled effect sizes, which were expressed as standardized mean differences (SMD).
Results
Seven studies satisfied the inclusion criteria and consisted of a total of 149 participants. NO donors were protective of endothelial function in IR injury (SMD: − 1.60; 95% confidence interval [CI]: − 2.33, − 0.88, P < 0.0001; heterogeneity [I2 = 66%, P = 0.001]). Results of the subgroup analysis showed the following: absence of protective effect of NO donor use following ischemia on endothelial function in IR injury − 1.78 (95% CI: − 2.50, − 1.07) and loss of protective effect on endothelial function after prolonged NO donor use − 0.89 (95% CI: − 2.06, 0.28).
Conclusion
The short-period use of NO donors before the onset of ischemia can protect endothelial function in IR injury.
Similar content being viewed by others

Introduction
Ischemia/reperfusion (I/R) is a complex pathophysiological process that leads to organ damage in many clinical conditions (e.g., myocardial infarction, organ transplantation, and cardiac arrest). Concurrently, I/R induces vascular endothelial dysfunction through multiple mechanisms, including cytotoxicity caused by pH changes, oxidative stress caused by overproduction of reactive oxygen species (ROS), and endothelial nitric oxide synthase (eNOS)–nitric oxide (NO) inhibition [1,2,3]. Endothelial cells have been shown to play a key role in the damage sustained after ischemia and reperfusion [4]. Following the discovery of endogenous (endothelial-derived) NO and the recognition of its importance in the control of vascular homeostasis [5], it was speculated that NO donors might be able to provide IR protection [6]. NO production via NOS is inhibited under hypoxic or anoxic conditions [7, 8]. However, as oxygen is being consumed, many proteins involved in the oxidation process at basal oxygen levels may become reductases to convert nitrite to NO. This shift in biological role often occurs in proteins containing heme or molybdenum pterin cofactors such as hemoglobin, myoglobin, and xanthine oxidase (XO) [9,10,11,12]. In hypoxic conditions, NO donors increase the amount of NO in the body independent of the L-arginine-NO synthase pathway, making it an attractive alternative therapy to help improve endothelial dysfunction secondary to NO insufficiency. In animal models, NO donors have been shown to reduce I/R injury [13, 14]. However, exogenous NO donor administration has potentially deleterious effects; for example, NO has been shown to play a key role in apoptosis by reacting with superoxide to form peroxynitrite, inducing tyrosine nitration and deleterious protein changes [15, 16]. There is also evidence that treatment with most organic nitrates at clinical doses impairs responsiveness to stimuli of endothelial-derived NO release [17]. Endothelial dysfunction has been observed in animal studies and in humans during extended nitroglycerin (GTN) and isosorbide mononitrate (ISMN) treatment [18]. These contradictory studies suggest that the dominant role of NO in I/R on endothelial function is unclear. Anderson et al. [19] invented the flow-mediated dilation (FMD) method at the brachial artery, which is presently an established, rapid, accurate, and noninvasive assessment method to measure and reflect endothelial function in subjects.
The aim of this article is to illustrate the effect of NO donors on endothelial function (FMD) in human subjects with I/R injury by systematically analyzing evidence from randomized controlled trials (RCTs).
Methods
In this systematic review, meta-analyses were performed in strict accordance with the criteria stated in PRISMA. The protocols retrieved for this study were registered on the PROSPERO platform (registration number CRD42022365781).
Search strategy
We searched the Cochrane Library, Medline, Web of Science, and Embase databases from the establishment of the database until April 1, 2023 using a search strategy consisting of a combination of subject terms and free words. Subject terms included reperfusion injury, nitric oxide donors, endothelium. (The complete search strategy for Medline is in the supplementary materials). We searched relevant local and international clinical research trial registry databases and consulted experts in the field to identify potential unpublished data. We also screened the reference lists of all articles selected for inclusion to identify additional studies for potential inclusion.
Inclusion and exclusion criteria
We included all human clinical studies in which NO donor agents were administered during I/R. Inclusion criteria were as follows: (1) RCTs; (2) studies in which flow-mediated dilation of the brachial artery was measured by ultrasound, namely the FMD method, to reflect vascular endothelial function; (3) trials comparing NO donors with placebo control groups; and (4) trials reporting the effects of these interventions on vascular endothelial function outcomes in I/R. Exclusion criteria included the following: (1) nonclinical studies; (2) lack of complete FMD data; (3) no available full text; (4) presence of other influences besides NO; (5) reviews, newsletters, or editorials.
Literature selection and data extraction
Two reviewers (Yao and Dou) independently performed an initial screening for relevance by reviewing titles and abstracts of identified articles for potential eligibility. Following the screening for relevance, the two reviewers compared their results. In cases of discrepancies, a third reviewer (Xie) assessed the abstracts, and a consensus was reached among the three reviewers. All studies that were considered potentially relevant were retrieved, and the complete manuscripts were reviewed for inclusion.
Following the completion of the study selection, the following data was extracted from the included studies: (1) authors and publication date of the study; (2) type of study; (3) study subjects and their health status; (4) drugs used, their doses, etc.; (5) number of people included in the study; (6) time course of NO donor application; (7) FMD baseline and endpoint values; and (8) FMD baseline and endpoint change values if available. When the exact data was not available, and only graphs and bars were available, we approached the authors to obtain unpublished data. If unsuccessful, a digital scale was used to estimate the data in the graph or bar chart, and the original data was derived based on estimation according to the axes [20]. As the main observed outcome of this meta-analysis is the change in FMD from baseline to endpoint after the use of NO donor agent, the change values were extracted directly if they were directly provided in the literature, and where only baseline and endpoint values were available, the change values were calculated according to the method proposed in the Cochrane Handbook for Systematic Reviews of Interventions for calculating change values in the meta-analysis and Follman’s theory [21]. The following formula was applied for the calculation of the FMD change values:
Baseline | Final | Change | |
|---|---|---|---|
Experimental Intervention | MeanE,b, | MeanE,f, | MeanE,change, |
SDE,b | SDE,f | SDE,change | |
Control Intervention | MeanC,b, | MeanC,f, | MeanC,change, |
SDC,b | SDC,f | SDC,change |
An estimated correlation value of R = 0.50 was used to provide conservative estimates based on the assumption that this value would minimize the error in the effect size estimates.
Risk of bias and quality assessment
Two researchers (Yao and Dou) assessed the quality of each study using the Cochrane Risk of Bias tool to assess the following: selection bias (random sequence generation and allocation concealment), performance bias (blinding of participants and researchers to the intervention), detection bias (blinding of outcome assessment), attrition bias (completeness of outcome data, including handling of attrition and data exclusion in analysis), and reporting bias (selective outcome reporting) [22].
Data synthesis and analysis
After obtaining the FMD change values and standard deviations for each study, data on the number of participants, FMD change values, and standard deviations in the experimental and control groups of each study were entered into the REVMAN software, and a random effects model was used to provide a more conservative estimate of the pooled effect size [23]. The standardized mean difference (SMD) and 95% confidence interval (95% CI) for each included study in this meta-analysis were obtained. The software was also used to calculate the final results of the meta-analysis and their p-values, plot a forest plot, and derive the values for heterogeneity between studies in this meta-analysis. Heterogeneity is expressed as I2. According to international standards, I2 > 50% indicates significant heterogeneity between studies while a value of less than 50% indicates the absence of heterogeneity between studies [24].
Exploring the source of heterogeneity was one of the important purposes of meta-analysis, and we selected the following factors as potential sources of heterogeneity and explored their effects on the outcome (FMD change values) via subgroup analysis: (1) timing of NO donor agent administration (i.e., pre-ischemic treatment or post-ischemic treatment) and (2) duration of NO donor agent administration (i.e., short-term treatment or long-term treatment, based on a 24-h cutoff). We first performed a sensitivity analysis to determine their effect on the stability of the results. Next, we applied subgroup analysis and sequentially divided the included studies into two different subgroups according to potential influencing factors, which were entered into the REVMAN software to derive the final results and heterogeneity for each of the two subgroups. The differences in the results between the two subgroups were observed, and if the differences were statistically different, they indicated that the potential factor was the main influencing element affecting this meta-analysis. Concurrently, based on an observation of the magnitude of heterogeneity among subgroups, if the heterogeneity of one or both of the subgroups disappeared, it further indicated that the potential factor was the main source of heterogeneity.
We also plotted funnel plots to clearly and accurately reflect the presence of bias in this meta-analysis.
Results
Study inclusion
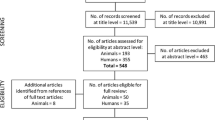
A total of 510 articles were found from the search and after removing duplicates (N = 99), 411 articles were screened based on the title and abstract, and 383 articles were excluded based on the exclusion criteria. A total of seven articles were selected for further screening, and their complete manuscripts were reviewed, of which two articles were excluded because one of them could not be found in usable full text and the other [25] contained confounding factors (aspirin) in addition to NO, resulting in the inclusion of five studies in the systematic review. We also referred to the references of these five articles and found two more that met the eligibility criteria for the review, which totaled up to seven articles [26,27,28,29,30,31,32], of which four articles included two independent clinical studies, thereby increasing the final number of included studies in the meta-analysis to 11. The flowchart of the study selection process is shown in Fig. 1.

Flowchart of the study selection process in the meta-analysis
Characteristics of the included studies
The seven studies were published in the last 15 years (2007–2022) and included a total of 149 participants. Six of the studies involved healthy populations and one [25] involved early menopausal women. The number of participants included in each study ranged from 9 to 34. Of the sources of NO, four were from GTN, two from pentaerithrityl tetranitrate (PETN), two from beetroot, and one from nitrite. The choice of placebo for the control group was conducted on a case-by-case basis and included saline, beetroot juice without NO3−, and no special treatment. Routes of administration included intravenous, oral, and transdermal, with a dosing duration ranging from 20 min to 7 days. The GTN dose was 0.6 mg/h for 2 h/day in all four trials. The PTNE dose was 80 mg/day. Only one study [28] was administered after the onset of ischemia; the remaining studies were administered before I/R. No adverse effects were reported in any of the studies. The quality of the studies indicated an overall low risk of bias. However, only two reported information on random sequence generation and allocation concealment, and the remaining two reported unknown risks. In five of the trials, the researchers were blinded. The risk of bias assessment graph is shown in Fig. 2. The specific detailed characteristics of each study are shown in Table 1.

Risk of bias assessment for each included study
Results of meta-analysis
The results of our meta-analysis showed that in 11 experiments, consisting of a total of 149 participants, NO donors had a protective effect on endothelial function in I/R injury (SMD: -1.60; 95% CI: − 2.33, − 0.88, P < 0.0001). However, there was significant heterogeneity in the results (I2 = 66%, P = 0. 001) (See Fig. 3 for specific results). The results of the case-by-case sensitivity analysis have low sensitivity.

Forest plot of the effect of NO donor intervention on endothelial function in I/R injury
We divided the different subgroups according to the timing of NO donor administration and the duration of NO donor administration, and the results are as follows: (1) Using the duration of NO donor administration as a cutoff, the results of the subgroup analysis were − 0.89 (95% CI: − 2.06, 0.28) for the long-term group and − 1.92 (95% CI: − 2.79, − 1.05) for the short-term group, with no statistically significant difference between the two groups (P = 0. 17) (See Fig. 4a for specific results).(2) Using the timing of NO donor administration as a cutoff, the results of the meta-analysis were − 1.78 (95% CI: − 2.50, − 1.07) for the pre-ischemic subgroup and − 1.78 (95% CI: − 2.50, − 1.07) for the post-ischemic subgroup, with statistically significantly different results between the two subgroups (P = 0.007) (See Fig. 4b for specific results).

Forest plots for subgroup analysis according to duration of NO donor use (a) and timing of NO donor use (b). Short-term: short-term use (< 24 h) of NO donor; long-term: long-term (> 24 h) use of NO donor. Pre-I/R: pre-ischemic use of NO donor; post-I/R: post-ischemic use of NO donor
Publication bias results
The funnel plots were symmetrical, indicating no significant publication bias in the results obtained from the 11 studies. The funnel plots are shown in Fig. 5.

Funnel plot of NO donor effects on endothelial function in I/R injury
Discussion
This is the first meta-analysis of the protective effect of NO donors on endothelial function in I/R, and overall, the present study indicates that NO donors have a protective effect on the endothelium in IR injury. However, the timing as well as the duration of NO donor use can affect the final outcome.
The results of the subgroup analysis in this study support the short-time use of NO donors before the onset of ischemia to prevent endothelial dysfunction due to I/R injury. However, all subgroups show significant heterogeneity, so this heterogeneity is likely to be real and may be due to differences in the population, Intervention drugs and Intervention drug dosage included in this study. NO2− entering the tissues can be used during hypoxia, or it can be converted to metabolites and stored in the tissues; its effects can be transmitted from the vascular surface to the tissues, thus preventing subsequent injury [33]. Most animal models suggest a beneficial effect on I/R injury when NaNO2 is injected prior to ischemia [34]. Under hypoxic conditions, hypoxic signaling reduces eNOS expression and activity. Meanwhile, by interfering with BH4 and L-Arg/ADMA-related activity or expression, it causes eNOS uncoupling, and uncoupled eNOS is an important source of free radicals that can disrupt redox homeostasis and cause oxidative stress. Simultaneously, hypoxia impairs the NO pathway by stimulating endothelial activation to increase oxygen radical production from the mitochondrial respiratory chain and NADPH (Nicotinamide Adenine Dinucleotide Phosphate) oxidase. Relying on exogenous NO supplementation alone at this point does not increase NO bioavailability but may instead increase peroxynitrite production and thus cause further endothelial dysfunction. Prolonged use of NO donors leads to loss of protective effect on endothelial function. This may be due to the development of tolerance after prolonged use of NO donors. After repeated administration, oxidative modifications in ALDH-2 may lead to loss of function of the enzyme, resulting in reduced GTN biotransformation and inhibition of the final effects of pharmacological pretreatment [35, 36]. However, not all nitrates are tolerated, and there is experimental evidence that long-term continuous application of PETN [37] does not lead to the development of tolerance, in part due to the ability of PETN to induce HO-1.
NO is extremely unstable in the body and is usually stored in the body in the form of nitrate or nitrite. In the past, nitrate or nitrite was often considered as inert products of NO oxidative metabolism. However, discoveries in recent years have shown that nitrite can act as a source of NO in vivo, especially under hypoxic conditions. Studies using bactericides to kill the oral microbiome or systemic NOS inhibition have shown that about half of the basal plasma nitrite comes from the reduction of nitrate in saliva and the other half from the oxidation of NO produced primarily by eNOS [38]. Nitrate ingested through the diet is reduced to nitrite by oral flora [39], which forms a pool of nitrite, along with nitrite from the oxidation of NO produced by NOS in the body. The reduction of nitrite to NO in the vascular system can be mediated by a variety of proteins, including heme proteins (heme proteins) [40, 41], XO, carbonic anhydrase [42], heme P450 cytochromes [43], etc. The primary mechanism for the hemodynamic effects of nitrate is thought to be attributed to the activation of the intracellular NO receptor enzyme soluble guanylate cyclase, leading to increased bioavailability of cGMP and activation of cGMP-dependent protein kinase and/or cyclic nucleotidylated ion channels [44]. In addition, S-nitrosylation of key intracellular proteins may reduce mitochondrial L-type Ca2+ channel function [45] and inhibit complex I of the electron transport chain, which generates ROS during reperfusion [46, 47]. Together, these theories suggest that the use of NO donor drugs is an effective alternative therapy for “NO-deficient” diseases.
However, there are several limitations to this meta-analysis. Firstly, the number of included studies and the total number of participants were relatively small. There were few high-quality studies on the effects of NO donor agent administration on endothelial function in patients with I/R injury. However, the use of NO donor agents in patients with I/R injury did not result in adverse events, such as hypotension or methemoglobinemia. Our results are important for clinical scientists who wish to further investigate ways to mitigate endothelial dysfunction in I/R injury. Secondly, the NO agents used in the included trials varied in doses and types and had different clinical protocols, leading to a high degree of heterogeneity. Meta-analyses are based on retrospective analytical extrapolation and may be influenced by a variety of factors, such as the inclusiveness of the search strategy for determining eligible studies, assumptions about the consistency of the methods applied across studies, and limited accessibility to data from individual studies. However, our clear delineation of inclusion and exclusion criteria and comprehensive searches of the four major electronic databases and reference lists were likely to minimize bias and increase the representativeness of the results.
Conclusion
Normal endothelial cell function plays a key role in maintaining vascular homeostasis. Previous studies have confirmed that nitrates improve endothelial function in patients without IR; however, there has been no systematic evaluation of whether NO supplementation improves endothelial function in patients with IR. In the present study, we found that pre-ischemic, short-term application of NO donors protected endothelial function in patients with IR. For endothelial dysfunction in human subjects with I/R injury, administration of NO donor agents may be an effective treatment.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NO:
-
Nitric oxide
- CI:
-
Confidence interval
- I/R:
-
Ischemia/reperfusion
- ROS:
-
Reactive oxygen species
- eNOS:
-
Endothelial nitric oxide synthase
- GTN:
-
Nitroglycerin
- FMD:
-
Flow-mediated dilation
- NADPH:
-
Nicotinamide Adenine Dinucleotide Phosphate
- PRISMA:
-
Preferred Reporting Items for Systematic Review and Meta-Analysis
- RCTs:
-
Randomized controlled trials
- SMD:
-
Standardized mean difference
References
Andreadou I, Iliodromitis EK, Farmakis D, Kremastinos DT. To prevent, protect and save the ischemic heart: antioxidants revisited. Expert Opin Ther Targets. 2009;13:945–56.
Carden DL, Granger DN. Pathophysiology of ischaemia-reperfusion injury. J Pathol. 2000;190:255–66.
Janaszak-Jasiecka A, Siekierzycka A, Płoska A, Dobrucki IT, Kalinowski L. Endothelial dysfunction driven by hypoxia-the influence of oxygen deficiency on NO bioavailability. Biomolecules. 2021;11:982.
Boyle EM, Pohlman TH, Cornejo CJ, Verrier ED. Endothelial cell injury in cardiovascular surgery: ischemia-reperfusion. Ann Thorac Surg. 1996;62:1868–75.
Palmer RM, Ferrige AG, Moncada S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature. 1987;327:524–6.
Farah C, Michel LYM, Balligand J-L. Nitric oxide signalling in cardiovascular health and disease. Nat Rev Cardiol. 2018;15:292–316.
Stuehr DJ. Enzymes of the L-arginine to nitric oxide pathway. J Nutr. 2004;134(10 Suppl):2748S–51S. discussion 2765S-2767S
Tejero J, Shiva S, Gladwin MT. Sources of vascular nitric oxide and reactive oxygen species and their regulation. Physiol Rev. 2019;99:311–79.
Cosby K, Partovi KS, Crawford JH, Patel RP, Reiter CD, Martyr S, et al. Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circulation. Nat Med. 2003;9:1498–505.
Shiva S, Huang Z, Grubina R, Sun J, Ringwood LA, MacArthur PH, et al. Deoxymyoglobin is a nitrite reductase that generates nitric oxide and regulates mitochondrial respiration. Circ Res. 2007;100:654–61.
Sparacino-Watkins CE, Tejero J, Sun B, Gauthier MC, Thomas J, Ragireddy V, et al. Nitrite reductase and nitric-oxide synthase activity of the mitochondrial molybdopterin enzymes mARC1 and mARC2. J Biol Chem. 2014;289:10345–58.
Li H, Samouilov A, Liu X, Zweier JL. Characterization of the magnitude and kinetics of xanthine oxidase-catalyzed nitrite reduction. Evaluation of its role in nitric oxide generation in anoxic tissues. J Biol Chem. 2001;276:24482–9.
Shiva S, Sack MN, Greer JJ, Duranski M, Ringwood LA, Burwell L, et al. Nitrite augments tolerance to ischemia/reperfusion injury via the modulation of mitochondrial electron transfer. J Exp Med. 2007;204:2089–102.
Baker JE, Su J, Fu X, Hsu A, Gross GJ, Tweddell JS, et al. Nitrite confers protection against myocardial infarction: role of xanthine oxidoreductase, NADPH oxidase and K(ATP) channels. J Mol Cell Cardiol. 2007;43:437–44.
Souza JM, Peluffo G, Radi R. Protein tyrosine nitration--functional alteration or just a biomarker? Free Radic Biol Med. 2008;45:357–66.
Pacher P, Beckman JS, Liaudet L. Nitric oxide and peroxynitrite in health and disease. Physiol Rev. 2007;87:315–424.
Azevedo ER, Schofield AM, Kelly S, Parker JD. Nitroglycerin withdrawal increases endothelium-dependent vasomotor response to acetylcholine. J Am Coll Cardiol. 2001;37:505–9.
Gori T, Mak SS, Kelly S, Parker JD. Evidence supporting abnormalities in nitric oxide synthase function induced by nitroglycerin in humans. J Am Coll Cardiol. 2001;38:1096–101.
Anderson EA, Mark AL. Flow-mediated and reflex changes in large peripheral artery tone in humans. Circulation. 1989;79:93–100.
Song L, Xu M-B, Zhou X-L, Zhang D-P, Zhang S-L, Zheng G-Q. A preclinical systematic review of Ginsenoside-Rg1 in experimental Parkinson’s disease. Oxidative Med Cell Longev. 2017;2017:2163053.
Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol. 1992;45:769–73.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Gresele P, Migliacci R, Procacci A, De Monte P, Bonizzoni E. Prevention by NCX 4016, a nitric oxide-donating aspirin, but not by aspirin, of the acute endothelial dysfunction induced by exercise in patients with intermittent claudication. Thromb Haemost. 2007;97:444–50.
Dragoni S, Gori T, Lisi M, Di Stolfo G, Pautz A, Kleinert H, et al. Pentaerythrityl tetranitrate and nitroglycerin, but not isosorbide mononitrate, prevent endothelial dysfunction induced by ischemia and reperfusion. Arterioscler Thromb Vasc Biol. 2007;27:1955–9.
Gori T, Di Stolfo G, Sicuro S, Dragoni S, Lisi M, Forconi S, et al. Nitroglycerin protects the endothelium from ischaemia and reperfusion: human mechanistic insight. Br J Clin Pharmacol. 2007;64:145–50.
Ingram TE, Fraser AG, Bleasdale RA, Ellins EA, Margulescu AD, Halcox JP, et al. Low-dose sodium nitrite attenuates myocardial ischemia and vascular ischemia-reperfusion injury in human models. J Am Coll Cardiol. 2013;61:2534–41.
McLaughlin K, Lytvyn Y, Luca MC, Liuni A, Gori T, Parker JD. Repeated daily dosing with sildenafil provides sustained protection from endothelial dysfunction caused by ischemia and reperfusion: a human in vivo study. Am J Physiol-Heart Circ Physiol. 2014;307:H888–94.
Somani YB, Soares RN, Gosalia J, Delgado JM, Flanagan M, Basu S, et al. A single dose of dietary nitrate supplementation protects against endothelial ischemia-reperfusion injury in early women. Appl Physiol Nutr Metab. 2022. https://doi.org/10.1139/apnm-2021-0693.
Webb AJ, Patel N, Loukogeorgakis S, Okorie M, Aboud Z, Misra S, et al. Acute blood pressure lowering, vasoprotective, and antiplatelet properties of dietary nitrate via bioconversion to nitrite. Hypertension. 2008;51:784–90.
Lisi M, Oelze M, Dragoni S, Liuni A, Steven S, Luca M-C, et al. Chronic protection against ischemia and reperfusion-induced endothelial dysfunction during therapy with different organic nitrates. Clin Res Cardiol Off J Ger Card Soc. 2012;101:453–9.
Liu T, Schroeder H, Power GG, Blood AB. A physiologically relevant role for NO stored in vascular smooth muscle cells: a novel theory of vascular NO signaling. Redox Biol. 2022;53:102327.
Webb A, Bond R, McLean P, Uppal R, Benjamin N, Ahluwalia A. Reduction of nitrite to nitric oxide during ischemia protects against myocardial ischemia-reperfusion damage. Proc Natl Acad Sci U S A. 2004;101:13683–8.
Szöcs K, Lassègue B, Wenzel P, Wendt M, Daiber A, Oelze M, et al. Increased superoxide production in nitrate tolerance is associated with NAD(P)H oxidase and aldehyde dehydrogenase 2 downregulation. J Mol Cell Cardiol. 2007;42:1111–8.
Marini E, Giorgis M, Leporati M, Rolando B, Chegaev K, Lazzarato L, et al. Multitarget antioxidant NO-donor organic nitrates: a novel approach to overcome nitrates tolerance, an ex vivo study. Antioxid Basel Switz. 2022;11:166.
Daiber A, Oelze M, Wenzel P, Bollmann F, Pautz A, Kleinert H. Heme oxygenase-1 induction and organic nitrate therapy: beneficial effects on endothelial dysfunction, nitrate tolerance, and vascular oxidative stress. Int J Hypertens. 2012;2012:842632.
Kapil V, Haydar SMA, Pearl V, Lundberg JO, Weitzberg E, Ahluwalia A. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radic Biol Med. 2013;55:93–100.
Qin L, Liu X, Sun Q, Fan Z, Xia D, Ding G, et al. Sialin (SLC17A5) functions as a nitrate transporter in the plasma membrane. Proc Natl Acad Sci U S A. 2012;109:13434–9.
Liu C, Wajih N, Liu X, Basu S, Janes J, Marvel M, et al. Mechanisms of human erythrocytic bioactivation of nitrite. J Biol Chem. 2015;290:1281–94.
Gladwin MT, Kim-Shapiro DB. The functional nitrite reductase activity of the heme-globins. Blood. 2008;112:2636–47.
Aamand R, Dalsgaard T, Jensen FB, Simonsen U, Roepstorff A, Fago A. Generation of nitric oxide from nitrite by carbonic anhydrase: a possible link between metabolic activity and vasodilation. Am J Physiol Heart Circ Physiol. 2009;297:H2068–74.
Li H, Liu X, Cui H, Chen Y-R, Cardounel AJ, Zweier JL. Characterization of the mechanism of cytochrome P450 reductase-cytochrome P450-mediated nitric oxide and nitrosothiol generation from organic nitrates. J Biol Chem. 2006;281:12546–54.
Birschmann I, Walter U. Physiology and pathophysiology of vascular signaling controlled by guanosine 3′,5′-cyclic monophosphate-dependent protein kinase. Acta Biochim Pol. 2004;51:397–404.
Sun J, Morgan M, Shen R-F, Steenbergen C, Murphy E. Preconditioning results in S-nitrosylation of proteins involved in regulation of mitochondrial energetics and calcium transport. Circ Res. 2007;101:1155–63.
Burwell LS, Nadtochiy SM, Brookes PS. Cardioprotection by metabolic shut-down and gradual wake-up. J Mol Cell Cardiol. 2009;46:804–10.
Zhang D, Wang F, Li P, Gao Y. Mitochondrial Ca2+ homeostasis: emerging roles and clinical significance in cardiac remodeling. Int J Mol Sci. 2022;23:3025.
Acknowledgements
Not applicable.
Funding
This work was supported by National Natural Science Foundation of China (grant No. 81974081,81601724), Guangdong Basic and Applied Basic Research Foundation (grant No. 2021A1515012318, 2019A1515011852), Science and Technology Program of Guangzhou, China (grant No. 202201010765, 202102010190).
Author information
Authors and Affiliations
Contributions
Study design: CD; data acquisition: CD and HX; data analysis/interpretation: XZ, XX and ZH; Supervision or mentorship: XH and GL. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved. WY, XZ and HL take responsibility that this study has been reported honestly, accurately, and transparently. All authors approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Material.
Search strategy for Medline.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dou, C., Han, X., Xie, H. et al. Protective role of nitric oxide donors on endothelium in ischemia-reperfusion injury: a meta-analysis of randomized controlled trials. BMC Anesthesiol 23, 189 (2023). https://doi.org/10.1186/s12871-023-02117-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02117-w