
Abstract
The health of a population is an important indicator of the general well-being of the population, and it has its practical significance, as it determines the costs of providing care, and social and medical assistance for the elderly. The study presents an assessment of healthy life-expectancy indicators of people over age 65 based on the results of the Russian epidemiological study EVCALIPT and a comparison of this results with data from other surveys in Russia and European countries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Life expectancy, LE (at birth or at any other age) is an integral characteristic of the mortality rate of the population. At the same time, as life expectancy increases and the population ages, additional indicators are needed that reflect not only changes in mortality in certain age groups, but also the health status of the population, mainly the elderly [29]. The state of health of the population is an important indicator not only of its general well-being, but is also of practical importance, as it determines the costs of caring for the elderly, and social and medical assistance.
The indicator of healthy life expectancy (HLE) is provided for in Decree of the President of the Russian Federation No. 204 dated May 7, 2018 “On the national goals and strategic objectives of the development of the Russian Federation for the period up to 2024” (increasing the HLE to 67 years). According to an approved methodology, this indicator is assessed using information on the self-rated health of the population according to selective federal statistical observation of the state of health of the population conducted by Rosstat.Footnote 1 According to published estimates by Rosstat, the HLE at birth was 60.3 years in 2019 and 58.9 years in 2020.
Self-rated health in general is widely used to calculate the integral indicators of health at the population level, such as HLE or years of life lost. A number of studies show a significant association between poor self-rated health and a higher risk of death in different countries [23, 34]. Self-rated health correlates well with morbidity and mortality within population groups, but this correlation is not always observed at the population level between the populations of different countries and regions [11].
In Russia, for the analysis of the state of public health, data from the Russian Monitoring of the Economic Situation and Health of the Population of the Higher School of Economics (RMEH), as well as the study “Parents and Children, Men and Women in the Family and Society” (P&CM&W) are widely used [3, 8, 10, 19, 35]. Thus, it was shown that in terms of HLE, Russia is inferior to European countries, mainly due to the high mortality of men of working age and poor health, according to the self-rated health of older women [1, 3, 8]. At the age of over 65 years, HLE indicators calculated according to the RLMS self-assessment of health are higher for men than for women due to lower self-rated health in older women, despite a higher life expectancy of women compared to men in general [3, 4].
Thus, self-reported health is the most common indicator of the health status of the population, often supplementing life expectancy. At the same time, the assessment of health status at an older age requires the involvement of more objective and meaningful indicators, including taking into account limitations in daily activity and the need for assistance with self-care. As mentioned above, data on the self-reported health of the population in Russia are presented in several surveys of the population (RMEH, P&CM&W, sample survey of Rosstat); however, a comprehensive assessment of the health status, especially of the elderly population, requires specialized surveys aimed, among other things, at obtaining objective indicators of health status and functional status. To obtain such information in Russia, a large epidemiological study EVCALIPT (Epidemiological study of the prevalence of geriatric syndromes and age-associated diseases in the elderly in regions of the Russian Federation with different climatic, economic and demographic characteristics), which collected information on the prevalence of geriatric syndromes and carried out assessment of the health status of people over 65 years based on the results of a comprehensive geriatric assessment was conducted [2]. This study was organized in 2018 at the initiative of the Russian Association of Gerontologists and Geriatrics and the Russian Gerontological Research and Clinical Center in cooperation with the National Research University Higher School of Economics. The aim of the study was to obtain domestic data on the prevalence of age-associated and chronic non-communicable diseases, senile asthenia and other geriatric syndromes in people over age 65, as well as to analyze the contribution of these diseases and syndromes to indicators of general health and functional status. The study has limitations, which lie in the fact that the features of sample formation do not allow us to consider it representative of the population of Russia. A more detailed description of the study is given in the relevant publications [2].
The functional status of the elderly may decrease due to physiological changes during life, as a result of which they become limited in basic and instrumental activity. Basic daily activities are self-care activities that include personal hygiene, eating, etc. Instrumental daily activities are more complex activities that require a higher level of autonomy and cognitive function and are necessary for independent living (using transportation, cooking, laundry, etc.). The need for help or difficulty in performing certain daily activities is considered as the presence of limitations in basic or instrumental activity [17]. The use of information on the prevalence of limitations in daily activities to calculate life expectancy without limitations provides important information about the health of the population, which can be used in planning in the healthcare system and social assistance and in the development of appropriate social and demographic policies [25, 28].
The purpose of this study is to assess the life expectancy of people aged 65 years or over and compare the results obtained with data from sample surveys of the population in Russia and European countries, as well as assess the conformity of the results obtained according to EVCALIPT data to the characteristics of self-assessment of the health of the general population (population of Russia) according to RMEH. The paper compares the self-assessment life expectancy of people over age 65 according to the EVCALIPT study, the population of Russia according to the RMEH data, and also compares it with European countries according to the ESS and SHARE surveys. Additionally, according to EVCALIPT and SHARE data, the life expectancy is calculated taking into account the functional status of the respondents (the presence of limitations on basic and instrumental activity).
MATERIALS AND METHODS
The source of data on the self-assessment of health and the presence of limitations in basic and instrumental activity are data from several surveys of the population in Russia and European countries. For comparison with EVCALIPT data on the self-assessment of health, we used the data of the Russian Monitoring of the Economic Situation and Health of the Population of the National Research University “Higher School of Economics” (RMEH) of the 27th wave (the surveys were conducted in 2018). The total sample size of the RMEH [5] of the 27th wave in the Russian Federation at the age of 65 years and older was 2283 people and that of the EVCALIPT sample, 4308 people, of which data on the self-assessment of health are indicated for 3963 people. Data on self-reported health in European countries are presented based on the results of the 9th wave of The European Social Survey [20] and the 7th wave of the Survey of Health, Aging and Retirement in EuropeFootnote 2 (SHARE) [13–15]. We also used SHARE data on the presence of limitations in basic and instrumental activity. The list of countries based on the data of these surveys and the sample size are presented in Table 1.
The EVCALIPT study used a visual analog scale [6] for self-assessment of health status, ranging from 0 (very poor) to 10 (very good).
Basic daily activity (Bartel index) was assessed according to the standard method [6]. The subjects were asked 10 questions regarding the ability to independently eat, take care of themselves at home, dress, go to the toilet, take a bath, control urination and defecation, climb stairs, move around the house and outside it. For each answer to the question, points were awarded (0 is needs help/completely dependent on outside help; 5, 10 or 15 points, depending on the question: does not need or partially needs help), the scores were totaled.
Instrumental daily activity was assessed using the Lawton scale [6]. The questionnaire includes eight questions related to the ability to independently use the phone, take medicine, manage finances, cook food, go to the grocery store, do housework, wash clothes, and get to places located outside the usual walking distances. For each answer to the question, 0 or 1 point was awarded (0 is cannot; 1 is can independently or with outside help), the points obtained were summed up.
The analysis was carried out using binary variables for the self-assessment of health and the presence of limitations on basic and instrumental daily activities. The wording of the questions and the scale for assessing health and the presence of limitations differ between the surveys used (Table 2). It should be noted that differences in the wording of the questions may affect the comparability of the results obtained on the prevalence of poor health [16].
The comparison of EVCALIPT data and SHARE data for European countries in terms of the proportion of people without limitations on basic and instrumental activity is given taking into account at least one limitation; however, the calculation of life expectancy without limitations according to EVCALIPT data is based on the presence of a pronounced dependence, the criteria for which are also given in Table 2. Data on self-reported health and other characteristics of the respondents, disaggregated by sex and age, were used to calculate the age-specific rates of poor health and limitations on basic and instrumental activity.
To calculate the mortality tables for Russia, we used the data of the Federal State Statistics Service (Rosstat) on the distribution of the dead and the population by sex and age groups for 2018 (in accordance with the year of the main part of the EVCALIPT surveys). For international comparisons, we also used data on the number of deaths and population for a number of European countries with reliable mortality statistics from the Human Mortality Database (HMD), which is the most authoritative source of mortality data [12, 22], for 2017—2018 or the latest available year for the respective countries.
The estimate of the HLE/unlimited life expectancy was made according to the Sullivan method [36] using summary tables of mortality for Russia and countries of Eastern and Western Europe. The Sullivan method consists in dividing the population of those living in each age interval into those with poor and good health, then, taking into account the proportion of people with good health, the indicators of the mortality tables (for the relevant generation) for the population with good health are calculated. HLE is the average number of years that a person is expected to live in a healthy state, assuming that throughout their life (at an age older than the age for which the indicator is calculated) the same age-specific mortality rates and proportion of the population with poor health as in the year for which the indicator is calculated, is preserved. Thus, HLE takes into account both the mortality rate and the state of health.
RESULTS AND DISCUSSION
Figure 1 shows the proportion of respondents with poor health according to self-assessment by sex and age reported by RMEH and EVCALIPT, indicating the 95% confidence interval. First of all, it should be noted that there are a higher proportion of respondents with poor health aged 65–69 years for men and 65–79 years for women according to the EVCALIPT survey. The proportion of men with poor health according to EVCALIPT increases with age from 33.7% at the age of 65–69 years to 82.4% over age 95; according to the RMEH, this increases from 19.5% at the age of 65–69 years to 75% over the age 90; and for women, from 38.8 to 76%, respectively, according to EVCALIPT and from 28.4 to 74%, according to RMEH. Estimates based on the EVCALIPT data change more steadily with age, and in older age groups, due to the larger sample size, they are characterized by a smaller confidence interval compared to the RMEH data.

Share of respondents with poor health according to self-assessment in Russia (according to RMEH and EVCALIPT).
Self-reported health in Eastern European countries and Russia deteriorates with age at a faster rate than in Western European countries. At the age of 65–69, the indicators in European countries, as well as in Russian men, according to the RMEH data, are comparable with each other; with age, the gap in the proportion of respondents with poor health between Russia and European countries increases (Fig. 2).

Share of respondents with poor health according to self-assessment in Russia and European countries.
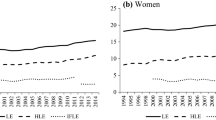
According to the EVCALIPT data, the HLE for men at the age of 65 was 8.1, which is 0.6 years lower compared to the estimate according to the RMEH data (Fig. 3); for women it was 9.2 years (according to the RMEH data it was 10 years).

Life expectancy (LE) and healthy life expectancy (HLE) in Russia (according to EVCALIPT and RMEH).
Depending on the data source, the difference in the HLE at age 65 between Russia and Eastern Europe is 3.2–4 years for men and 3.6–4.8 years for women. In Western Europe, men at the age of 65 are expected to live in good health 7.4–8.5 years more than in Russia, and women, for 8.6–9.6 years. At the same time, the difference in the life expectancy in general at the age of 65 between Russia and the countries of Western Europe is significantly lower and amounts to 5.2 years for men and 4.7 years for women (Table 3).
Russia is ahead of European countries in terms of the difference in life expectancy between men and women; however, the difference in life expectancy between the sexes in Russia, on the contrary, is minimal, and amounts to 1.1 years according to EVCALIPT data and 1.3 years according to RMEH data (in Eastern Europe, it is 1.7–2 years and in the countries of Western Europe, 2.1–2.4 years).
Thus, the EVCALIPT data show a larger proportion of people with poor health according to self-assessment in younger age groups compared to the RMEH data, and lower, but comparable estimates with HLE.
The proportion of respondents without limitations on instrumental activity (taking into account the presence of at least one limitation) according to the EVCALIPT survey is lower than in European countries. For women, the indicators in the countries of Western and Eastern Europe and in Russia, according to the EVCALIPT data, appeared to be closer; at the same time, the tendency for the countries of Eastern Europe to lag behind the countries of Western Europe and Russia from the countries of Western and Eastern Europe remains (Fig. 4).

Percentage of respondents without limitations on instrumental activity in Russia and European countries.
According to the EVCALIPT survey, the proportion of women aged 65–69 years without limitations on instrumental activity is 75.8%, and over 90 it decreases to 10.2% (in Western Europe, it is from 87.6 to 20.1%, and in the countries of Eastern Europe, it is from 83.2 to 16.7%, respectively).
The proportion of men without limitations on instrumental activity according to the EVCALIPT survey is significantly lower than in European countries, according to SHARE, and also significantly lower than in women. As shown in Table 4, the differences in the proportion of persons without instrumental-activity limitations between men and women according to EVCALIPT data are primarily due to such activities as cooking and washing, however, the exclusion of these types of activity from the calculation of indicators for men has little effect on the presented results.
The proportion of respondents without limitations on basic activity according to the EVCALIPT survey is also lower than in European countries. The difference between the countries of Eastern and Western Europe is relatively small (Fig. 5), while for men, the difference in indicators between the EVCALIPT sample and European countries according to SHARE data increases rapidly with age, and for women, a noticeable delay is observed from the age of 65. Thus, according to the EVCALIPT data, the proportion of men aged 65–69 years without limitations on basic activity is 86.3%, by the age of 85–89 years it decreases to 50.3%, and over 90 years, it increases to 24.2% (in the countries of Western Europe, it is from 92.1 to 58.3%, and in Eastern Europe, it is from 89.6 to 49.4%, respectively). The difference in the proportion of people without limitations on basic activity according to EVCALIPT and SHARE data in women in the considered age range is 10–20%.

Share of respondents without limitations on basic activity in Russia and European countries.
A subjective deterioration in health occurs on average earlier than the need for additional assistance in daily activities and self-care. Thus, according to self-assessment, life expectancy with poor health is about 9 years for women and 5.8 years for men. Without limitations in instrumental activity (taking into account the presence of pronounced limitations), at the age of 65, the women surveyed are expected to live an average of 14.2 years and men 12.3 years; without limitations on basic activity, they are expected to live 17.2 and 13 years, respectively (Table 5).
Life expectancy with limitations on basic and instrumental activities gives an idea of how much of the life older people, on average, need extra care or assistance in daily life. The preliminary results of calculations based on the EVCALIPT study show that older people aged 65 years and older, on average, live with severe limitations in basic daily activities (eating, personal hygiene, and so on), and therefore need appropriate care, for 0.9 years (see Table 5). For about 4 years of life in women and 1.5 years in men aged 65 and older, there are limitations in instrumental activity (going to the store, cooking, housekeeping, etc.).
Almost half of the life expectancy of women occurs in a period with poor health according to self-rated health (for men, it is 42%), including with limitations on instrumental activity, 22% for women and 11% for men and with limitations on basic activity, 5 and 6.5% respectively.
CONCLUSIONS
Self-reported health is one of the most sensitive indicators predicting the risk of death at the individual level. The strong relationship between self-reported health and mortality is evidenced by the results of studies in other countries. At the same time, self-reported health in surveys of the Russian population is on average worse than in English-speaking countries, which may indicate objective factors, such as high levels of morbidity and disability, which is also reflected in high mortality in Russia compared to other countries. However, differences in self-reported health do not always explain differences in mortality rates and may be due, among other things, to subjective factors. In addition, the use of indicators based on self-reported health does not allow the identification and assessment of the population’s need for services for care of the elderly. The planning and development of measures in the health-and-social-care system also require the involvement of objective indicators of health and functional status.
One approach to using functional-status data is to calculate the “active” life expectancy, which is the expected number of years of life without limitations on daily activity [24, 26, 28, 29], which is used, among other things, to estimate healthcare costs associated with a change in functional status [21, 30]. Studies conducted in a number of foreign countries show a trend towards a gradual decrease in the prevalence of functional-activity limitations over time [9, 17, 18, 29, 37].
The results of the EVCALIPT survey reflect patterns known for Russia in the prevalence of self-reported poor health, but show a larger proportion of people with self-reported poor health in younger age groups and, accordingly, lower, but generally comparable estimates of healthy life expectancy compared to nationally representative RMEH data.
It is necessary to note a number of limitations of the presented results according to the EVCALIPT data. Thus, the presented sample is not representative of the population of Russia, since it is based on data on patients of medical organizations in several regions of Russia. In this regard, it is necessary to refer to the obtained results with caution. In particular, the higher proportion of people with poor health in younger age groups (compared to the RMEH data) may be the result of a larger representation of people with health problems in the sample.
According to the EVCALIPT survey, interviewed patients aged 65 years and older, on average for about 1 year of life, need care associated with limitations in basic activity (eating, personal hygiene). With limitations in instrumental activity that do not require constant care, women are expected to live for 4 years and men for 1.7 years. Studies of the healthy life expectancy without limitations show the advantage of women over men in life expectancy in general, with a higher proportion of life expectancy with functional-status limitations [7, 17, 27, 28, 31–33], the so-called “male-female health-survival paradox”. Estimates of healthy life expectancy according to the EVCALIPT data also show that the proportion of life expectancy with health limitations in women is higher than in men both in terms of self-reported health and the presence of instrumental-activity limitations.
The need to develop an adapted methodology for assessing the presence of limitations in instrumental activity for men in Russia should also be noted. The results of the Lawton score used in the EVCALIPT study are likely to overestimate the proportion of men with limited activity compared to women, and also compared to European countries with a comparable proportion of people with limited basic activity.
The results obtained can be used within the framework of gerontological service to assess the characteristics of patients in gerontological clinics, including resource planning for the provision of medical and social assistance to the elderly.
Notes
Rosstat Order No. 95 of February 25, 2019 “On approval of the methodology for calculating the indicator “Healthy life expectancy” (years).”
The collection of data for SHARE was financed by the European Commission within the framework of FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RIICT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA no. 211 909, SHARELEAP: GA no. 227822, SHARE M4: GA no. 261 982, DASISH: GA no. 283 646) and Horizon 2020 (SHARE-DEV3: GA no. 676 536, SHARECOHESION: GA no. 870 628, SERISS: GA no. 654 221, SSHOC: GA no. 823782) and the European Commission Directorate-General for Employment, Social Affairs, and Inclusion. Additional financing was obtained from the Federal Ministry of Education and Research of Germany, the Max Planck Society for the Advancement of Science, and the National Institute on Aging of the USA (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and various national sources of financing.
REFERENCES
Andreev, E.M., Shkol’nikov, V.M., and McKee, M., Healthy life expectancy, Vopr. statistiki, 2002, no. 11, pp. 16–21.
Vorob’eva, N.M., Tkacheva, O.N., Kotovskaya, Yu.V., et al., Russian epidemiologic survey EVKALIPT: protocol and basal characteristics of participants, Ros. Zh. Geriatr. Med., 2021, no. 1, pp. 35–43. https://doi.org/10.37586/2686-8636-1-2021-35-43
Ramonov, A.V., Healthy life expectancy as an integral estimate of health of the Russians, Ekon. Zh. Vysshei Shkoly Ekonomiki, 2011, vol. 15, no. 4, pp. 497–518.
Ramonov, A.V., Analysis of health status of the Russian population using integral indoces, Sots. Issledovaniya, 2012, vol. 335, no. 3, pp. 104–116.
Rossiiskii monitoring ekonomicheskogo polozheniya i zdorovya naseleniya NIU VShE (RLMSHSE), provodimyi Natsional’nym issledovatel’skim universitetom Vysshey shkoly ekonomiki i OOO “Demoskop” pri uchastii Tsentra narodonaseleniya Universiteta Severnoy Karoliny v Chapel Khille i Instituta sotsiologii Federal’nogo gosudarstvennogo byudzhetnogo uchrezhdeniya nauki Federal’nogo nauchno-issledovatel’skogo sotsiologicheskogo tsentra RAN (Russian Monitoring of Economic State and Health of Population by the National Research University of the Higher School of Economics (RLMSHSE) Performed by the National Research University of the Higher School of Economics and Demoscope Ltd. with the involvement of the Carolina Population Center of the University of North Carolina in Chapel Hill and the Institute of Sociology of the Federal Budgetary Scientific Institution, Federal Research Sociological Center of the Russian Academy of Sciences) (RLMS-HSE survey sites: http://www.hse. ru/rlms, http://www.cpc.unc.edu/projects/rlms).
Tkacheva, O.N., Kotovskaya, Yu.V., Runikhina, N.K., et al., “Senile asthenia” clinical recommendations, Ros. Zh. Geriatr. Med., 2020, no. 1, pp. 11–46. https://doi.org/10.37586/2686-8636-1-2020-11-46
Alberts, S.C., Archie, E.A., Gesquiere, L.R., et al., The male–female health–survival paradox: a comparative perspective on sex differences in aging and mortality, in Committee on Population; Division of Behavioral and Social Sciences and Education, Weinstein, M., and Lane, M.A., Eds., National Research Council, Sociality, Hierarchy, Health: Comparative Biodemography: A Collection of Papers, Washington (DC), National Academies Press (US), 2014.
Andreev, E.M., McKee, M., and Shkolnikov, V.M., Health expectancy in the Russian federation: a new perspective on the health divide in Europe, Bull. World Health Org., 2003, no. 81, pp. 778–788.
Angleman, S.B., Santoni, G., von Strauss, E., and Fratiglioni, L., Temporal trends of functional dependence and survival among older adults from 1991 to 2010 in Sweden: toward a healthier aging, J. Gerontol.: Series A, 2015, vol. 70, no. 6, pp. 746–752. https://doi.org/10.1093/gerona/glu206
Brainerd, E. and Cutler, D.M., Autopsy on an empire: understanding mortality in Russia and the former Soviet Union, J. Econ. Perspect., 2005, vol. 19, no. 1, pp. 107–130. https://doi.org/10.1257/0895330053147921
Babones, S.J., The consistency of self-rated health in comparative perspective, Publ. Hlth, 2009, vol. 123, no. 2, pp. 199–201. https://doi.org/10.1016/j.puhe.2008.12.016
Barbieri, M., Wilmoth, J.R., Shkolnikov, V.M., et al., Data resource profile: the human mortality database (HMD), Int. J. Epidemiol., 2015, vol. 44, no. 5, pp. 1–8. https://doi.org/10.1093/ije/dyv105
SHARE Wave 7 Methodology: Panel Innovations and Life Histories, Bergmann, M.A., Scherpenzeel, A., and Börsch-Supan, Eds., Munich: MEA, Max Planck Institute for Social Law and Social Policy, 2019. URL: http://www.share-project.org/fileadmin/pdf_documenta-tion/MFRB_Wave7/SHARE_Methodenband_A4_-WEB.pdf (accessed on March 17, 2021).
Börsch-Supan, A., Brandt, M., Hunkler, C., et al., Data resource profile: the survey of health, ageing and retirement in Europe (SHARE), Int. J. Epidemiol., 2013, vol. 42, no. 4, pp. 992–1001. https://doi.org/10.1093/ije/dyt088
Börsch-Supan, A. and Gruber, S., easySHARE. Release version: 7.1.0. SHARE-ERIC, 2020.https://doi.org/10.6103/SHARE.easy.710
Cambois, E., Robine, J.-M., and Mormiche, P., Did the prevalence of disability in France really fall in the 1990s? A discussion of questions asked in the French health survey, Population-E, 2007, vol. 62, no. 2, pp. 315–337. https://doi.org/10.3917/popu.702.0361
Carmona-Torres, J.M., Rodríguez-Borrego, M.A., Laredo-Aguilera, J.A., et al., Disability for basic and instrumental activities of daily living in older individuals, PLoS One, 2019, vol. 14, no. 7. e0220157. https://doi.org/10.1371/journal.pone.0220157
Christensen, K., Thinggaard, M., Oksuzyan, A., et al., Physical and cognitive functioning of people older than 90 years: a comparison of two Danish cohorts born 10 years apart, Lancet, 2013, vol. 382, no. 9903, pp. 1507–1513. https://doi.org/10.1016/S0140-6736(13)60777-1
Denisova, I., Adult mortality in Russia: a microanalysis, Econom. Transit., 2010, vol. 18, no. 2, pp. 333–363.https://doi.org/10.1111/j.1468-0351.2009.00384.x
ESS Round 9: European Social Survey Round 9 Data, Data file edition 3.1. NSD—Norwegian Centre for Research Data, Norway—Data Archive and distributor of ESS data for ESS ERIC. https://doi.org/10.21338/NSD-ESS9-2018
Guralnik, J.M., Alecxih, L., Branch, L.G., and Wiener, J.M., Medical and long-term care costs when older persons become more dependent, Amer. J. Publ. Hlth, 2002, vol. 92, no. 8, pp. 1244–1245. https://doi.org/10.2105/ajph.92.8.1244
Human Mortality Database, University of California, Berkeley (USA), and Max Planck Institute for Demographic Research (Germany). URL: http://www.mortality.org.
Idler, E. and Benyamini, Y., Self-rated health and mortality: a review of twenty-seven community studies, J. Hlth Soc. Behav., 1997, vol. 38, no. 1, pp. 21–37.
Jagger, C., Goyder, E., Clarke, M., et al., Active life expectancy in people with and without diabetes, J. Publ. Hlth, 2003, vol. 25, no. 1, pp. 42–46. https://doi.org/10.1093/pubmed/fdg009
Jagger C. and Robine, J.M., Healthy Life Expectancy, in International Handbook of Adult Mortality. International Handbooks of Population, Rogers, R. and Crimmins, E., Eds., Dordrecht: Springer, 2011, vol. 2.https://doi.org/10.1007/978-90-481-9996-9_26
Jia, H. and Lubetkin, E.I., Life expectancy and active life expectancy by disability status in older U.S. adults, PLoS One, 2020, vol. 15, no. 9. e0238890. https://doi.org/10.1371/journal.pone.0238890
Jitapunkul, S., Kunanusont, C., Phoolcharoen, W., et al., Disability-free life expectancy of elderly people in a population undergoing demographic and epidemiologic transition, Age Ageing, 2003, vol. 32, no. 4, pp. 401–405. https://doi.org/10.1093/ageing/32.4.401
Katz, S., Branch, L.G., Branson, M.H., et al., Active life expectancy, N. Engl. J. Med., 1983, vol. 309, no. 20, pp. 1218–1224. https://doi.org/10.1056/NEJM198311173092005
Keeler, E., Guralnik, J.M., Tian, H., et al., The impact of functional status on life expectancy in older persons, J. Gerontol.: Series A, 2010, vol. 65A, no. 7, pp. 727–733. https://doi.org/10.1093/gerona/glq029
Lubitz, J., Cai, L., Kramarow, E., and Lentzner, H., Health, life expectancy, and health care spending among the elderly, N. Engl. J. Med., 2003, vol. 349, no. 11, pp. 1048–1055. https://doi.org/10.1056/NEJMsa020614
Moreno, X., Albala, C., Lera, L., et al., Gender, nutritional status and disability-free life expectancy among older people in Santiago, Chile, PLoS One, 2018, vol. 13, no. 3. e0194074. https://doi.org/10.1371/journal.pone.0194074
Oksuzyan, A., Petersen, I., Stovring, H., et al., The male–female health–survival paradox: a survey and register study of the impact of sex-specific selection and information bias, Ann. Epidemiol., 2009, vol. 19, no. 7, pp. 504–511. https://doi.org/10.1016/j.annepidem.2009.03.014
Oksuzyan, A., Brønnum-Hansen, H., and Jeune, B., Gender gap in health expectancy, Europ. J. Ageing, 2010, vol. 7, no. 4, pp. 213–218. https://doi.org/10.1007/s10433-010-0170-4
Perlman, F. and Bobak, M., Determinants of self-rated health and mortality in Russia—are they the same? Int. J. Equity Hlth, 2008, vol. 7, р. 19 (2008), https://doi.org/10.1186/1475-9276-7-19
Permyakova, N.V. and Billingsley, S., Men’s health and co-residence with older generations in Russia: better or worse? J. Epidem. Commun. Hlth, 2018, vol. 72, no. 3, pp. 179–184. https://doi.org/10.1136/jech-2017-209896
Sullivan, D., A single index of mortality and morbidity, HSMHA Hlth Report, 1971, vol. 86, no. 4, pp. 347–354.
Zunzunegui, M.V., Nunez, O., Durban, M., et al., Decreasing prevalence of disability in activities of daily living, functional limitations and poor self-rated health: a 6-year follow-up study in Spain, Aging Clin. Exp. Res., 2006, vol. 18, no. 5, pp. 352–358. https://doi.org/10.1007/BF03324830
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
We declare that we have no conflict of interest. This article does not contain any studies involving animals or human participants performed by any of the authors.
Additional information
Translated by P. Kuchina
Rights and permissions
About this article

Cite this article
Papanova, E.K., Vorobyeva, N.M., Kotovskaya, Y.V. et al. Healthy Life Expectancy of People Over Age 65: Results of the Russian Epidemiological Study EVCALIPT. Adv Gerontol 12, 347–356 (2022). https://doi.org/10.1134/S2079057022040130
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S2079057022040130