
Abstract
The chronic extension of heart and blood-vessel walls due to hypertension leads to metabolic disorders in their interstitial matrix. To assess involutive and hypertensive changes in the cardiac and vascular interstitial matrix and to assess the their potential correction with Valsartan and Veroshpiron, 30 normotensive elderly women and 30 patients of the same age with stage-II arterial hypertension (AH) have been examined. Echocardiography and Doppler cardiography were carried out, the volume fraction of interstitial collagen (VFIC) in the myocardium and cardiovascular conjugation (CVC) was measured, and the serum concentrations of systemic collagenogenesis markers were determined. In elderly patients with AH, a higher intensity of LV myocardial fibrosis was found with a statistically significant increase in VFIC as compared to the patients with normal tension. This was due to the increased activity of fibrosis markers. A decrease in their levels was observed after antihypertensive therapy, which proved the antifibrotic effect of the therapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Metabolic disorders develop in the interstitial matrix of the heart and vessels in response to chronic extension of the walls of the heart and the blood vessels of the arterial bed, which is caused by arterial tension. First, fibroblast transforming growth factor β (TGF-β1) responds with increased activity; the synthesis of extracellular matrix proteins is then activated, and collagen synthesis increases. A consequence of these processes is myocardium remodeling, which follows complex pathogenic mechanisms, starting from the inflammatory response and ending with a regulatory imbalance in the metabolism of matrix metalloproteinases (MMPs) and disorders in the collagen synthesis mediated by these enzymes.
The chain of pathogenic metabolic transformations of the collagen synthesis system leads to fibrosis and vessel-myocardium rigidity. These changes are even more profound when underlined by involutive changes in the organism. They are characterized by the primary symptoms of fibrosis, modifications of the connective tissue interstitial matrix in target organs.
Despite the numerous studies and vast selection of antihypertensive drugs used to treat patients with arterial hypertension (AH), the question of the priority of certain drug groups remains unresolved. This is particularly so in regards to their efficiency in slowing fibrosis, decreasing vessel-myocardium rigidity, and compensating for collagen metabolism disorders in the interstitial matrix of heart and blood vessels.
In clinical treatment of AH, there are two currently predominant drug groups: angiotensin-converting enzyme inhibitors (ACE inhibitors) and angiotensin-II receptor blockers (ARB II and sartans). The years of experience with the use of ACE inhibitors to treat chronic AH, and target organ disorders as its consequence, led to the conclusion that ACE inhibitors show different efficiency in the blockage of the two angiotensin-II synthesis pathways, there being numerous bypass routes by which angiotensin I can be converted into angiotensin II with the subsequent development of AH. After angiotensinogen is produced in liver and other tissues in response to renin, it is transformed into angiotensin I, which is then modified with the production of angiotensin II upon increased ACE activity. The latter binds two receptor types: AT1-R and AT2-R [10]. The stimulation of AT1-R has vasoconstrictor, procoagulatory, and pro-proliferative effects with increased aldosterone synthesis, hypertrophic processes, and remodeling of cardiovascular system. The use of ACE inhibitors is often insufficient to counterbalance the described processes [5]. The use of ARB is suggested for the selective blockage of AT1-R [7, 11].
Angiotensin II stimulates the production of the steroid hormone aldosterone in the zona glomerulosa of the adrenal gland. This hormone acts on mineralocorticoid receptors in the kidneys, which, in turn, leads to an increase in the reabsorption of sodium ions and the excretion of potassium and hydrogen ions and enhances oxidative stress. The increase in the aldosterone content is the instrument of cardiovascular tissue remodeling due to the intensification of collagen synthesis, which, in turn, contributes to the increase in the rigidity of the vessel walls, left-ventricle (LV) myocardium hypertrophy, and kidney fibrosis.
The goal of the present study was to assess the efficiency of the long-term (six months) treatment of myocardial rigidity via the combined blockage of AT1-R with Valsartan and aldosterone receptors with Veroshpiron.
MATERIALS AND METHODS
The study involved 60 female patients of elderly age (average age—66 ± 0.7 years old). The main group included 30 female patients with stage-II AH, while the control group was formed by 30 almost healthy individuals of the same age and gender with normal AP. Informed consent was obtained from all patients. The disease duration in the patients with AH was 17 ± 1.06 years. The exclusion criteria were symptomatic AH, atherosclerosis at any location with clinical manifestation, chronic cardiac insufficiency (CCI) of functional classes III–IV according to the NYHA classification, cardiac-rhythm disturbance, hemodynamically relevant cardiac defects, acute cerebrovascular accidents, and myocardial infarction in the personal medical history. Individuals with obesity or lipid metabolism disorders, diabetes, concomitant kidney or liver impairments, thyroid gland disorders, systemic connective tissue disorders, anemia, malignant tumors, or respiratory and gastrointestinal disease in the acute phase were also excluded.
The thickness of the intraventricular septum and the left-ventricular (LV) posterior wall (TIVS and TPWLV) was determined, and the LV myocardium weight and stroke volume were calculated via echocardiography. The ejection fraction (EF) of the LV was calculated according to Teichholz’s formula. The index value was considered sufficient at ≥55%.
Cardiovascular coupling (CVC) was calculated according to the simplified formula ESP/ESV [1], where ESP is the end-systolic pressure and ESV is the end-systolic volume. A CVC index of 0.6–1.2 was considered optimal in the LV–artery interaction system.
To assess the degree of interstitial myocardial fibrosis, the volume fraction of interstitial collagen (VFIC) was calculated based on an analysis of the amplitude of the main peaks observed in a 12-lead ECG at rest and the LV myocardium mass calculated based on the echo-CG results with the formula proposed by Shirani et al. (1992) [12].
The serum levels of myocardium fibrosis markers, including fibroblast transforming growth factor β-1, matrix metalloproteinase (MMP-1), its tissue inhibitor (TIMP-1), and type-I collagen (COL-1), were measured via enzyme-linked immunosorbent assay (ELIZA). One of the markers of collagen synthesis, galectin-3 (Gal-3) was studied. It belongs to the lectin protein group, which binds β-galactosidase by a conservative element, the carbohydrate-recognition domain. It was demonstrated that Gal-3 plays a role in the pathogenesis of myocardial fibrosis; it is secreted into the extracellular space and thus stimulates fibrosis via fibroblast activation [5]. According to these studies, aldosterone stimulates the production of Gal-3 by myocardial macrophages. Gal-3, in turn, transmits the signal to fibroblasts, increasing their proliferation and pro-collagen-1 deposition [3].
The second part of the study consisted of the repeated laboratory examination of female patients with AH after six months of treatment with Valsartan at a dose of 80 mg/day (twice a day) with Veroshpiron at a fixed dose of 50 mg.
Statistical analysis of the obtained results was carried out with the Statistica 10.0 BIOSTAT software and nonparametric tests. The differences between groups were considered significant at p < 0.05. Correlations were measured with Pearson’s correlation coefficient.
RESULTS AND DISCUSSION
Table 1 lists the characteristics of both patient groups.
In patients with AH, the TIVS was 12.74 ± 0.22 mm, which was higher than the corresponding index values in the normotensive females, 9.43 ± 0.1 mm (p1–2 < 0.0000). The same was observed for TPWLV. It was 11.91 ± 0.17 in patients with AH, while it was 9.7 ± 0.16 (p1–2 < 0.0000) in females with normal AP. The observed changes pointed to hypertrophic processes in the studied heart compartments due to chronic excessive pressure overload.
Quantitative heart parameters are important for the characterization of the cardiac structural changes in AH. One of them, the myocardial mass, increased to 273.68 ± 10.1 as compared to normotensive individuals, 226.85 ± 5.91 (p1–2 < 0.0004). This indicated the presence of not only hypertonic but also involutive modifications of the heart. The VFIC in female patients with AH (12.03 ± 0.5%) was shown to be more than two times higher than that in the normotensive patients. This indicated an intensive synthesis of collagen in the myocardial interstitium.
All patients with hypertension were diagnosed with grade-1 diastolic disfunction (DD = 0.68 ± 0.02). No clinical signs of CCI were observed (LV EF = 53.9 ± 2).
Two weeks prior to blood collection, patients with AH were taken off antihypertensive medication except for rescue drugs (Capoten and Physiotens).
Valsartan was first prescribed at a dose of 80 mg/day (twice a day), combined with a fixed dose (50 mg) of Veroshpiron. If this sartan representative was well tolerated and had the expected effect with no observed side effects, the dose was doubled to 160 mg/day. Dose titration was performed with monitoring of the systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate, the dynamics of AH symptoms, and adverse effects. In the case of hypotension with SBP <110 mm Hg or other adverse effects of Valsartan, each patient returned to their individually selected, previously used dose. Laboratory examination was carried out at the start of the experiment and six months after the start of treatment.
Table 2 gives the blood plasma levels of collagen-1 and the regulators of its synthesis and degradation prior to the start of the therapy.
At the initial stage of the study, collagen synthesis in the extracellular matrix of myocardium predominated in patients with AH. Increased levels of fibroblast growth factor indicated the intensity of collagen production. Its activity was, to a certain extent, inhibited by the effects of MMP-1, which, in turn, was blocked by the corresponding inhibitor.
The content of Gal-3, one of the profibrotic molecules that are potential biomarkers of fibrosis and CCI development, was determined in blood plasma. Its activity in female patients with AH was 5.98 ± 0.2 ng/mL.
The relevant literature contains rather controversial data on the role of this molecule. According to Yu.V. Dubolazova [8], the Gal-3 levels in the blood serum of patients with CCI with retained normal EF was statistically higher than those in patients with decreased EF; at the same time, according to the results of the study performed by Fedorova et al. [10], a fourfold increase in Gal-3 levels was observed in patients with decreased LV EF [1].
These data supported the results of the studies from in the previous years, which provided solid evidence for the participation of Gal-3 in the development and progression of cardiac insufficiency; it was also demonstrated that increased Gal-3 levels are associated with severe cardiac insufficiency, disease progression, inflammation, and fibrosis [2].
The direct participation of Gal-3 in the pathogenesis of myocardial fibrosis was proved. It is secreted into the extracellular space at the injury site, thus stimulating fibrosis via fibroblast activation [6]. According to these studies, the stimulus for Gal-3 synthesis by myocardial macrophages appears to be aldosterone. Gal-3, in turn, transmits the signal to fibroblasts, which results in their increased proliferation and pro-collagen-1 deposition [2].
For example, some studies reported that there is a statistically significant correlation between Gal-3 levels and kidney dysfunction parameters in patients with CCI and that it plays a role in the processes of plasma oxidative stress in the patient after infarction [3, 4, 9]. However, its role as a marker of early manifestations of cardiovascular dysfunction is still unclear and requires further study and development.
In the present study, we demonstrated a direct correlation between collagen-1 and TGF-1 prior to the treatment, 0.62 (p < 0.0000), TIMP-1, r = 0.65 (p < 0.0007), and Gal-3, r = 0.6 (p < 0.0000), and a negative correlation between collagen-1 and MMP-1, r = ‒0.55 (0.0000).
Arterial-cardiac interaction, which is referred to as cardiovascular coupling (CVC) in literature, is considered one of the pathogenic factors of myocardial dysfunction. It reflects the interaction between the LV and the arterial network. An increase in CVC indices to 0.95 ± 0.09 c.u. were demonstrated for elderly patients with AH as compared to the corresponding indices in females with normal AP, 0.79 ± 0.03 c.u. (p < 0.05). These changes indicated an increasing rigidity of arterial walls with the subsequent changes in heart hemodynamics.
Strong correlation between collagen-1 and the volume fraction of interstitial collagen (r = 0.7, p < 0.0000) and CVC (r = 0.73, p < 0.0000) was found. The strong correlation between Gal-3 and the volume fraction of interstitial collagen (r = 0.99, p < 0.0000) and CVC (r = 0.95, p < 0.0000) almost completely reflected the highly important role of Gal-3 in the myocardial interstitial matrix and vascular-wall fibrosis.
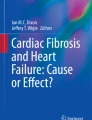
After six months of follow-up observations, all patients participating in the study successfully completed the Valsartan and Veroshpiron therapy. We observed that hemodynamic indices were stable in the course of the combined therapy. Figures 1–3 present the changes in the collagen biomarkers and collagen-1 concentration after the six-month course of the combined therapy.

TGF-β1 concentration in elderly patients with AH after six months of combined therapy.
In elderly age females with AH, we observed a statistical decrease in TFG-β1 activity to 1842.9 ± 20.2 pg/mL as a result of the antihypertensive therapy combining Valsartan and spironolactone. The difference was 12.4%. The observed decrease in the TGF-β1 concentration affected the quantitative collagen-1 indices (Fig. 2). The decrease in the COL-1 concentration from 202.32 ± 13.8 to 189.48 ± 14.3 pg/mL in patients after treatment indicated a decrease in the intensity of collagen synthesis by 6.3% and, correspondingly, inhibition of the fibrosis of the myocardial connective tissue matrix.

COL-1 level in elderly patients with AH after six months of combined therapy.
Figure 3 presents the changes in the new, poorly-studied Gal-3 marker. The study obtained significant results, indicating a decrease in the Gal-3 concentration from 6 ± 0.19 to 4.67 ± 0.1 ng/mL as a result of Valsartan and Veroshpiron treatment, which corresponds to 21.7%. The observed changes also confirm the lower intensity of collagen synthesis, and consequently, decreased heart muscle fibrosis. It was shown that there is a correlation between COL-1 and Gal-3 (r = 0.65, p < 0.0000), which supports the role of the latter in fibrosis. The results are in agreement with the conclusions made by other authors [3, 8].

Gal-3 concentration in elderly patients with AH after six months of combined therapy.
CONCLUSIONS
The results demonstrated the antifibrotic effects of the combined Valsartan + Veroshpiron therapy, which were confirmed by a decrease in the COL-1 level by 6.3% and indicated the direct participation of Gal-3 in collagenogenesis in the myocardial extracellular matrix.
REFERENCES
Andriyanova, A.V., Clinical features and neurohumoral mechanisms of development of manifest heart failure: innovative aspects of diagnostics and secondary prevention measures, Extended Abstract of Cand. Sci. (Med.) Dissertation, Tomsk, 2015.
Gorshunova, N.K., Medvedev, N.V., and Savich, V.V., Involute and hypertensive fibrous heart transformation during myocardial dysfunction and circulatory failure, Usp. Gerontol., 2018, vol. 31, no. 1, pp. 132–138.
Gyamdzhyan, K.A., Drapkina, O.M., and Maksimov, M.L., Galectin-3: clinical and prognostic role for examination of patients with chronic heart failure, Serdechnaya Nedostatochn., 2014, no. 1, pp. 51–55.
Gyamdzhyan, K.A., Kukes, V.G., and Maksimov, M.L., Clinical determination of galectin-3 in patients with chronic heart failure, Med. Sovet, 2017, no. 7, pp. 63–68.
Drapkina, O.M. and Kostyukevich, M.V., The effect of renin–angiotensin–aldosterone system blockers on myocardial remodeling and the risk of atrial fibrillation in patients with arterial hypertension, Klinitsist, 2012, nos. 3–4, pp. 73–79.
Drapkina, O.M. and Deeva, T.A., Galectin-3 is a biomarker of fibrosis in patients with metabolic syndrome, Ross. Kardiol. Zh., 2015, no. 9, pp. 96–102.
Drapkina, O.M. and Drapkina, Yu.S., Fibrosis and activity of the renin–angiotensin–aldosterone system: present and prospects, Arterial’naya Gipertenziya, 2012, vol. 18, no. 3, pp. 449–458.
Dubolazova, Yu.V., Evaluation of the clinical course of chronic heart failure with saved ejection fraction, Extended Abstract of Cand. Sci. (Med.) Dissertation, Moscow, 2012.
Medvedeva, E.A., Berezin, I.I., and Shchukin, Yu.V., Galectin-3, markers of oxidative stress and renal dysfunction in patients with chronic heart failure, Kardiologiya, 2017, vol. 57, no. 3, pp. 46–50.
Fedorova, N.V., Kashtalap, V.V., Hryachkova, O.N., and Barbarash, O.L., Galectin-3 in assessment of severity of coronary atherosclerosis in patients with ST-elevated myocardial infarction, Proc. Conf. “Materials of Acute Cardiovascular Care,” Vienna, 2015, p. 242.
Montezano, A.C., Callera, G.E., Yogi, A., et al., Aldosterone and angiotensin II synergistically stimulate migration in vascular smooth muscle cells through c–Src-regulated redox–sensitive RhoA pathways, Arterioscler., Thromb., Vasc. Biol., 2008, vol. 28, no. 8, pp. 1511–1518.
Shirani, J., Pick, R., Guo, Y., and Silver, M.A., Usefulness of the electrocardiogram and echocardiogram in predicting the amount of interstitial myocardial collagen in endomyocardial biopsy specimens of patients with chronic heart failure, Am. J. Cardiol., 1992, vol. 1, no. 69, pp. 1502–1503.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest. The authors declare no conflict of interest.
Statement of compliance with the standards of research involving humans as subjects. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all patients.
Additional information
Translated by E. Martynova
Rights and permissions
About this article

Cite this article
Gorshunova, N.K., Savich, V.V. Characteristics of Fibrosis and Collagen Metabolism Disorders in the Myocardial Interstitial Matrix of Patients with Arterial Hypertension and the Potential Use of Sartan Drugs for Their Treatment. Adv Gerontol 10, 234–238 (2020). https://doi.org/10.1134/S2079057020030078
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S2079057020030078