
Abstract
This study analyzed the relationship between LOX-1 and CX3CR1 and vascular endothelial function, fibrinolytic activity, and recurrence rate after thrombolysis in patients with cerebral infarction. Sixty patients with cerebral infarction who visited our hospital between May 2019 and April 2021 were enrolled as the study group, and 45 healthy individuals who underwent health checkups at our hospital during the same period were selected as the control group. The serum levels of LOX-1 and CX3CR1 in the study group were higher than those in the control group. The levels of serum LOX-1 and CX3CR1 were higher in the recurrence group than in the non-recurrence group. The study group had significantly lower plasma tPA and vWFp; higher plasma PAI-1; lower FMD levels; higher ba-PWV and ABI; and higher serum S100β, NSE, and NGF levels than those of the control group (P < 0.05). Pearson correlation analysis showed that LOX-1 and CX3CR1 levels in patients with cerebral infarction were positively correlated with PAI-1, ba-PWV, ABI, S100β, NSE, and NGF (r > 0, P < 0.05), and negatively correlated with tPA, vWF, and FMD (r < 0, P < 0.05). Serum LOX-1 and CX3CR1 levels are closely related to endothelial function, fibrinolytic activity, and neurological function in patients with cerebral infarction, and their combined detection can effectively predict the occurrence of cerebral infarction and recurrence after thrombolysis, which can be used to identify high-risk groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Cerebral infarction is a common cerebrovascular disease, which is defined by the World Health Organization as an acute onset of focal/hemispheric brain dysfunction caused by ischemic factors and lasting for more than 24 h. Most patients experience slowed blood flow, reduced blood pressure, and long-term cholesterol deposition in the intima of arteries, resulting in arterial tortuosity and deformation, increased fibers, fatty infiltration of the vessel wall, and large amounts of fibrin and platelets adhering to the vessel wall and forming vessels, which induces arterial occlusion [1–3]. Cerebral infarction accounts for 60–80% of the total incidence of cerebrovascular disease; has become the primary cause of disability and third cause of death in China; and is characterized by rapid onset, disease progression, and poor prognosis [4]. Currently, the key to the treatment of cerebral infarction is to restore the blood supply to the ischemic foci and promote recanalization of infarcted vessels as early as possible, which is often achieved through neurointerventional thrombolysis. However, relevant data have shown that there is still a reocclusion rate of 15% in the stenotic area after the procedure [5, 6]. Therefore, finding an effective predictor of cerebral infarction and prognosis after thrombolysis is particularly critical in identifying high-risk groups, adjusting drug doses and treatment regimens, and preventing re-infarction.
CX3C chemokine receptor 1 (CX3CR1) is mainly present on the surface of endothelial cells. When the vascular endothelium is damaged, CX3CR1 expression increases and causes aggregation of inflammatory factors, which activate the endothelial inflammatory response [7]. Lectin-like oxidized low-density lipoprotein receptor-1 (LOX-1) is the main receptor for oxidized low-density lipoprotein (ox-LDL) on the surface of atherosclerotic plaque cells and mediates biological behaviors, such as endothelial cell injury, activation, and apoptosis, which contribute to lipid aggregation in macrophages and smooth muscle cells, leading to thrombosis [8]. It has been found that CX3CR1 and LOX-1 accelerate the process of atherosclerosis and are associated with arterial vascular stenosis [9]. However, it is not clinically clear whether both are related to prognosis after cerebral infarction. In this study, we analyzed the relationship between LOX-1 and CX3CR1, cerebral infarction, and recurrence after thrombolysis.
MATERIALS AND METHODS
Clinical data. This study was approved by the Medical Ethics Committee of The First People’s Hospital of Wenling (approval number 2020PS58K) and performed in accordance with the Helsinki Declaration. The clinical data of 60 patients with cerebral infarction who visited our hospital from May 2019 to April 2021 were retrospectively collected as the study group. Forty-five healthy individuals who underwent physical examination at our hospital during the same period were selected as the control group. No randomization or blinding was performed to allocate the participants in the study.
(1) Inclusion criteria. Patients who met the diagnostic criteria for acute cerebral infarction in the Chinese Guidelines for the Diagnosis and Treatment of Acute Ischemic Stroke (2014) [10], had a time from onset to admission <72 h, had their condition diagnosed using cranial CT and MRI with imaging showing no obvious early hypointense changes, had first onset, were indicated for thrombolysis, had unilateral cerebral infarction, and had complete clinical data available were included in this study. The research participants and their families were informed, and they signed a fully informed consent form.
(2) Exclusion criteria. Patients with cerebrovascular malformation, cerebral aneurysm, Alzheimer’s disease, Parkinson’s disease, and other neurological diseases; hematologic diseases, serious infections, severe coagulation dysfunction, organic lesions of organs, cerebral infarction induced by arterial malformation or intracranial tumor, history of myocardial infarction within the past three months, history of serious trauma within two weeks, history of brain injury, brain surgery, and stroke; cerebral hemorrhage or subarachnoid bleeding; or where pregnant or currently lactating were excluded.
Methods. (1) Case sample size estimation [11]: tissue-type plasminogen activator (tPA), a common clinical indicator, was used as a reference for sample size estimation. The average plasma tPA level in the healthy population was 18.99 ± 4.17 ng/L, with a predicted difference of 3.5 ng/L and a confidence level of 1 − α = 0.95. PASS15.0 software was used to estimate the required sample size of each group (n = 30).
(2) Sample collection. Five milliliters of fasting peripheral elbow venous blood was collected from subjects in the study group before treatment and healthy individuals in the control group on the day of physical examination. Blood was collected using anticoagulant-free vacuum blood collection tubes and centrifuged at a low temperature for 5 min (3000 rpm, r = 10 cm) on an M1324R centrifuge (RWD Life Science Co., Ltd., Shenzhen, China) to separate the serum. The same amount of fasting peripheral venous blood was collected using vacuum blood collection tubes with EDTA. After centrifugation, the plasma was separated and stored at –80°C in a refrigerator for testing.
(3) Laboratory indicator tests. The levels of serum LOX-1, CX3CR1, nerve growth factor (NGF), neuron-specific enolase (NSE), and S100β protein (S100β) were measured using enzyme-linked immunosorbent assay (ELISA). The kits were purchased from R&D, USA. The Model 550 Microplate Reader was purchased from Bio-Rad Laboratories, Inc., Hercules, USA. Plasma levels of plasminogen activator inhibitor-1 (PAI-1), tPA, and von Willebrand factor (vWF) were measured using a double antibody sandwich ELISA, and the kits were purchased from Nanjing Novozymes Biotechnology Co.
(4) Vascular endothelial function. Brachial-ankle pulse wave velocity (baPWV) and ankle brachial index (ABI) were measured using an atherosclerosis meter (BP203RPE II model, Item no. 516828, Omron Colin, Japan), and endothelium-dependent flow-mediated vasodilation (FMD) was measured using a full-digital color Doppler ultrasound diagnostic instrument (UF-760AG model, Fukuda Denshi, Japan).
(5) Follow-up. The recurrence rate of cerebral infarction was determined at the follow-up 6 months after thrombolysis. If the condition of acute cerebral infarction improved or was basically cured, recurrence was considered if the original signs and symptoms were aggravated or new signs and symptoms of neurological deficits appeared, and the original lesions were enlarged or new lesions were visible on cranial CT or MRI. The researchers involved in the follow-up were blinded to the patients’ baseline data.
Statistical Analysis. Statistical analysis software (SPSS 23.0) was used to test normality using the Shapiro–Wilk test; measures with normal distribution are expressed as \(\bar {x}~\) ± s and were examined using an independent samples t-test. Pearson analysis was used to evaluate correlations, and receiver operating characteristic (ROC) curves were drawn to analyze the value of serum LOX-1 and CX3CR1 in predicting the occurrence of cerebral infarction and recurrence after thrombolysis. P < 0.05 indicated that the difference was statistically significant.
RESULTS
Baseline data. The study group included 34 men and 26 women, aged 43–76 years (mean, 62.43 ± 4.89 years), with a body mass index (BMI) of 18.45–23.09 kg/m2 (mean, 21.13 ± 1.06 kg/m2), with 12 patients with infarction in the internal capsule, 38 with infarction in the basal ganglia, and 10 with infarction in the radial crown. The diameter of the infarct lesion ranged 1–6 cm, with a mean diameter of 3.39 ± 0.72 cm. In the control group, there were 24 men and 21 women, aged 39–78 years old (mean, 61.94 ± 5.11 years), with a BMI of 18.97–23.65 kg/m2 (mean, 21.43 ± 0.98 kg/m2). The two groups were well-balanced in terms of sex, age, and BMI (P > 0.05).
LOX-1 and CX3CR1 levels and predictive value. The levels of serum LOX-1 and CX3CR1 in the study group were higher than those in the control group (P < 0.05). ROC analysis found that the AUCs of serum LOX-1, CX3CR1, and their combination for predicting cerebral infarction were 0.933 (95% CI: 0.887–0.978), 0.879 (95% CI: 0.811–0.947), and 0.941 (95% CI: 0.899–0.983) (Tables 1, 2 and Fig. 1).

ROC plot of serum LOX-1 and CX3CR1 for predicting cerebral infarction (n = 60).
Fibrinolytic activity. The plasma tPA and vWF levels in the study group were significantly lower, and PAI-1 levels were significantly higher than those in the control group (P < 0.05). This suggests that fibrinolytic function in patients with brain infarction is impaired, and the body is in a hypercoagulable state (Table 3).
Vascular endothelial function. The FMD of the study group was significantly lower than that of the control group, and the ba-PWV and ABI were significantly higher than those of the control group (P < 0.05). This suggests that patients with cerebral infarction had injured vascular endothelial cells (Table 4).
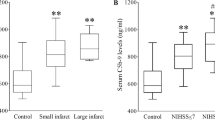
Neurological function markers. The serum S100β, NSE, and NGF levels of the patients in the study group were significantly higher than those in the control group (P < 0.05). Patients with cerebral infarction may have neurological impairments (Table 5).
Correlation. Pearson correlation analysis showed that LOX-1 and CX3CR1 levels in patients with cerebral infarction were positively correlated with PAI-1, ba-PWV, ABI, S100β, NSE, and NGF (r > 0, P < 0.05), and negatively correlated with tPA, vWF, and FMD (r < 0, P < 0.05) (Table 6).
Value of serum LOX-1 and CX3CR1 in predicting recurrence after thrombolysis. Serum LOX-1 and CX3CR1 levels were higher in the recurrence group than in the non-recurrence group (P < 0.05), and the ROC results showed that the AUCs of serum LOX-1, CX3CR1, and their combination for predicting recurrence after thrombolysis were 0.830 (95% CI: 0.715–0.946), 0.808 (95% CI: 0.678–0.938), and 0.845 (95% CI: 0.735–0.955) (Tables 7, 8 and Fig. 2).

ROC plot of serum LOX-1 and CX3CR1 for predicting recurrence after thrombolysis (n = 60).
DISCUSSION
Most studies have found that many chemokines and receptors, such as chemokine (FNK)/CX3CR1 and monocyte chemotactic protein-1 (MCP-1)/ chemokine receptor 2 (CCR2), produced locally in the brain tissue after cerebral ischemia, may interact with other cytokines by regulating leukocyte aggregation and chemotaxis, and participate in the inflammatory immune response to cerebral ischemia. Studies have confirmed that LOX-1 and CX3CR1 are associated with endothelial damage and arterial stenosis and can be used as predictors of ischemic heart disease [12–14]. Although endothelial damage and arterial stenosis are the main pathological changes in cerebral infarction, this study further analyzed the relationship between serum LOX-1 and CX3CR1 levels and cerebral infarction and prognosis.
LOX-1 is not only expressed in skeletal, cardiac, and vascular sites but is also distributed in endothelial cells, macrophages, vascular smooth muscle cells, and single nucleated cells [15]. Wang et al. [16] demonstrated that LOX-1 can induce apoptosis in endothelial and smooth muscle cells through the Bax/Bcl-2 metabolic pathway and exacerbate the instability of atherosclerotic plaques. Lin et al. [17] showed that LOX-1 can promote the release of HMGB1 from mitochondria to cytoplasm and nuclear to cytoplasmic translocation by regulating caveolin-1 phosphorylation, which contributes to macrophage recruitment and apoptosis of umbilical vein endothelial cells. Kobayashi et al. [18] found that LOX-1 is involved in atherosclerotic plaque formation by activating inflammatory cells to secrete inflammatory factors. CX3CR1 is a chemokine mostly expressed on the surface of endothelial cells and is associated with cell adhesion and involved in cell chemotaxis. Luo et al. [19] reported that the Fractalkine/CX3CR1 axis regulates synaptic plasticity and inflammatory cytokine release in neurological diseases. In this study, the levels of serum LOX-1 and CX3CR1 in the study group were higher than those in the control group, and were related to endothelial function, fibrinolytic activity, and neurological function. This may be because LOX-1 is involved in the atherosclerotic process by regulating the AMP-AMPK/PKC/NADPH signaling pathway and releasing a large amount of reactive oxygen species [20, 21]. Moreover, the rise of LOX-1 expression and ox-LDL binding can activate NF-kB signaling pathway, destroy vascular endothelial cells to activate platelets, induce inflammatory response, which leads to the deposition of large amounts of inflammatory cytokines in the intima, and inflammatory factors can increase plaque instability, causing plaque rupture, dislodgement and blockage of blood vessels, which aggravates the disease [22]. The downregulation of CX3CR1 can reduce the inflammatory response, modulate the immune response, and regulate the activation and function of microglia, neuronal survival, and synaptic function, thus protecting against brain injury. Yokota et al. [23] found that serum LOX-1 levels were highly expressed in patients with acute stroke, and that high levels of LOX-1 were independently associated with acute ischemic stroke (OR = 3.80, 95% CI: 1.86–7.74). Skarpengland et al. [24] reported a high serum LOX-1 level in patients with ischemic stroke, which is similar to the conclusion of this study.
Neurointerventional thrombolysis can effectively unblock blood vessels, rescue ischemic semi-dark zones, and repair damaged nerve cells in the area of cerebral infarction. However, it is affected by hardening, thickening, and loss of elasticity of the vessel wall, which certainly affects the normal coagulation system, leading to postoperative recurrence. Apostolakis [25] et al. suggested that CX3CL1/CX3CR1 pathway activity is associated with the risk of developing atherosclerotic disease and can be used as a prognostic/diagnostic biomarker. In the present study, serum LOX-1 and CX3CR1 levels in the recurrence group were higher than those in the non-recurrence group, and the AUC of serum LOX-1, CX3CR1, and their combination in predicting cerebral infarction and recurrence after thrombolysis were 0.830, 0.808, and 0.845, respectively, indicating that monitoring changes in serum LOX-1 and CX3CR1 levels may provide new targets for the prevention and treatment of cerebral infarction and drug development. However, there are some shortcomings in this study, such as the short follow-up time, small sample size, and single source, which may have affected the results. In addition, this study lacks relevant data on vascular risk factors and prescription of secondary prevention treatment, so it should be taken as a focus in subsequent studies. Observation time should be extended, and the sample size and source range should be expanded to further confirm study findings.
CONCLUSIONS
In conclusion, serum LOX-1 and CX3CR1 levels are closely related to endothelial function, fibrinolytic activity, and neurological function in patients with cerebral infarction, and their combined detection can effectively predict the occurrence of cerebral infarction and recurrence after thrombolysis, and identify high-risk groups.
REFERENCES
Sveinsson, O.A., Kjartansson, O., and Valdimarsson, E.M., Laeknabladid, 2014, vol. 100, no. 5, pp. 271–279.
Takeda, H., Yamaguchi, T., Yano, H., and Tanaka, J., J. Pharmacol. Sci., 2021, vol. 145, no. 1, pp. 130–139.
Shin, T.H., Lee, D.Y., Basith, S., Manavalan, B., Paik, M.J., Rybinnik, I., Mouradian, M.M., Ahn, J.H. and Lee, G., Cells, 2020, vol. 9, no. 7, pp. 1630.
Lee, S.U., Kim, T., Kwon, O.K., Bang, J.S., Ban, S.P., Byoun, H.S., and Oh, C.W., J. Korean Neurosurg. Soc., 2020, vol. 63, no. 1, pp. 69–79.
Heo, N.H., Lee, M.R., Yang, K.H., Hong, O.R., Shin, J.H., Lee, B.Y., Lee, J.Y., Ahn, J.M., Oh, H.J., and Oh, J.S., Medicine (Baltimore), 2021, vol. 100, no. 44, pp. e27652.
Güneş, Y., Sincer, I., and Erdal, E., Anatol. J. Cardiol, 2019, vol. 22, no. 2, pp. 54–59.
Pawelec, P., Ziemka-Nalecz, M., Sypecka, J. and Zalewska, T., Cells, 2020, vol. 9, no. 10, pp. 2277.
Kattoor, A.J., Kanuri, S.H., and Mehta, J.L., Curr. Med. Chem., 2019, vol. 26, no. 9, pp. 1693–1700.
Lu, J., Mitra, S., Wang, X., Khaidakov, M., and Mehta, J.L., Antioxid. Redox Signal, 2011, vol. 15, no. 8, pp. 2301–2333.
Chinese Society of Neurology; Chinese Society of Neurology Cerebrovascular Disease Group, Chinese Journal of Neurology, 2015, vol. 48, no. pp. 246–257.
Gao, T.L., Zhang, Z., Wen, S.J., and Zhang, N., Beijing Med. J., 2004, vol. 26, no. 2, pp. 86–89.
Pothineni, N.V.K., Karathanasis, S.K., Ding, Z., Arulandu, A., Varughese, K.I., and Mehta, J.L., J. Am. Coll. Cardiol., 2017, vol. 69, no. 22, pp. 2759–2768.
Stancel, N., Chen, C.C., Ke, L.Y., Chu, C.S., Lu, J., Sawamura, T., and Chen, C.H., Clin. Chem., 2016, vol. 62, no. 2, pp. 320–327.
Zeya, B., Arjuman, A., and Chandra, N.C., Biochemistry, 2016, vol. 55, no. 32, pp. 4437–4444.
Gliozzi, M., Scicchitano, M., Bosco, F., Musolino, V., Carresi, C., Scarano, F., Maiuolo, J., Nucera, S., Maretta, A., Paone, S., Mollace, R., Ruga, S., Zito, M.C., Macrì, R., Oppedisano, F., Palma, E., Salvemini, D., Muscoli, C., and Mollace, V., Int. J. Mol. Sci., 2019, vol. 20, no. 13, pp. 3294.
Wang, X.L., Yu, T., Yan, Q.C., Wang, W., Meng, N., Li, X.J., and Luo, Y.H., J. Mol. Neurosci., 2015, vol. 56, no. 2, pp. 449–460.
Lin, F., Pei, L., Zhang, Q., Han, W., Jiang, S., Lin, Y., Dong, B., Cui, L., and Li, M., J. Cell Physiol., 2018, vol. 233, no. 10, pp. 6683–6692.
Kobayashi, N., Takano, M., Hata, N., Kume, N., Yamamoto, M., Yokoyama, S., Shinada, T., Tomita, K., Shirakabe, A., Otsuka, T., Seino, Y., and Mizuno, K., Int. J. Cardiol, 2013, vol. 168, no. 4, pp. 3217–3223.
Luo, P., Chu, S.F., Zhang, Z., Xia, C.Y., and Chen, N.H., Brain Res. Bull., 2019, vol. 146, no. pp. 12–21.
Ding, Z., Liu, S., Wang, X., Dai, Y., Khaidakov, M., Romeo, F., and Mehta, J.L., Can. J. Physiol. Pharmacol., 2014, vol. 92, no. 7, pp. 524–530.
Hofmann, A., Brunssen, C., and Morawietz, H., Vascul. Pharmacol., 2017, pp. S1537–1891(17)30171-4.
Aoyama, T., Inokuchi, S., Brenner, D.A. and Seki, E., Hepatology, 2010, vol. 52, no. 4, pp. 1390–1400.
Yokota, C., Sawamura, T., Watanabe, M., Kokubo, Y., Fujita, Y., Kakino, A., Nakai, M., Toyoda, K., Miyamoto, Y., and Minematsu, K., J. Atheroscler. Thromb., 2016, vol. 23, no. 10, pp. 1222–1226.
Skarpengland, T., Skjelland, M., Kong, X.Y., Skagen, K., Holm, S., Otterdal, K., Dahl, C.P., Krohg-Sørensen, K., Sagen, E.L., Bjerkeli, V., Aamodt, A.H., Abbas, A., Gregersen, I., Aukrust, P., Halvorsen, B., and Dahl, T.B., J. Am. Heart Assoc., 2018, vol. 7, no. 2, pp. e006479.
Apostolakis, S. and Spandidos, D., Acta Pharmacol. Sin., 2013, vol. 34, no. 10, pp. 1251–1256.
Funding
No external funding was received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest. The authors declare that they have no conflicts of interest.
Ethical approval. This study was approved by the Medical Ethics Committee of The First People’s Hospital of Wenling (approval number 2020PS58K) and was performed in accordance with the Helsinki Declaration.
Informed consent. The research subjects and their families were informed, and they signed a fully informed consent form.
Additional information
Corresponding author: Department of Neurology, The First People’s Hospital of Wenling, No. 333, Chuanan South Road, Chengxi Street, Wenling, Zhejiang 317500, China; Phone: +86-13486878880; e-mail: jinxinchun@tom.com.
Rights and permissions
About this article

Cite this article
Huo, X.L., Shao, J.H., Wang, L.S. et al. Correlation between LOX-1 and CX3CR1 and Vascular Endothelial Function, Fibrinolytic Activity, and Recurrence after Thrombolysis in Patients with Cerebral Infarction. Neurochem. J. 16, 498–503 (2022). https://doi.org/10.1134/S1819712422040109
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S1819712422040109