
Abstract
The structural and physicochemical mechanisms of interaction of bone tissue with titanium implants under conditions of tuberculous osteitis are studied using scanning electron microscopy, X-ray diffraction analysis, IR spectroscopy, and thermal analysis. Physiological regeneration of bone tissue during treatment of tuberculous osteitis is accompanied by an increase in the organic component, embrittlement of the mineral phase of the bone matrix, and its decomposition to fine particles. The presence of titanium implants under physiological conditions contributes to the activation of the synthesis of the apatite phase in the regenerating bone. The primary mechanism of implantation osteogenesis in tuberculous osteitis is the formation of an inorganic phase of hydroxyapatite mainly in the regions of destruction of the titanium alloy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
The occurrence of bone defects as a result of injuries or some diseases (osteoporosis, osteoarthritis, diabetes mellitus, tuberculous osteitis, etc.) leads to the need for drug treatment or complete replacement of damaged bone tissue [1, 2]. When repairing bone defects, bioinert polymers [3] and inorganic composites [4, 5] are usually used, and with extensive injuries, metal implants prove to be useful [6, 7]. The use of implants based on titanium and its alloys to replace damaged bone tissue has been known for a long time [7–9], which is associated with the bioinertness and strength of these materials. The osseointegration of titanium implants is now believed to occur due to a titanium oxide film. The film acts as a chemisorbent of OH– ions, which increase the hydrophilicity of its surface and ensures high bone adhesion to the implant [8]. In some cases, the body reacts to the implant, which is due to microimpurities (iron, chlorine) in technically pure titanium or alloying additives (vanadium, aluminum, zirconium, etc.) in titanium alloys [9]. In addition, a cascade of reactions can be triggered under pathological conditions, which affect bone regeneration. So far, the features of osteogenesis occurring in the area of contact between bone tissue and titanium implants against the background of concomitant diseases remain poorly understood. In this regard, the goal of this study was to analyze the structure and physicochemical properties of regenerating bone tissue in contact with titanium implants under conditions of tuberculous osteitis during treatment.
1. SAMPLES AND METHODS OF RESEARCH
The experiments were performed using mature male Chinchilla rabbits in the experimental laboratory of the St. Petersburg Research Institute of Phthisiopulmonology. The animals were divided into the following groups (three animals in each): (1) healthy rabbits (control), (2) rabbits with simulated tuberculous osteitis, (3) rabbits with implanted titanium implants, and (4) rabbits with simulated tuberculous osteitis and implanted titanium implants. Tuberculous osteitis was simulated by introducing tuberculous mycobacteria into holes drilled in the femur. Tuberculosis therapy in Groups 2 and 4 was carried out according to the standard procedure.
We took samples of the epiphyses of the femur bones, cut out from the region being in contact with the surface of the VT-6 (Ti-6Al-4V) titanium implants for 2 months as the objects of study. Animals were removed from the experiment using lethal doses of Zoletil.
Scanning electron microscopy (SEM) was performed using an LEO 1420 microscope (Germany) with an energy-dispersive attachment for local elemental analysis (EDAX). Cleavages of the samples for microscopy were obtained in liquid nitrogen vapor, followed by fixation in 2.5% glutaraldehyde, dehydration in ethanol, and gold sputtering.
X-ray diffraction analysis (XRD) of bone tissue samples dried in air to constant weight was carried out using an ADVANCE D8 diffractometer (Bruker, Germany) using CuKα radiation with a wavelength of 1.5405 Å. The IR spectra of the samples were recorded using a Tensor-27 spectrometer (Bruker, Germany) in the range of 400–4000 cm–1. Samples for analysis were prepared by compressing powdered bone tissue into tablets with potassium bromide. The relative mineralization of the collagen matrix (apatite-to-collagen ratio) was estimated by IR spectroscopy from the ratio of the area of characteristic bands (900–1200 and 1550–1800 cm–1) corresponding to vibrations of the PO4 groups in the composition of hydroxyapatite (inorganic phase) and Amide I groups (organic phase) [10]. Thermogravimetry (TG), differential thermogravimetry (DTG), and differential thermal analysis (DTA) were carried out using a combined Netzsch STA 409 PC Luxx thermal analyzer (Germany); the heating rate was 10.0°C/min in air; and the sample weight was 40 ± 10 mg.
2. RESULTS AND DISCUSSION
2.1. Regenerating Bone Tissue (Group 1)
According to SEM, in the regenerating bone tissue, foci of remodeling in the form of clusters of osteoblasts with characteristic processes on the surface (Fig. 1a) and bone plates growing in the cavity of the intercellular space of the bone matrix (Fig. 1b) are observed.

SEM images of (a, b) healthy bone tissue and (c, d) bone tissue during treatment of tuberculosis: (a) with foci of remodeling of bone matrix (b) with newly formed bone plates, (c) with matrix vesicles in the cytoplasm and organomineral cytoplasmic outgrowths, and (d) with the growth of bone trabeculae.
In X-ray diffraction patterns of healthy bone tissue samples, broadened diffraction peaks of amorphized calcium phosphate are seen with the main reflections in the 2θ range of 30°–35° (Fig. 2a, diffractogram 1). These peaks are typical of both nonstoichiometric hydroxyapatite (n-HA) and carbonate-substituted hydroxyapatite (c-HA) (Table 1).

(a) X-Ray diffraction patterns and (b) IR spectra of the samples of (1, 3) healthy bone tissue and (2, 4) bone tissue during treatment of tuberculosis: (1, 2) physiological regeneration and (3, 4) regeneration with titanium implants.
IR spectroscopy data show that in a healthy bone, there are intense bands in the region of 3200–3600 cm–1 (Fig. 2b, curve 1), caused by stretching vibrations of the associated O–H and N–H groups in the three-dimensional structure of collagen, as well as the presence of adsorbed water. The bands at 2927 and 2856 cm–1 correspond to vibrations of the C–H groups of the polypeptide chain, and the bands at 1745 cm–1 are for vibrations of the C=O and N–H groups of the glycine amino acid residue in the primary protein structure. The apatite phase of bone tissue appears at 455 and 565 cm–1 (planar deformation vibrations of the PO4 groups) and at 930–990 and 975–1140 cm–1 (stretching vibrations of the PO4 groups). The free О–Н group of n-HA in the IR spectrum of the control sample is practically invisible, which indicates a distortion of the crystal lattice of the hydroxyapatite phase and its binding to collagen due to hydrogen bonds. In addition, isomorphic substitutions of О–Н (A-type substitution) and PO4 groups (B-type substitution) to carbonate groups also lead to distortions in the crystal lattice of hydroxyapatite. In the IR spectrum, these bands are seen at 1545 cm–1 (asymmetric vibrations of C–O bonds of A-type carbonate groups of c-HA), 1465 and 1410 cm–1 (asymmetric vibrations of C–O bonds of B-type carbonate groups of c-HA), and at 873 cm–1 (vibrations of O–C–O bonds of B-type carbonate groups of c-HA). We note that the assignment of certain absorption bands only to the hydroxyapatite component of the bone is conditional, since the vibrations of C–O bonds can also be caused by functional groups of collagen amino acid residues. In this regard, the calculated values of relative mineralization of the collagen matrix are estimates, and the apatite-to-collagen ratio in the control sample is 48/52 (Table 2).
The results of XRD and IR spectroscopy are confirmed by thermal analysis data (Fig. 3). Weight loss of the samples is observed in temperature ranges of 50–200, 200–400, 400–550, and 550–900°C. First, structural water is lost (9%); at the second stage, low-molecular-weight organic substances and noncollagenous proteins are removed; and above 400°C, high-molecular-weight organic substances and collagen are decomposed, which is consistent with published data [11]. Considering that the organic phase begins to be removed only in the second stage, its content when recalculated for dehydrated samples is 49% (Table 2).

(a) Thermogravimetry and differential thermogravimetry data and (b) IR spectra of the samples of (1, 3) healthy bone tissue and (2, 4) bone tissue during treatment of tuberculosis: (1, 2) physiological regeneration and (3, 4) regeneration with titanium implants.
2.2. Regenerating Bone Tissue with Tuberculosis Osteitis Under Treatment (Group 2)
According to SEM data (Figs. 1c and 1d), morphological signs of imbalance of remodeling processes with a shift towards excessive osteogenesis were revealed in bone tissue samples with treated tuberculosis osteitis. This is manifested in the form of uncontrolled proliferation of bone trabeculae, obliteration of micropores, and microfitization of the bone matrix.
Using XRD and IR spectroscopy, we found that after treatment of tuberculous osteitis, the amount of n-HA increases (Table 1) and the concentration of the apatite phase decreases (Table 2). Moreover, the trend in the ratio of inorganic and organic phases according to two types of analysis (IR spectroscopy and DTA) coincides.
The bands corresponding to vibrations of the functional groups of c-HA of mixed AB-type are observed in the IR spectrum (Fig. 2b, curve 2). The presence of carbonate groups in the crystal lattice of hydroxyapatite promotes a particular approximation of calcium and oxygen atoms in the composition of hydroxyl groups, which leads to the formation of “calcification” centers. The appearance of such structural changes can affect the micromechanical properties of the mineral phase of the bone matrix and enhance its “binding” properties.
2.3. Regenerating Bone Tissue with Implanted Titanium Implants (Group 3)
When titanium implants are introduced into the bone tissue of healthy animals, according to SEM data (Fig. 4a), characteristic bone plates are revealed in the interface region, indicating active regeneration. It is essential that the structure of the titanium implant remains uniform, without cracks, which indicates its safety under physiological conditions.

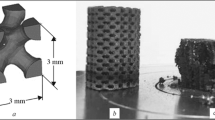
(a) SEM images of the interface region of the implant with healthy bone tissue in the growth zone and (b) structure of the deep layers of the titanium implant cut during treatment of tuberculous osteitis.
The XRD data indicate that in the bone tissue samples extracted from the implant region, the intensity of the main reflection is slightly lower compared to the samples of Groups 1 and 2 (Fig. 2a, diffractogram 3), and there is a tendency towards increased concentration of the n-HA phase relative to the c-HA phase (Table 1). This indicates the tendency of the bone tissue to restore the apatite phase in the matrix of regenerating bone.
In the IR spectrum, the intensity of the bands in the region of stretching vibrations of the O–H and N–H groups, responsible for the hydrogen bond, decreases at 3600–3200 cm–1 (Fig. 2b, curve 3). The bands corresponding to the carbonate groups are observed only for B-type c-HA. In comparison with the control sample, the intensity of the bands corresponding to vibrations in the functional groups of both the organic component and the mineral phase of the bone tissue decreases. Consequently, the degree of amorphism of the apatite component of bone tissue during implantation of titanium matrices increases. According to the data calculated by both IR spectroscopy and DTA (Table 2), the concentration of the inorganic phase increases compared to samples of the previous groups (without implants). This means that, in comparison with physiological regeneration, titanium implants have a stimulating effect on the processes of reparative regeneration.
According to DTA data (Fig. 3), dehydration occurs up to 200°C with almost the same rates for all bone tissue samples. It is noteworthy that, starting from 350°C, the decay rate of collagen proteins for different groups varies. In particular, during the regeneration of bone tissue in the cases of tuberculosis, more intense decomposition of the organic phase is recorded in the samples compared to the control group. Significant differences are observed for samples in the range of 600–900°C; namely, during implantation osteogenesis, in comparison with the control sample, a more significant amount of the inorganic phase remains in the dry residue. This means that under indicated conditions, the formation of the inorganic phase occurs faster than in the control sample.
2.4. Regenerating Bone Tissue with Implanted Titanium Implants in the Treatment of Tuberculous Osteitis (Group 4)
SEM data indicate that the main features in this group of samples are multiple erosion and lytic channels with scalloped edges of defects in the deep layers of titanium implants (Fig. 4b). It is crucial that the newly formed bone tissue grows deep into the corroded implant. In this case, migration of small osteogenic precursor cells into the gap with a size of up to 5–10 μm is observed. In sections of larger volume, cells differentiate into mature osteoblasts with embryonic bone plates. In general, the structure of the contact area with an implant is nonuniform, which creates the conditions for a significant variation in the acid–base equilibrium of tissue fluid. In particular, regions with an alkaline environment contribute to titanium corrosion, as evidenced by the predominant deposition of hydroxyapatite in corrosion zones.
According to XRD data, in the regenerating bone tissue with implanted titanium implants in the case of tuberculous osteitis, compared with physiological regeneration (Group 3), there is a slight increase in the crystallinity of the inorganic phase and an increase in the crystallite size of both n-HA and c-HA (Fig. 2a, diffractogram 4; Table 1). In the IR spectrum, a shift of the strong Amide I band, corresponding to carbonyl absorption at 1745 cm–1, and the stretching vibration band of С–О at 1165 cm–1 are observed (Fig. 3, curve 4) in comparison with similar samples of healthy bone tissue. The absence of a peak at 1540 cm–1, according to [10], indicates the predominance of B-type c-HA in these samples. An increase in the concentration of the inorganic phase (Table 2) in the samples of regenerating bone tissue with implanted titanium implants after treatment of tuberculous osteitis indicates a less intensive growth of connective collagen tissue compared with bone tissue without an implant under these conditions. In addition, samples of bone tissue of Group 4 are characterized by higher heat resistance associated with dense packing of collagen fibers, which makes it difficult to remove volatile decomposition products of organic compounds from samples [12]. This is manifested in the DTA curves as the shift of thermal effects to the region of high temperatures at the 3rd and 4th stages. It is noteworthy that with regenerative tuberculosis osteitis, a more substantial decrease in the inorganic phase is observed than with implant osteogenesis under tuberculosis osteitis; that is, titanium in tuberculosis conditions make a higher contribution to the formation of the hydroxyapatite phase than the physiological norm.
CONCLUSIONS
Bone tissue regeneration under physiological conditions and with tuberculous osteitis is implemented under various structural-phase transformations of the inorganic and organic phases. Regeneration of bone tissue during treatment of tuberculous osteitis is characterized by a decrease in the concentration of the apatite phase with a predominance of n-HA (up to 77%), tending to a stable stoichiometric form. In this case, the bone matrix is destroyed by a fragile mechanism with disintegration into fine particles.
Under physiological conditions, implantation osteogenesis is accompanied by the intensive formation of an inorganic phase with a-HA/c-HA ratio tending to normal.
In tuberculosis osteitis, titanium implants undergo alkaline corrosion with local deposition of hydroxyapatite, which is a crucial factor that triggers reparative osteogenesis.
REFERENCES
A. A. Gaidash, L. N. Sinitsa, O. A. Babenko, and A. A. Lugovskoy, J. Osteoporosis 2011, 162041 (2011). https://doi.org/10.4061/2011/162041
S. M. Jung, K. W. Kim, C.-W. Yang, S.-H. Park, and J. H. Ju, J. Immunol. Res. 2014, 263625 (2014). https://doi.org/10.1155/2014/263625
O. I. Agapova, Sovrem. Tekhnol. Med. 9, 190 (2017). https://doi.org/10.17691/stm2017.9.2.24
V. K. Krut’ko, A. I. Kulak, and O. N. Musskaya, Inorg. Mater. 53, 429 (2017). https://doi.org/10.1134/S0020168517040094
O. N. Musskaya, A. I. Kulak, V. K. Krut’ko, Yu. A. Lesnikovich, V. V. Kazbanov, and N. S. Zhitkova, Inorg. Mater. 54, 117 (2018). https://doi.org/10.1134/S0020168518020115
T. D. Sargeant, M. O. Guler, S. M. Oppenheimer, A. Mata, R. L. Satcher, D. C. Dunand, and S. I. Stupp, Biomaterials 29, 161 (2008). https://doi.org/10.1016/j.biomaterials.2007.09.012
A. A. Yanovska, A. S. Stanislavov, L. B. Sukhodub, V. N. Kuznetsov, V. Yu. Illiashenko, S. N. Danilchenko, and L. F. Sukhodub, Mater. Sci. Eng. C 36, 215 (2014). https://doi.org/10.1016/j.msec.2013.12.011
F. Barrerea, M. M. E. Snelc, C. A. Van Blitterswijka, K. De Groota, and P. Layrollea, Biomaterials 25, 2901 (2004). https://doi.org/10.1016/j.biomaterials.2003.09.063
S. Ichinose, T. Muneta, I. Sekiya, S. Itoh, H. Aoki, and M. Tagami, J. Mater. Sci.: Mater. Med. 14, 79 (2003). https://doi.org/10.1023/A:1021557605458
A. L. Boskey, E. Donnelly, E. Boskey, L. Spevak, Y. Ma, W. Zhang, J. Lappe, and R. R. Recker, J. Bone Miner. Res. 31, 1070 (2016). https://doi.org/10.1002/jbmr.2759
S. A. Lemesheva, O. A. Golovanova, and S. V. Turenkov, Chem. Sustainable Dev. 17, 327 (2009).
S. A. Lemesheva, O. A. Golovanova, I. V. Muromtsev, and S. V. Turenkov, Vestn. Omsk. Univ., No. 2, 106 (2010).
Funding
This work was supported by the State Research Program Chemical Technologies and Materials (assignment 1.04).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
CONFLICT OF INTEREST
The authors declare that they do not have any conflicts of interest.
STATEMENT OF THE WELFARE OF ANIMALS
The experimental protocols, including the content and method of euthanasia, agree with the ethics committee of the St. Petersburg Research Institute of Phthisiopulmonology and comply with the Rules for the Maintenance of Laboratory Animals, approved by Order of the Ministry of Health of the Russian Federation.
Additional information
Translated by O. Zhukova
Rights and permissions
About this article

Cite this article
Musskaya, O.N., Krut’ko, V.K., Gaidash, A.A. et al. Structure and Physicochemical Mechanisms of Interaction of Bone Tissue with Titanium Implants in Cases of Tuberculous Osteitis. Tech. Phys. 64, 1898–1903 (2019). https://doi.org/10.1134/S1063784219120193
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S1063784219120193