
Abstract
Pendant drop and bubble shape methods are employed to study the tensiometric and rheological parameters of blood serum and plasma in 45 patients 49–70 years old subjected to surgical operations under the conditions of artificial circulation because of ischemic heart disease (first group) and heart valve pathology (second group). Blood sampling is performed 1 h before and 12 h after (the first day) the operation, as well as on the 7th postoperative day. Statistically significant changes in the surface tension and viscoelasticity modulus are observed on the 1st day after the operation in both groups, thereby indicating a substantial increase in the content of surfactants in the blood serum. On the seventh day of the postoperative period, a positive dynamics is observed; however, the studied rheological parameters—in particular, viscoelasticity modulus E—at frequencies of 0.1 and 0.01 Hz statistically reliably exceed their preoperative level and do not reach the values characteristic of healthy people. Thus, the pathological deviations of biochemical parameters (contents of glucose, urea, creatinine, albumin, and lipoproteins) that affect blood viscosity are accompanied by substantial changes in the surface tension and dilatational viscoelasticity of blood serum. However, the examined biochemical markers are not dominating predictors for changes in the rheological and tensiometric properties of blood.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
INTRODUCTION
The main pathogenic factors of thrombogenesis (disruptions of vascular walls, activation of blood clotting, and deceleration of bloodstream) are regularly revised; as a result, the notions of the specific mechanisms for each of them are refined [1–7]. The timely diagnosis of patients with ischemic heart disease (IHD) reduces the number of unfavorable pathologic processes, in particular, atherosclerotic injury to great vessels, which is relevant to the manifestations of multifocal atherosclerosis. A high level of proatherogenic lipids that exhibit surface-active properties is observed in the blood serum of many such patients [6]. It should be noted that the number of works devoted to studying the interfacial (adsorption and rheological) characteristics of blood serum and plasma at different pathologies [8–12] is increasing. The history of studying the surface tension of blood and other biological fluids in the last 100 years and the main methods used for these purposes have been described in monograph [9]. The authors of review [12] have reported data obtained at Gorky Donetsk National Medical University for 25 years by tensiometry and surface rheometry on biological fluids of patients with several tens of different diseases. Let us present a few examples. The values of the dynamic and equilibrium surface tensions of blood decrease by 5–10 mN/m in oncological, rheumatological, neurological, and some other diseases. On the contrary, the surface tension of blood increases in diabetic neuropathy and scleroderma. The viscoelasticity modulus of blood strongly changes in some diseases; it doubles in glomerulonephritis and renal insufficiency, but decreases in gout.
Various methods, such as the Du Nouy ring detachment, pendant drop, bubble shape, and maximum bubble pressure methods, have been employed to study biological fluids. It has been found that the two latter methods are the best. They enable one to measure the surface tension within a time period of 0.01–10 000 s and determine its dynamic and equilibrium values, as well as the viscoelasticity modulus and phase angle. It is of great importance that a small amount of biological fluid (no more than 5 mL) is required to realize these methods. Blood contains various surfactants, such as albumins, globulins, fibrinogen, creatinine, creatine, glucosamine, pentoses, lipids, triacylglycerols, phospholipids, phosphatidylcholine, and several tens of others. More than ten types of surface active acids (citric, succinic, uric, lactic, acetoacetic, and other acids) are present in blood. Diseases affect the chemical composition of biological fluids, including the concentrations of the aforementioned surfactants. Total chemical analysis of blood is a complex and expensive procedure, while the measurements of the surface tension and dilatational viscoelasticity are relatively simple and accessible methods for obtaining integral characteristics of blood and other biological fluids.
In this work, we studied the surface tension and dilatational rheology of blood serum and plasma in IHD with valvular defects. Substantial changes have been observed in the surface tension and viscoelasticity modulus of patient’s blood serum and plasma.
EXPERIMENTAL
Surface tension γ and dilatational viscoelasticity were studied by the pendant drop and bubble shape methods using PAT-1 and PAT-2 tensiometers (SI-NTERFACE Technologies, Germany). The procedures are described in detail elsewhere [13]. A drop of blood serum or plasma was formed at a vertical capillary with internal and external diameters of 1 and 3 mm, respectively. The edge of the capillary had an internal diameter of 2.96 mm; i.e., the capillary walls were rather thin, so as to exclude the influence of the contact angle on the shape and size of the drop. The drop surface area was automatically kept constant during the experiment within a range of 34–36 mm2 at any value of γ. The volume of the formed drop was equal to 24–25 mm3 and decreased during adsorption because of a reduction in γ and a variation in the drop shape. The dilatational rheology of blood serum was experimentally studied after equilibration, which required 2000–2500 s from the moment of drop formation (see below).
Dilatational modulus E characterizes the viscoelastic properties of the surface (interfacial) layers. Modulus E is determined as the ratio of a change in solution surface tension γ to relative change in surface area A:
The experiments were performed in the mode of harmonic oscillations of the drop surface area with an amplitude of ±8% and a frequency of 0.5–0.005 Hz. The error in the determination of the surface tension with the PAT-2 and PAT-1 instruments was 0.1 mN/m. The error in the determination of the viscoelasticity modulus was several times larger and amounted to nearly 0.6 mN/m. When measuring the rheological parameters with the PAT tensiometers, the oscillation frequency and amplitude, as well as the number of cycles, were preset. The rheological parameters were calculated with the help of the software supplied with the PAT-2 instrument using the Fourier transformation and the model described in [14].
Dilatational modulus E is a complex parameter, which comprises real and imaginary components [15, 16]:
Real Er and imaginary Ei components of dynamic surface elasticity E make it possible to determine the absolute value of this parameter and phase angle ϕ:
Here, \(\left| E \right|\) is viscoelasticity modulus and ϕ is the phase angle between the maxima of variations in the surface area (deformation) and surface tension.
Note that the results obtained by the pendant drop shape method may differ from those obtained for a planar liquid surface. For a planar surface on which a surfactant is adsorbed by the diffusion mechanism, the components of the modulus are determined by the following equations [15, 16]:
Parameter \(\zeta = \sqrt {{{{{\omega }_{{\text{D}}}}} \mathord{\left/ {\vphantom {{{{\omega }_{{\text{D}}}}} {2\omega }}} \right. \kern-0em} {2\omega }}} \) comprises angular frequency ω and diffusion relaxation frequency \({{\omega }_{{\text{D}}}}\left( c \right) = D{{\left( {{{d\Gamma } \mathord{\left/ {\vphantom {{d\Gamma } {dc}}} \right. \kern-0em} {dc}}} \right)}^{{ - 2}}}.\) The value of \({{E}_{0}}\left( c \right) = {{ - d\gamma } \mathord{\left/ {\vphantom {{ - d\gamma } {d\ln \Gamma }}} \right. \kern-0em} {d\ln \Gamma }}\) is the limiting elasticity, while parameters c, Γ, and D are the volume concentration, adsorption value, and diffusion coefficient, respectively. Equations (4) may be written in another form:
Joos has derived the following equation for the case of adsorption from the bulk of a spherical drop with radius R on its surface [17]:
where \({{n}^{2}} = {{i\omega } \mathord{\left/ {\vphantom {{i\omega } D}} \right. \kern-0em} D}.\) It should be noted that, for the used values of the drop volume and oscillation frequency, the results of the calculations by Eq. (6) are lower than those obtained by Eqs. (5) at the same parameters for a planar surface by only a few percent.
Seventeen healthy people 5–75 years of age (average age of 61 years) were examined. They composed a blank group. In addition, 45 patients 49–70 years of age (average age of 62 years) were examined. They were divided into two groups containing 18 and 27 people. The patents of the first group were subjected to prosthetics of the mitral and aortic valves. The patients of the second group were subjected to coronary artery bypass grafting (two to five bypasses). All operations were performed under the conditions of artificial circulation. Blood of all patients was sampled 1 h before the operations and 12 h after the operations (the first day), as well as on the seventh day of the postoperative period.
Statistical data processing was carried out using the Microsoft Excel and Statistica programs. The mean values, errors of mean, and Student’s t-tests were calculated, and significance level p was estimated according to Student.
RESULTS AND DISCUSSION
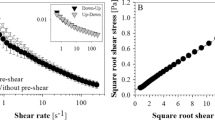
Figure 1 shows the dynamic surface tension curves for blood serum of (1) a healthy volunteer and (2) a patient with IHD. It is seen that the curve for the patient lies substantially lower and the equilibrium values of γ are reached over 1500–2000 s. Therefore, oscillations of the drop surface area were initiated in the rheological experiments at times longer than 2000 s.

Dynamic surface tension of the blood serum of (1) a healthy person and (2) a patient with IHD.
Table 1 presents the results of examining blood serum and plasma of patents from the two aforementioned groups before the operations. The six following parameters are shown: dynamic surface tension at an adsorption time of 100 s, equilibrium surface tension (adsorption time of 2500 s), viscoelasticity moduli \(\left| E \right|\) at oscillation frequencies of 0.1 and 0.01 Hz, and phase angles ϕ at these frequencies. The aforementioned tensiometric and rheological parameters are most informative [9–12]. The values of the surface tension at times of 0.01 and 1 s were determined by the maximum bubble pressure method using an MPT or BPA tensiometer.
It follows from Table 1 that these parameters for the two groups of patients are almost identical. For serum, the moduli are somewhat different at frequencies of 0.1 and 0.01 Hz, while the phase angles differ at 0.01 Hz. For plasma, the phase angle has different values at the frequency of 0.01 Hz.
A substantial difference in the values of the dynamic and equilibrium surface tensions for serum and plasma should be noted: they are substantially higher for plasma. That is, the content of surfactants in plasma is lower than that in serum. At the same time, the viscoelasticity moduli at the considered frequencies are markedly higher for plasma in both groups of patients, while the phase angle at 0.01 Hz is higher for the first group. The latter finding suggests a high value of the imaginary component of viscoelasticity, i.e., a high surface viscosity.
Table 2 shows the results of the tensiometric and rheological examinations of serum in healthy people and the patients of the first group before and after the operations. The same six parameters as those in Table 1 are presented. If the difference in a parameter for patients and healthy people is statistically reliable, the value of Student’s p coefficient is presented in addition to the mean value and the error of mean of the parameter.
As follows from Table 2, almost all parameters of patients' serum (with the exception of ϕ at 0.1 Hz) reliably differ from the corresponding parameters of the serum of healthy people.
Table 3 presents the corresponding data on sera of patients from the second group. It is seen that, for the patients of the second group, almost all parameters (with the exception of viscoelasticity moduli at 0.1 and 0.01 Hz) also reliably differ from those for healthy people. A very strong change is seen in the values of γ for patients of the first and second groups. Both dynamic (at 100 s) and equilibrium surface tensions of serum for patients are lower than those for healthy people by 6–7 mN/m. This indicates a substantial increase in the content of surfactants in the patient’s blood. This may be caused by a marked increase in the concentration of urea and creatinine in IHD, with these substances being able to increase the surface activity of albumin and other proteins. Moreover, in IHD, the composition of lipids in blood is changed (the concentrations of high- and low-density lipoproteins, triglycerides, and cholesterol are increased) and the concentrations of glucose and immunoglobulins G, M, and A are elevated. In addition, the content of C-reactive protein rises and the balance of cytokines is violated. All these facts may lead to an increase in the concentration of surfactants in patients' blood.
Changes in the biochemical composition of blood and their effect on its surface tension may be illustrated by the example of patients suffering from oncological diseases [12]. Increased concentrations γ-globin, β2-microglobin, α2-glycoproten, ferrite, immune complexes, T-globulin, α-antitrypsin, fatty acids, mucoids, and other components have been revealed in their blood. The content of some of the aforementioned components may also be changed in IHD, thereby decreasing the blood surface tension.
Concerning the rheological parameters presented in Table 2, it may be noted that modulus E at a frequency of 0.01 Hz is strongly increased with a concomitant decrease in the phase angle. This attests to a rise in the surface elasticity at an almost unchanged surface viscosity.
It has been found that the operations have no effect on the subsequent variations in the parameters for patients of the first and second groups and their approach to the parameters of healthy people. Most probably, 7 days are insufficient for changes in the composition of patients’ blood sera.
The studies of plasma analogous to the examinations of serum have shown that, in the first group of patients, the viscoelasticity modulus and phase angle at 0.01 Hz reliably increase after operations approaching the values characteristic of healthy people. These parameters of the patients before the operations were lower than those of healthy people. For example, the phase angles for healthy people and patients before and after the operations are 40.2°, 35°, and 39°, respectively. For the plasma of the second-group patients, it has been revealed that the dynamic surface tension (at 100 s) after the operations reliably increases approaching the plasma surface tension of healthy people.
CONCLUSIONS
The pendant drop shape method has been used to experimentally study the surface tension and dilatational viscoelasticity of blood serum and plasma of healthy people and patients with IHD before and after surgical operations. The values of the dynamic and equilibrium surface tensions, viscoelasticity moduli at oscillation frequencies of 0.1 and 0.01 Hz, and phase angles at these frequencies have been determined. The obtained results indicate reliable differences between some of these parameters for the patients before and after operations and healthy people. These results are likely to improve the diagnostics and treatment of patients with IHD and acquired valvular defects.
REFERENCES
Grin’, V.K., Anikeeva, T.V., and Sinyachenko, O.V., Porazhenie sosudov pri ishemicheskoi bolezni serdtsa (Vessel Injury on Myocardial Ischemia), Donetsk: INVKh, 2011.
Kalashnikov, V.Yu., Mitryagina, S.N., Syrkin, A.L., and Poltavskaya, M.G., Ter. Arkh., 2008, vol. 80, no. 4, p. 8.
Bravata, D.M., Gienger, A.L., McDonald, K.M., Sundaram, V., Perez, M.V., Varghese, R., Kapoor, J.R., Ardehali, R., Owens, D.K., and Hlatky, M., A, Ann. Intern. Med., 2007, vol. 147, p. 703.
Shishehbor, M.H., Venkatachalam, S., Sun, Z., Rajeswaran, J., Kapadia, S.R., Bajzer, C., Gornik, H.L., Gray, B.H., Bartholomew, J.R., Clair, D.G., Sabik, J.F., and Blackstone, E.H., J. Am. Coll. Cardiol., 2013, vol. 62, p. 1948.
Dormandy, J.A., Biomed. Eng., 1974, vol. 9, p. 284.
Vizir, V.A. and Berezin, A.E., Ukr. Med. Chasopis, 2008, vol. 68, no. 6, p. 53.
Shlyakhto, E.V., Moiseeva, O.M., Lyasnikova, E.A., Villeval’de, S.V., and Emel’yanov, I.V., Kardiologiya, 2004, vol. 44, no. 4, p. 20.
Krishnan, A., Wilson, A., Sturgeon, J., Siedlecki, C.A., and Vogler, E.A., Biomaterials, 2005, vol. 26, p. 3445.
Kazakov, V.N., Sinyachenko, O.V., Fainerman, V.B., Pison, U., and Miller, R., Dynamic Surface Tensiometry in Medicine, Amsterdam: Elsevier, 2000.
Kazakov, V.N., Knyazevich, V.M., Sinyachenko, O.V., Fainerman, V.B., and Miller, R., in Interfacial Rheology, Miller, R. and Liggieri, L., Eds., Boca Raton: CRC, 2009, p. 519.
Kazakov, V.N., Barkalova, E.L., Levchenko, L.A., Klimenko, T.M., Fainerman, V.B., and Miller, R., Colloids Surf., 2011, vol. 391, p. 190.
Fainerman, V.B., Trukhin, D.V., Zinkovych, I.I., and Miller, R., Adv. Colloid Interface Sci., 2018, vol. 255, p. 34.
Zholob, S.A., Makievski, A.V., Miller, R., and Fainerman, V.B., in Bubble and Drop Interfaces, Miller, R. and Liggieri, L., Eds., Boca Raton: CRC, 2011, p. 39.
Zholob, S.A., Makievski, A.V., Miller, R., and Fainerman, V.B., Adv. Colloid Interface Sci., 2007, vols. 134–135, p. 322.
Lucassen, J. and Hansen, R.S., J. Colloid Interface Sci., 1967, vol. 23, p. 319.
Lucassen, J. and Tempel, M., Chem. Eng. Sci., 1972, vol. 27, p. 1283.
Joos, P., Dynamic Surface Phenomena, Boca Raton: CRC, 1999.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The authors declare that they have no conflict of intere-st.
Additional information
Translated by A. Kirilin
Rights and permissions
About this article

Cite this article
Potapov, V.V., Shramenko, E.K. & Zenin, O.K. Surface Tension and Dilatational Rheology of Blood in Patients Subjected to Cardiological Operations under Conditions of Artificial Circulation. Colloid J 82, 49–53 (2020). https://doi.org/10.1134/S1061933X20010111
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S1061933X20010111