
Abstract—
The aim of this research was to study the dependence of poststroke motor impairments of paretic and non-paretic arm on lesion lateralization, and paresis severity. The influence of lesion lateralization and paresis severity on the recovery of motor functions (MFs) after rehabilitation using a hand exoskeleton controlled by a brain–computer interface was also investigated. The study included 24 patients, 12 with left and 12 with right hemispheric lesions. Each group included six patients with moderate paresis and six patients with severe paresis. Isolated movements in the joints of paretic and non-paretic arms were used as motor tests performed before and after the course of rehabilitation. Joint torque and movement isolation degree were used to assess MFs. It was shown that the joint torques of the non-paretic arm were greater in the case of left hemispheric lesions, characterized by more pronounced asymmetry of joint torques than in right hemispheric lesions. This might be due to a greater imbalance in the activity of hemispheres. The effectiveness of rehabilitation was manifested in: (1) an increase in joint torques in both paretic and non-paretic arms and (2) an increase in the symmetry of biomechanical parameters of paretic and non-paretic arms, potentially indicating the restoration of balance in the hemispheric activity. The biomechanical analysis of isolated movements suggested the pronation–supination movement in a vertical forearm position as a sensitive indicator of MF recovery after stroke.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
It is well-known that motor deficit after stroke involves both paretic [1–3] and non-paretic arms [4, 5]. Cerebrovascular accident is a syndrome of diffuse rather than local brain damage associated with insufficient blood circulation in both hemispheres resulting in the deficiency of regulatory influences in both arms during the premorbid phase. A focal brain lesion causes the impairment of interhemispheric connections, particularly those responsible for bimanual coordination, which affects the state of motor function (MFs) of the non-paretic arm [6, 7]. Consequently, the term “intact arm” is often avoided in studies of arm MFs after stroke, preferring the terms “non-paretic” or “less affected” arm.
Despite the lower expressiveness of motor dysfunction in the non-paretic arm, it can still substantially reduce the patient’s functional activity especially in the presence of severe lesions [8–11], because they force patients to use the non-paretic arm three to six times more often than the paretic one [12]. It was shown that motor deficit of the non-paretic arm does not regress spontaneously over time [13]. Therefore, the non-paretic arm is the main target of rehabilitation in case of severe paresis as it overtakes the main motor load. However, rehabilitation procedures after stroke are mainly aimed at the recovery of MFs of the paretic arm. Traditional methods involving the non-paretic arm in rehabilitation process provide discrepant results. Some studies demonstrated the improvement of MFs in the paretic arm after inclusion of the non-paretic arm in the rehabilitation [14, 15], whereas other studies did not detect any differences in the efficacy of unilateral and bilateral approaches [16].
In this regard, the procedures using a brain–computer interface (BCI) that controls a hand exoskeleton based on kinesthetic motor imagery [17–22] seem adequate for simultaneous rehabilitation of paretic and non-paretic arms . Bimanual motor imagery used in these procedures stimulates neuroplasticity in both hemispheres, promoting the MF progress for each arm and bimanual coordination. Importantly, motor imagery remains the only means of active rehabilitation for severe paresis [23, 24] and/or patients in a chronic stage of stroke reaching a functional plateau in MF recovery [25].
A BCI + exoskeleton procedure is a novel elaboration that is only beginning its introduction into clinical practice [26]. Studies of their efficacy mostly focused on the progress of paretic arm MFs. Non-paretic arm studies compared electrophysiological [27] and hemodynamic [20, 28] activity of contralateral and ipsilateral hemispheres. Biomechanical analysis of non-paretic arm MFs was only performed in individual clinical cases [24, 29, 30]. Non-paretic arm movements can serve as indicators of neuroplastic reorganizations associated with rehabilitation procedures or be the only reliable indicator of successful rehabilitation in case of severe paresis. Thus, biomechanical analysis of non-paretic arm movement provides an objective evaluation of both the severity of motor deficit and the efficacy of motor recovery.
Research on non-paretic arm movements showed that the motor deficit of the non-paretic arm majorly depended on lesion lateralization. The differences involve both the severity of motor deficit and specifics of impaired function. For example, it was found that non-paretic arm motor deficit in patients with left hemispheric damage (LHD) was more pronounced than in patients with right hemispheric damage (RHD) [31] and concerns a motor coordination [13]. The motor deficit of the non-paretic arm in patients with RHD comprises the movement accuracy [13] and maintenance of static limb position [32–34].
The aim of this study was to identify the correlation between non-paretic MFs and lesion lateralization and paresis severity referring to the biomechanical analysis of paretic and non-paretic arm movements before and after rehabilitation using a BCI + hand exoskeleton. Isolated joint movements in non-paretic and paretic arms were used as the motor tests, allowing us to analyze the coordination of postural and motor components of movement organization.
According to our experimental data, the efficacy of kinesthetic motor imagery trainings manifested in: (1) an increase in joint torques in both paretic and non-paretic arms; and (2) an increase in the symmetry of biomechanical parameters of paretic and non-paretic arms, potentially indicating the restoration of balance in the hemispheric activity.
The joint torques of the non-paretic arm were higher in LHD than RHD, suggesting a less pronounced motor deficit of the non-paretic arm in case of LHD. As follows, LHD was associated with stronger asymmetry of joint torques between paretic and non-paretic arms, possibly demonstrating a more prominent imbalance of hemispheric activities, i.e., higher degree of MF impairment, also seen in incoordination of the left non-paretic arm.
Referring to the lateralization theory of movement control [35], it can be proposed that poststroke impairment of posture maintenance of the non-paretic arm is less pronounced than damage of motor coordination mechanisms.
METHODS
The movements of 24 patients were studied, undergoing poststroke rehabilitation using a hand exoskeleton controlled by a BCI based on kinesthetic motor imagery. The rehabilitation procedures were conducted in the Neurology Department of the Vladimirsky Moscow Regional Research and Clinical Institute (Moscow, Russia).
All patients were right-handers. LHD was observed in 12 patients and 12 patients had RHD. Each group included six patients with moderate and six patients with severe paresis. Paresis severity was assessed using the Fugl-Meyer (FM) scale [36] with 66 points being the maximum for the upper extremity. The cut-off score for moderate (m) and severe (s) paresis was set on 29 FM points [37]. The patient characteristics are presented in Table 1.
Rehabilitation Procedure
The rehabilitation procedure was performed according to the protocol elaborated earlier [22]. The patient was situated in an armchair facing the computer screen. Hand exoskeletons operated by electromotors (Androidnaya Tekhnika R&D, Russia) were fixed on both arms. Electroencephalograms (EEGs) were recorded using 32 electrodes located in accordance with the 10–20 system. In order to control the BCI, a patient was supposed to reproduce three states: relaxation (rest) and kinesthetic imagery of finger extension of the left and right hands. Instructions on motor imagery were randomly presented on the screen for 10 s each, separated by a 10-s resting period. An EEG classifier based on the Bayesian method was used to recognize imagined movements [38]. The results of recognition for imagined movements were presented using visual and kinesthetic feedback, particularly, brightness change of gaze fixation marker and passive finger extension executed by the exoskeleton. There were 10 daily procedures including 3 sessions for 10 min each. The rest interval between sessions was 5 min.
Biomechanical Movement Analysis
Non-paretic and paretic arm movements were recorded directly prior to the first procedure and right after the last rehabilitation procedure. The ideology of rehabilitation process consisted in the stimulation of neuroplasticity in the brain cortex. Conditions for such stimulation were created by early verticalization and stimulation of the sole of the foot, promoting the activation of afferent inflow in the brain. Therefore, registration of movement parameters in the upright position was chosen, with arms initially positioned vertically.
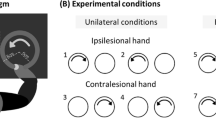
Isolated movements corresponding to each of the degrees of arm freedom were used as the motor tests, constituting a so-called kinematic portrait [29], including abduction–adduction and flexion–extension at the wrist joint; flexion–extension and pronation–supination at the elbow joint; flexion-extension, abduction–adduction, and rotation about the longitudinal axis at the shoulder joint. The patient was supposed to perform each movement three times with the maximal amplitude and comfortable speed. The patient was asked to avoid movements in degrees of freedom outside the instruction. In addition, all test movements were passively performed by the doctor conducting a procedure. Active and passive movements were registered with the help of four sensors of a trakStar electromagnetic system (Ascension Technology Corp., United States) placed on the dorsal hand surface, distal part of forearm, shoulder, and acromion (Fig. 1). The report rate during movement registration was 100 Hz.

Arm movements included in motor tests. (a) Pronation–supination with vertical forearm position (psev); (b) pronation–supination with horizontal forearm position (pseh); (c) elbow flexion-extension (fee).
Afterwards, isolated movements in the elbow joint were analyzed, particularly, pronation–supination in vertical (psev) (Fig. 1a) and horizontal (pseh) (Fig. 1b) forearm positions and flexion–extension (fee) (Fig. 1c). The movement selection was motivated by the following considerations. It is known that the proximal shoulder joint is controlled by both hemispheres, whereas distal joint control is lateralized [39]. Movements in distal wrist joints after stroke are severely limited and often absent in case of severe paresis. Therefore, movements in the elbow joint appear suitable for the analysis of movement features associated with lesion lateralization.
According to the registration of passive movements, individual positions of rotation axes were calculated, whereas active movement registration was used to assess joint angles corresponding to all degrees of freedom of the arm [40]. Joint velocities were calculated using a five-point scheme with weights 1, 2, 4, 2, and 1 [41]. Several examples of time dependences of joint velocities before and after rehabilitation for non-paretic and paretic arms are illustrated in Fig. 2.

Dependences of joint velocities from time during pronation–supination in horizontal forearm position (pseh) performed by a patient with moderate paresis and LHD. Bold line indicates pseh velocity, fine line designates the movement velocities for other degrees of freedom. Velocities of joint movements in the non-paretic arm: (a) before rehabilitation; (b) after rehabilitation. Velocities of joint movements in paretic arm: (c) before rehabilitation; (d) after rehabilitation.
Two parameters were accepted for the estimation of MFs of non-paretic and paretic arms: (1) summary muscle torque responsible for movement in each degree of freedom and (2) the degree of movement isolation characterizing the coordination between degrees of freedom. Standard deviation ∆V of velocity for each degree of freedom was calculated to estimate the muscle torque [42]. This parameter characterizes the changes in angular velocity during movement and can be used for evaluation of angular acceleration, and therefore evaluation of summary muscle torque in the joint. The movement isolation degree was calculated as a ratio of standard deviations of movement velocity included in the instruction to the sum of standard deviations of movement velocities for all degrees of freedom.
One patient with LHD and four patients with RHD had a severe paresis and could not perform pronation–supination, holding the forearm in a horizontal position. Therefore, further on ∆Vpseh joint torque and pseh isolation degree were studied for patients with moderate paresis only.
A relative change of biomechanical parameters was applied to describe changes in MFs induced by a BCI + exoskeleton, i.e., ratio of their difference after and before the rehabilitation procedures to the value before the procedures. For example, changes in joint torques were calculated according to the formula: (ΔV2 – ΔV1)/ΔV1 × 100%, where 1 and 2 indicated the values of joint torques before and after rehabilitation procedures.
Statistical Analysis
The Wilcoxon test was used to detect differences between the biomechanical parameters and Spearman’s correlation was used to identify correlations.
RESULTS
Joint Torques
Mean values of joint torques in the non-paretic arm before the procedures were higher in LHD than in RHD both for moderate and severe paresis (Fig. 3). Significant difference of LHD from RHD was seen only for pseh in moderate paresis (p = 0.006) and psev in severe paresis (p = 0.04) (white boxes on the left and right, Fig. 3).

Assessment of muscle torques in paretic (dashed boxes) and non-paretic (white boxes) arm joints before rehabilitation. Mean values (dots inside boxes), standard errors (boxes), and mean-square deviation (whiskers) are presented. Data of patients with LDH are illustrated on the left, whereas RHD patients are illustrated on the right. (a) Patients with moderate paresis, (b) patients with severe paresis. Asterisk designates significant differences in paretic and non-paretic arm parameters.
On the contrary, joint torques were averagely higher for paretic arm with moderate paresis in case of RHD, though non-significantly (dashed boxes, Fig. 3a). Mean values of psev and fee joint torques were identical for LHD and RHD (dashed boxes, Fig. 3b).
Mean values of joint torques for all test movements were higher for the non-paretic arm than for the paretic one both for LHD and RHD and moderate or severe paresis (Fig. 3). Joint torques before the procedures of patients with LHD were significantly higher for non-paretic arms than for paretic arms in all studied joints. The difference was observed both in moderate—pseh (p = 0.03), psev (p = 0.03), and fee (p = 0.03) and severe paresis—psev (p = 0.03) and fee (p = 0.03).
Patients with RHD were characterized by significant difference (p = 0.04) only for psev in case of severe paresis (Fig. 3).
Isolation Degree of Joint Movement
The mean values of movement isolation in the non-paretic arm before the procedures were higher for LHD than for RHD (Fig. 4). This was true both for moderate and severe paresis, except for fee movement in case of moderate paresis isolation of which was averagely higher for RHD (Fig. 4). However, this difference between LHD and RHD was non-significant.

Movement isolation degree in joints of paretic (dashed boxes) and non-paretic (white boxes) arms before rehabilitation. For legend see Fig. 3.
The degree of movement isolation for the paretic arm was averagely higher in LHD only for pseh and psev movements of patients with moderate paresis (Fig. 4). As for other joint movements, namely fee for moderate paresis and psev and fee for severe paresis, the degree of isolation was on average higher for RHD, though non-significantly (Fig. 4).
The differences were significant only in the case of severe paresis in psev (p = 0.03) and fee (p = 0.03) of patients with LHD.
Low mean values of movement isolation degree varying from 0.4 to 0.6 in the paretic arm and 0.5 to 0.6 in the non-paretic arm were related to the correlation between the joint torques during instruction and summary joint torques outside instruction. The largest correlations were seen for psev in the paretic arm with severe paresis (R = 0.87, p = 0.0002) and the smallest correlation was seen in fee of the non-paretic arm with moderate paresis (R = 0.61, p = 0.03).
Differences of Biomechanical Parameters in Cases of Moderate and Severe Paresis
The data on significance of differences between the biomechanical parameters in cases of moderate and severe paresis are presented in Table 2. The differences between moderate and severe paresis were significant for psev joint torque and isolation degree of the paretic arm both for LHD and RHD. No significant differences were detected between moderate and severe paresis for fee joint torques in the paretic arm nor for LHD neither for RHD. As for fee isolation, moderate and severe paresis differed significantly only for LHD. For the non-paretic arm the difference between moderate and severe paresis was significant only for the fee degree of isolation in LHD patients.
Changes in MF of Non-Paretic and Paretic Arms after BCI + Exoskeleton Procedures
The joint torques of both paretic and non-paretic arms increased after the rehabilitation procedures (Fig. 5). The only exception was the pseh torque in the non-paretic arm with moderate paresis and left-hemispheric lesion (LHDm) that slightly reduced after the procedures. MF progress of the paretic arm was the most prominent in psev in case of severe paresis, particularly, the joint torque associated with this movement augmented by 59% for LHD and 67% for RHD.

Relative changes in fee, psev, and pseh joint torques after rehabilitation. Dashed columns illustrate mean relative changes in joint torques of paretic arm; white columns represent these parameters for non-paretic arm in patients with moderate paresis and LHD (LHDm), moderate paresis and RHD (RHDm), severe paresis and LHD (LHDs), and severe paresis and RHD (RHDs).
The joint torques of the paretic arm in a patient with LHD increased more pronouncedly than in the non-paretic arm in all cases except of fee in case of severe paresis (Fig. 5). However, significant difference between the joint torques of non-paretic and paretic arms maintained after the rehabilitation procedures.
In the majority of cases of RHD, the joint torques of the non-paretic arm increased more than in the paretic arm (Fig. 5). No significant differences were found between the joint torques of non-paretic and paretic arms either before or after the procedures.
The progress of fee joint torque of the non-paretic arm was more expressed than in the paretic arm in case of severe paresis (LHDs and RHDs) and for fee and psev joint torques in case of moderate paresis and right-hemispheric lesion (RHDm).
Significant correlation between changes in pseh (R = 0.68, p = 0.015) and psev (R = 0.61, p = 0.03) joint torques of non-paretic and paretic arms was demonstrated only in case of moderate paresis.
The progress in the isolation degree of joint movements was not so pronounced after the procedures as the joint torques both in paretic and non-paretic arms (Fig. 6). The isolation degree of joint movements increased by more than 20% in paretic arms of patients with RHD only, specifically for psev in case of severe and moderate paresis and for pseh in case of moderate paresis (Fig. 6).

Changes in fee, psev, and pseh isolation degrees. Dashed columns illustrate changes in movement isolation degrees of paretic arm; white columns represent these parameters for non-paretic arm. Mean values for patients with moderate paresis and LHD (LHDm), moderate paresis and RHD (RHDm), severe paresis and LHD (LHDs), and severe paresis and RHD (RHDs) are presented.
Movement isolation deteriorated in certain cases after the procedures (negative values in Fig. 6) both in paretic and non-paretic arms, although such deterioration was not substantial (less than 10%), except for the 22% reduction of psev isolation degree in case of severe paresis of RHD patients.
DISCUSSION
Motor deficit in an ipsilateral non-paretic arm in central paresis is demonstrated by neurophysiological [6, 7], anatomical [43, 44], clinical [15, 31], and biomechanical [13] studies.
Numerous studies showed that the type of movement disorders in the non-paretic arm depended on the lesion lateralization and paresis severity. In these studies the performed movements were analyzed and therefore those results majorly affected the choice of motor tests and means of MF assessment.
From this perspective, the studies could be divided into two groups: (1) studies [15, 31, 45] using everyday movements from Jebsen–Taylor Hand Function Test [46] as motor tests and the performance time to estimate MF; (2) studies [13, 35, 45, 47–50] using arm movements to static targets in the external space as motor tests and biomechanical parameters of arm working point trajectory to assess MFs.
In both cases the motor tests are substantially lateralized: the dominant arm is more involved in the everyday movements of the Jebsen–Taylor Hand Function Test, whereas targeted movements are more coordinated and accurate when performed by the dominant arm [51]. Regarding the movement assessment, the performance time in the Jebsen–Taylor Hand Function Test characterizes the coordination component of motor organization [52, 53]. Approximation of working point trajectory to a line characterizes interjoint coordination during targeted movement performance [54]. The postural component is evaluated by the accuracy of posture maintenance for the working point when reaching a goal.
All of the abovementioned parameters describe the resulting effect from coordinated movements in arm joints. However, damage to different mechanisms of joint control can be associated with the same level of functional deficit. The studies of poststroke joint movement impairment mostly refer to the coordination between shoulder and elbow joints [2, 33, 55]. In the present article the impairments of isolated movements at the elbow joint were investigated, i.e., flexion–extension and pronation–supination in vertical and horizontal forearm positions.
Such motor tests have been chosen referring to the following ideas: (1) impaired ability to perform isolated movement in a joint is one of the crucial signs of motor deficit associated with stroke: it was shown that this ability affects targeted movement coordination more than spasticity or sensation deficit [56]; (2) performance of isolated movement implies the immobilization of all joints apart from the one involved in the instruction, which requires the interjoint coordination including both motor and postural components, essential for determining the differences between LHD and RHD; and (3) unlike target-specific and everyday movements, isolated movements have no functional significance, hence no association with the arm dominance, which is also important to identify lesion lateralization-related differences.
Similar to the results of previous biomechanical studies, our data suggested less pronounced motor deficit in the non-paretic arm compared to the paretic one (Figs. 3 and 4). However, the expressiveness of difference of motor deficit in non-paretic and paretic arms depending on lesion lateralization has not been studied until now. According to our data, the differences between joint torques in non-paretic and paretic arms were substantially more pronounced in LHD patients than in RHD ones (Fig. 3).
Joint torque asymmetry in non-paretic and paretic arms can ensue from the imbalance of hemispheric activity and enhancement of functional connections in the intact hemisphere [7], as well as from an increase of interhemispheric inhibitory projections from the intact to damaged hemispheres [6]. Earlier such recovery from BCI + exoskeleton procedures was demonstrated by the example of hemodynamic activity in a patient with severe paresis in a chronic stage of stroke [28]. Joint torque asymmetry predominating in LHD might indicate a more expressed imbalance in hemispheric activity and resulting higher severity of motor deficit in LHD. In particular, this can be expressed in the incoordination of the left non-paretic arm [13].
Referring to our data, the joint torques in the non-paretic arm were larger in LHD than in RHD (Fig. 3). The possible reason for that observation is higher activity of left dominant hemisphere during left non-paretic arm operation compared to the activity of right non-dominant hemisphere when operating with the right non-paretic arm [57, 58]. Probably, due to the lesser severity of impairment of the muscle strength in the non-paretic arm in case of LHD, the left non-paretic arm is more involved in the everyday activity and therefore its motor deficit correlates with the functional independence of the patient, unlike right non-paretic arm deficit in case of RHD [45].
In contrast to the joint torques, the isolation degree of joint movements of the non-paretic arm was similar in patients with LHD and RHD (Fig. 4), associated with strong positive correlation between the joint torques within the instruction and summary torques of other joints. These results conformed to the shared command hypothesis regulating the postural adjustments and movements [59, 60]. Isolated movement was closely related to postural adjustments impaired with stroke [61, 62]. This damage was associated to the delay in postural adjustments compared to norm. It was shown that those delays were longer in the non-dominant arm than in the dominant one [63], explaining poorer postural stability (larger summary joint torques outside the instruction) in the non-paretic arm in case of LHD. Along with the mistakes of sensorimotor modifications, postural setting delay can contribute to the incoordination of non-dominant arm movements. More severe incoordination of targeted [13] and everyday movements from the Jebsen–Taylor Hand Function Test [31] in LHD patients could be associated with elbow overextension provoked by postural adjustment delay [63].
Several data demonstrated the exacerbation of motor deficit in the non-paretic arm with growing severity of paresis, especially in LHD [13, 31]. No such difference was seen in the vast majority of our parameters (Table 2). The only exception was the significant difference in fee isolation degree between moderate and severe paresis in case of LHD. It should be emphasized that even in the paretic arm significant differences in joint torques and isolation degree were seen only in psev (Table 2). Motor deficit was evaluated in studies [13, 30] using the evaluation of time to perform everyday habitual movements. Time to perform these movements depended both on the coordination of joint movements and postural adjustments, whereas isolated movement performance was mainly determined by postural adjustments. It could be proposed that the difference of our work from the previous results of other authors [13, 31] was due to the more prominent coordination impairment with the aggravation of paresis severity than the regulation of postural settings. This can be related to the organization of postural control on a lower subcortical level than the control over multijoint extremity coordination [64, 65]. Patients included in the analysis had subcortical and cortical–subcortical lesions (Table 1), though performed the test movements in vertical position, suggesting the light dysfunction of postural control, thus not being the pivotal sign of focal lesion [66].
The difference between moderate and severe paresis was detected not only for the parameters of isolated movements with the non-paretic arm, but also for their ratios to the movement parameters of the paretic hand. The movement parameters of non-paretic and paretic arms with moderate paresis differed substantially less than in arms with severe paresis (Figs. 3 and 4). The mean values of parameter differences were greater in case of severe paresis than in moderate paresis both for LHD and RHD, although the difference was significant only in LHD (Table 2). This result supports the role of symmetry in biomechanical parameters of non-paretic and paretic arms as an indicator of balance between hemispheric activities, which in turn indicates their normal functioning [67].
MF Progress after BCI + Exoskeleton Procedures
It was shown that BCI + exoskeleton procedures promoted the progression of MFs in paretic arm [17–22], though the influence of such procedures on the MFs of the non-paretic arm was not specifically investigated. On the other hand, BCI + exoskeleton procedures were aimed at stimulation of neuroplasticity in both hemispheres, which should affect the MF condition both in the paretic and non-paretic arms. As a matter of fact, the joint torques augmented after the procedures both in the paretic and non-paretic arms (Fig. 5). According to the patients’ reports after rehabilitation procedures, motor imagery was strongly associated with a feeling of resistance to the imagined movement. Possibly the efficacy of muscle strength recovery is related to these patients’ feelings.
As opposed to the joint torques, the increase in movement isolation degree was mainly seen in the paretic arm and insignificantly in the non-paretic arm , with its decrease detected in some cases. Joint isolation degree was calculated as the ratio of joint torque during instruction to summary joint torques outside the instruction. Taking into account the growth of joint torques after the procedures, the absence of movement isolation increment suggested the concomitant increase in the joint torques outside the instruction. Their expected reduction, meaning the stabilization of joints outside the instructions, was associated with coactivation of antagonist muscles that apparently recovered less successfully during the procedures than muscle strengths.
Regarding the moderate paresis, relative changes in joint torques of non-paretic and paretic arms significantly correlated with each other in pseh and psev, naturally resulting from simultaneous training of activity of both hemispheres underlying BCI + hand exoskeleton procedures. The absence of correlation between fee joint torques and joint torques in severe paresis was possible due to the insufficient intensity of rehabilitation course, e.g., its short duration.
As for LHD, the increase in joint torques of the paretic arm was chiefly larger than in the non-paretic one (Fig. 5), resulting in a more symmetrical joint torque pattern. This might demonstrate the procedure efficacy in promoting the recovery of hemispheric activity balance that was impaired after stroke. In contrast, in the majority of RHD cases the joint torques of the non-paretic arm augmented after the procedures more prominently than of the paretic one (Fig. 5). Both before and after the procedures, no significant differences were found between the joint torques of non-paretic and paretic arms . To summarize, kinesthetic motor imagery trainings showed benefits for patients with LHD and were responsible not only for growth of joint torques , but also the reduction of joint torque asymmetry between non-paretic and paretic arms . The influence of activity ratio of right and left hemispheres on the efficacy of MF recovery is still a subject of discussion [68], however, the recovery of normal activity balance can be considered a standard indicator of rehabilitation efficiency [67].
The studies applying BCI for stroke rehabilitation found that MF improvement in case of severe paresis correlated with the increase in primary motor cortex activity of both intact [25, 69, 70] and damaged [20, 71] hemispheres. It is still disputable the activity of which hemisphere promotes the initiation of neuroplasticity and MF recovery. The answer to this question determines every specific design of BCI procedures. For instance, it was offered in [70] to use BCI stimulating the activity of the intact hemisphere to activate the paretic hand exoskeleton. Nevertheless, active bilateral stimulation seems more adequate since it facilitates a recovery of activity balance in both hemispheres [28], successfully driving the exoskeletons of both paretic and non-paretic arms.
The biomechanical movement parameters objectively reflected MF changes in paretic and non-paretic arms resulting from the rehabilitation procedures, particularly, from kinesthetic motor imagery trainings [24, 29, 30, 42]. The results of analysis given above showed that pronation–supination of the paretic arm in a vertical forearm position benefited from the procedures the most in case of severe paresis, particularly, both joint torque (Fig. 5) and isolation degree (Fig. 6) of this movement substantially increased. These results might be associated with the fact that such movement did not require: (1) additional muscular effort to balance gravity and (2) the coordination between several muscles with similar functions as it involved only a pair of independent antagonists (m. pronator teres and m. supinator). Because of these reasons pronation–supination seems the most comprehensive for the assessment of rehabilitation effectiveness. However, it is rarely included in biomechanical analysis [24, 42]. Usually, the analysis of joint movements is limited to flexion–extension at elbow and shoulder joints [2, 33, 55].
CONCLUSIONS
Ideomotor trainings of kinesthetic motor imagery for controlling a limb exoskeleton are principally aimed at activating both hemispheres. Their efficacy infers the stimulation of neuroplasticity and manifests with (1) augmentation of muscle torques in joints of both the non-paretic and paretic arms and (2) increase in symmetry of biomechanical parameters of the non-paretic and paretic arms, probably indicating the recovery of balance in activities of intact and damaged hemispheres.
The joint torques of the non-paretic arm were larger in the case of LHD than in RHD, suggesting less pronounced muscle deficit in the non-paretic arm after LHD. As a result, LHD was associated with larger asymmetry of joint torques of non-paretic and paretic arms, potentially representing more severe imbalance in hemispheric activity, i.e., more severe motor deficit seen in the incoordination of the left non-paretic arm.
Comparison with the results within the lateralization theory of movement control [35] allowed proposing that poststroke impairment of postural maintaining mechanisms was less pronounced in non-paretic arm than the impairment of motor coordination mechanisms.
The biomechanical analysis of isolated joint movements allowed presuming that pronation-supination in vertical forearm position was a sensitive indicator of MF recovery after stroke.
REFERENCES
Given, J.D., Dewald, J.P., and Rymer, W.Z., Joint dependent passive stiffness in paretic and contralateral limbs of spastic patients with hemiparetic stroke, J. Neurol. Neurosurg. Psychiatry, 1995, vol. 59, no. 3, p. 271.
Levin, M.F., Interjoint coordination during pointing movements is disrupted in spastic hemiparesis, Brain, 1996, vol. 119, p. 281.
Beer, R.F., Dewald, J.P., Dawson, M.L., and Rymer, W.Z., Target-dependent differences between free and constrained arm movements in chronic hemiparesis, Exp. Brain Res., 1989, vol. 156, no. 4, p. 458.
Haaland, K.Y. and Harrington, D.L., Hemispheric asymmetry of movement, Curr. Opin. Neurobiol., 1996, vol. 6, no. 6, p. 796.
Sunderland, A., Recovery of ipsilateral dexterity after stroke, Stroke, 2000, vol. 31, no. 2, p. 430.
Duque, J., Hummel, F., and Celnik, P., et al. Transcallosal inhibition in chronic subcortical stroke, NeuroImage, 2005, vol. 28, no. 4, p. 940.
Gerloff, C., Bushara, K., Sailer, A., et al., Multimodal imaging of brain reorganization in motor areas of the contralesional hemisphere of well recovered patients after capsular stroke, Brain, 2006, vol. 129, p. 791.
Desrosiers, J., Bourbonnais, D., Bravo, G., et al., Performance of the 'unaffected' upper extremity of elderly stroke patients, Stroke, 1996, vol. 27, no. 9, p. 1564.
Lang, C.E., Wagner, J.M., Edwards, D.F., and Dromerick, A.W., Upper extremity use in people with hemiparesis in the first few weeks after stroke, J. Neurol. Phys. Ther., 2007, vol. 31, no. 2, p. 56.
Wetter, S., Poole, J.L., and Haaland, K.Y., Functional implications of ipsilesional motor deficits after unilateral stroke, Arch. Phys. Med. Rehabil., 2007, vol. 86, no. 4, p. 776.
Rinehart, J.K., Singleton, R.D., Adair, J.C., et al., Arm use after left or right hemiparesis is influenced by hand preference, Stroke, 2009, vol. 40, no. 2, p. 545.
Vega-González, A. and Granat, M.H., Continuous monitoring of upper-limb activity in a free-living environment, Arch. Phys. Med. Rehabil., 2005, vol. 86, no. 3, p. 541.
Sainburg, R.L., Maenza, C., Winstein, C., and Good, D., Motor lateralization provides a foundation for predicting and treating non-paretic arm motor deficits in stroke, Adv. Exp. Med. Biol., 2016, vol. 957, p. 257.
Pandian, S., Arya, K.N., and Kumar, D., Effect of motor training involving the less-affected side (MTLA) in post-stroke subjects: a pilot randomized controlled trial, Top. Stroke Rehabil., 2015, vol. 22, no. 5, p. 357.
Maenza, C., Wagstaff, D.A., Varghese, R., et al., Remedial training of the less-impaired arm in chronic stroke survivors with moderate to severe upper-extremity paresis improves functional independence: a pilot study, Front. Hum. Neurosci., 2021, vol. 15, p. 645714.
van Delden, A.E.Q., Peper, C.E., Beek, P.J., and Kwakkel, G., Unilateral versus bilateral upper limb exercise therapy after stroke: a systematic review, J. Rehabil. Med., 2012, vol. 44, no. 2, p. 106.
Ang, K.K., Guan, C., Chua, K.S.G., et al., A large clinical study on the ability of stroke patients to use an EEG-based motor imagery brain-computer interface, Clin. EEG Neurosci., 2011, vol. 42, no. 4, p. 253.
Ang, K.K., Guan, C., Phua, K.S., et al., Brain-computer interface-based robotic end effector system for wrist and hand rehabilitation: results of a three-armed randomized controlled trial for chronic stroke, Front. Neuroeng., 2014, vol. 7, p. 30.
Ang, K.K., Chua, K.S.G., Phua, K.S., et al., A randomized controlled trial of EEG-based motor imagery brain-computer interface robotic rehabilitation for stroke, Clin. EEG Neurosci., 2015, vol. 46, no. 4, p. 310.
Ramos-Murguialday, A., Broetz, D., Rea, M., et al., Brain—machine interface in chronic stroke rehabilitation: a controlled study, Ann. Neurol., 2013, vol. 74, no. 1, p. 100.
Ono, T., Shindo, K., Kawashima, K., et al., Brain—computer interface with somatosensory feedback improves functional recovery from severe hemiplegia due to chronic stroke, Front. Neuroeng., 2014, vol. 7, p. 19.
Frolov, A.A., Mokienko, O., Lyukmanov, R., et al., Post-stroke rehabilitation training with a motor-imagery based brain—computer interface (BCI)-controlled hand exoskeleton: a randomized controlled multicenter trial, Front. Neurosci., 2017, vol. 11, p. 400.
Buch, E., Weber, C., Cohen, L.G., et al., Think to move: a neuromagnetic brain—computer interface (BCI) system for chronic stroke, Stroke, 2008, vol. 39, no. 3, p. 910.
Biryukova, E.V., Pavlova, O.G., Kurganskaya, M.E., et al., Recovery of the motor function of the arm with the aid of a hand exoskeleton controlled by a brain—computer interface in a patient with an extensive brain lesion, Hum. Physiol., 2016, vol. 42, no. 1, p. 13.
Young, B.M., Nigogosyan, Z., Walton, L.M., et al., Changes in functional brain organization and behavioral correlations after rehabilitative therapy using a brain—computer interface, Front. Neuroeng., 2014, vol. 7, p. 26.
Cervera, M.A., Soekadar, S.R., Ushiba, J., et al., Brain—computer interfaces for post-stroke motor rehabilitation: a metaanalysis, Ann. Clin. Transl. Neurol., 2018, vol. 5, no. 5, p. 651.
Kotov, S.V., Romanova, M.V., Kondur, A.A., et al., Reorganization of bioelectrical activity in the neocortex after stroke by rehabilitation using a brain—computer interface controlling a wrist exoskeleton, Neurosci. Behav. Physiol., 2020, vol. 50, no. 9, p. 1146. https://doi.org/10.1007/s11055-020-01017-7
Frolov, A.A., Bobrov, P.D., Biryukova, E.V., et al., Electrical, hemodynamic and motor activities in post-stroke rehabilitation provided by the hand exoskeleton under control of brain—computer interface: clinical case study, Front. Neurol., 2018, vol. 9, p. 1135.
Kondur, A.A., Biryukova, E.V., Kotov, S.V., et al., The kinematic portrait of a patient as an objective indicator of motor function in the process of neurorehabilitation with hand exoskeleton controlled by the brain—computer interface, Uch. Zap. S.-Peterb. Gos. Med. Univ. im. I, P. Pavlova, 2016, vol. 23, no. 3, p. 28.
Dzhalagoniya, I., Biryukova, E., Bushkova, Y., et al., Biomechanical assessment of Fugl-Meyer score: the case of one post stroke patient who has undergone the rehabilitation using hand exoskeleton controlled by the brain—computer interface, Int. J. Phys. Med. Rehabil., 2018, vol. 6, no. 3, p. 2.
Maenza, C., Good, D.C., Winstein, C.J., et al., Functional deficits in the less-impaired arm of stroke survivors depend on hemisphere of damage and extent of paretic arm impairment, Neurorehabil. Neural Rep., 2020, vol. 34, no. 1, p. 39.
Schaefer, S.Y., Haaland, K.Y., and Sainburg, R.L., Ipsilesional motor deficits following stroke reflect hemispheric specializations for movement control, Brain, 2007, vol. 130, p. 2146.
Schaefer, S.Y., Haaland, K.Y., and Sainburg, R.L., Hemispheric specialization and functional impact of ipsilesional deficits in movement coordination and accuracy, Neuropsychologia, 2009, vol. 47, no. 13, p. 2953.
Mani, S., Mutha, P.K., Przybyla, A., et al., Contralesional motor deficits after unilateral stroke reflect hemisphere-specific control mechanisms, Brain, 2013, vol. 136, p. 1288.
Mutha, P.K., Haaland, K.Y., and Sainburg, R.L., Rethinking motor lateralization: specialized but complementary mechanisms for motor control of each arm, PLoS One, 2013, vol. 8, no. 3. e58582.
Fugl-Meyer, A.R., Jääskö, L., Leyman, I., et al., The post-stroke hemiplegic patient: 1. A method for evaluation of physical performance, Scand. J. Rehabil. Med., 1975, vol. 7, no. 1, p. 13.
Woytowicz, E.J., Rietschel, J., Goodman, R.N., et al., Determining levels of upper extremity movement impairment by applying a cluster analysis to the Fugl-Meyer assessment of the upper extremity in chronic stroke, Arch. Phys. Med. Rehabil., 2017, vol. 98, no. 3, p. 456.
Bobrov, P.D., Korshakov, A.V., Roshchin, V.Yu., and Frolov, A.A., Bayesian classifier for brain—computer interface based on mental representation of movements, Zh. Vyssh. Nerv. Deyat. im I. P. Pavlova, 2012, vol. 62, no. 1, p. 89.
Lemon, R., Descending pathways in motor control, Annu. Rev. Neurosci., 2008, vol. 31, p. 195.
Biryukova, E.V., Roby-Brami, A., Frolov, A.A., and Mokhtari, M., Kinematics of human arm reconstructed from spatial tracking system recordings, J. Biomech., 2000, vol. 33, no. 8, p. 985.
Hamming, R.W., Numerical Methods for Scientists and Engineers, New York: McGrow-Hill, 1962.
Kondur, A.A., Biryukova, E.V., and Frolov, A.A., Rehabilitation of the arm motor function in poststroke patients with an exoskeleton-controlling brain—computer interface: effect of repeated hospitalizations, Hum. Physiol., 2020, vol. 46, no. 3, p. 321. https://doi.org/10.1134/S036211972003007X
Bradnam, L.V., Stinear, C.M., and Byblow, W.D., Ipsilateral motor pathways after stroke: implications for non-invasive brain stimulation, Front. Hum. Neurosci., 2013, vol. 7, p. 184.
Noskin, O., Krakauer, J.W., Lazar, R.M., et al., Ipsilateral motor dysfunction from unilateral stroke: implications for the functional neuroanatomy of hemiparesis, J. Neurol. Neurosurg. Psychiatry, 2008, vol. 79, no. 4, p. 401.
Jayasinghe, S.A.L., Good, D., Wagstaff, D.A., et al., Motor deficits in the ipsilesional arm of severely paretic stroke survivors correlate with functional independence in left, but not right hemisphere damage, Front. Hum. Neurosci., 2020, vol. 14, p. 599220.
Jebsen, R.H., Taylor, N., Trieschmann, R.B., et al., An objective and standardized test of hand function, Arch. Phys. Med. Rehab., 1969, vol. 50, no. 6, p. 311.
Haaland, K.Y., Prestopnik, J.L., Knight, R.T., and Lee, R.R., Hemispheric asymmetries for kinematic and positional aspects of reaching, Brain, 2004, vol. 127, p. 1145.
Winstein, C.J. and Pohl, P.S., Effects of unilateral brain damage on the control of goal-directed hand movements, Exp. Brain Res., 1995, vol. 105, no. 1, p. 163.
Mutha, P.K., Haaland, K.Y., and Sainburg, R.L., The effects of brain lateralization on motor control and adaptation, J. Mot. Behav., 2012, vol. 44, no. 6, p. 455.
Schaefer, S.Y., Mutha, P.K., Haaland, K.Y., and Sainburg, R.L., Hemispheric specialization for movement control produces dissociable differences in online corrections after stroke, Cereb. Cortex, 2012, vol. 22, no. 6, p. 1407.
Sainburg, R.L. and Kalakanis, D., Differences in control of limb dynamics during dominant and nondominant arm reaching, J. Neurophysiol., 2000, vol. 83, no. 5, p. 2661.
Johansson, G.M., Grip, H., Levin, M.F., and Häger, C.K., The added value of kinematic evaluation of the timed finger-to-nose test in persons post-stroke, J. NeuroEng. Rehab., 2017, vol. 14, no. 1, p. 11.
Rodrigues, M.R.M., Slimovitch, M., Chilingaryan, G., and Levin, M.F., Does the finger-to-nose test measure upper limb coordination in chronic stroke?, J. NeuroEng. Rehab. 2017, vol. 14, no. 1, p. 6.
Flash, T. and Hogan, N., The coordination of arm movements: an experimentally confirmed mathematical model, J. Neurosci., 1985, vol. 5, no. 7, p. 1688.
Mutha, P.K., Sainburg, R.L., and Haaland, K.Y., Coordination deficits in ideomotor apraxia during visually targeted reaching reflect impaired visuomotor transformations, Neuropsychologia, 2010, vol. 48, no. 13, p. 3855.
Zackowski, K.M., Dromerick, A.W., Sahrmann, S.A., et al., How do strength, sensation, spasticity and joint individuation relate to the reaching deficits of people with chronic hemiparesis? Brain, 2004, vol. 127, no. 5, p. 1035.
Kawashima, R., Yamada, K., Kinomura, S., et al., Regional cerebral blood flow changes of cortical motor areas and prefrontal areas in humans related to ipsilateral and contralateral hand movement, Brain Res., 1993, vol. 623, no. 1, p. 33.
Kim, S.G., Ashe, J., Hendrich, K., et al., Functional magnetic resonance imaging of motor cortex: hemispheric asymmetry and handedness, Science, 1993, vol. 261, no. 5121, p. 615.
Cavallari, P., Bolzoni, F., Bruttini, C., and Esposti, R., The organization and control of intra-limb anticipatory postural adjustments and their role in movement performance, Front. Hum. Neurosci., 2016, vol. 10, p. 525.
Bruttini, C., Esposti, R., Bolzoni, F., and Cavallari, P., Ischemic block of the forearm abolishes finger movements but not their associated anticipatory postural adjustments, Exp. Brain Res., 2014, vol. 232, no. 6, p. 1739.
Dickstein, R., Shefi, S., Marcovitz, E., and Villa, Y., Anticipatory postural adjustment in selected trunk muscles in post stroke hemiparetic patients, Arch. Phys. Med. Rehabil., 2004, vol. 85, no. 2, p. 261.
Yang, C.-L., Creath, R.A., Magder, L., et al., Impaired posture, movement preparation, and execution during both paretic and nonparetic reaching following stroke, J. Neurophysiol., 2019, vol. 121, no. 4, p. 1465.
Bruttini, C., Esposti, R., Bolzoni, F., and Cavallari, P., Higher precision in pointing movements of the preferred vs. non-preferred hand is associated with an earlier occurrence of anticipatory postural adjustments, Front. Hum. Neurosci., 2016, vol. 10, p. 365.
Massion, J., Ioffe, M., Schmitz, C., et al., Acquisition of anticipatory postural adjustments in a bimanual load-lifting task: normal and pathological aspects, Exp. Brain Res., 1999, vol. 128, nos. 1—2, p. 229.
Viallet, F., Massion, J., Massarino, R., and Khalil, R., Coordination between posture and movement in a bimanual load lifting task: putative role of a medial frontal region including the supplementary motor area, Exp. Brain Res., 1992, vol. 88, no. 3, p. 674.
Hsieh, C.L., Sheu, C.F., Hsueh, I.P., and Wang, C.H., Trunk control as an early predictor of comprehensive activities of daily living function in stroke patients, Stroke, 2002, vol. 33, no. 11, p. 2626.
Dodd, K.C., Nair, V.A., and Prabhakaran, V., Role of the contralesional vs. ipsilesional hemisphere in stroke recovery, Front. Hum. Neurosci., 2017, vol. 11, p. 469.
Hoyer, E.H. and Celnik, P.A., Understanding and enhancing motor recovery after stroke using transcranial magnetic stimulation, Restor. Neurol. Neurosci., 2011, vol. 29, no. 6, p. 395.
Song, J., Young, B. M., Nigogosyan, Z., et al., Characterizing relationships of DTI, fMRI, and motor recovery in stroke rehabilitation utilizing brain—computer interface technology, Front. Neuroeng., 2014, vol. 7, p. 31.
Bundy, D.T., Souders, L., Baranyai, K., et al., Contralesional brain—computer interface control of a powered exoskeleton for motor recovery in chronic stroke survivors, Stroke, 2017, vol. 48, no. 7, p. 1908.
Pichiorri, F., Morone, G., Petti, M., et al., Brain—computer interface boosts motor imagery practice during stroke recovery, Ann. Neurol., 2015, vol. 77, no. 5, p. 851.
ACKNOWLEDGMENTS
The authors are grateful to Prof. Jean Massion for discussing the study results.
Funding
The study was financially supported by the Russian Foundation for Basic Research (grant nos. 19-015-00192 and 20-015-00370) and Ministry of Education and Science of the Russian Federation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest. The authors declare that they do not have a conflict of interest.
Statement of compliance with standards of research involving humans as subjects. All procedures performed in studies involving human participants were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments and approved by the local Ethics Committee of Vladimirsky Moscow Regional Research and Clinical Institute (protocol no. 9, October 2, 2014). Informed consent was obtained from all individual participants involved in the study.
Additional information
Translated by E. Sherstyuk
Rights and permissions
About this article

Cite this article
Biryukova, E.V., Kondur, A.A., Kotov, S.V. et al. Paretic and Non-Paretic Arm Motor Deficit and Recovery as a Function of Lesion Lateralization and Paresis Severity: A Biomechanical Study. Hum Physiol 48, 667–679 (2022). https://doi.org/10.1134/S0362119722700116
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0362119722700116