
Abstract
The spread of the COVID-19 pandemic has shown great heterogeneity between countries that merits investigation. There is a need to better highlight the variability in the pandemic trajectories in different geographic areas. By using openly available data from ‘GitHub’ COVID-19 dataset for Europe and from the official dataset of France for the period 2020 to 2021, I present the three COVID-19 waves in France and Europe in maps. The epidemic trends across areas display different evolutions for different time periods. National and European public health authorities will be able to improve allocation of resources for more effective public health measures based on geo-epidemiological analyses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Key messages
-
The spread of the COVID-19 pandemic showed heterogeneity between and across countries
-
National and European public health authorities should improve allocation of resources according to this heterogeneity
Introduction
The spread of the COVID-19 pandemic has shown great heterogeneity between regions in countries, including in France and in Europe [1]. Geographical differences in incidence, infection, and mortality rates have been correlated with arrival time of the COVID-19 virus, population age structure, socio-economic development and population density, the health insurance system, climatic and meteorological determinants, and anti-contagion policies and health practices [2].
Geo-epidemiological analyses of epidemics is an approach by which one compares data of epidemics across different geographical regions and populations, preferably at high geographical resolution, and in the process helps to identify environmental and socio-economic factors that govern the detected patterns and shape prevention, resource-planning, policy making, funding, healthcare considerations, and therapeutic intervention [3, 4]. Geo-epidemiological analyses allow comparison of epidemiological data of epidemics through a geographical and population prism and can improve the local and global health policies [5,6,7]. Local geo-referenced temporal data could help to identify the changing dynamic in the spread of epidemics [8,9,10,11].
Recent studies have shown that the geo-epidemiological distribution of the epidemic waves varied across countries [1, 12]. Thus, geo-epidemiological analyses using data that are publicly available could be of importance to help governments select and implement efficient health policies [13].
With the worldwide spread of COVID-19 there is a need to better highlight the geo-epidemiological variability in the spatiotemporal trajectory of this pandemic in Europe. The epidemic dynamics may change over time and across areas [14]. Dynamics include increasing trends, leveling off, stationary incidence patterns, and decreasing trends. Because the types and stringency of public health policies vary across counties and locations within a country, classifying and summarizing the geo-epidemiological dynamics of the COVID-19 pandemic is essential for real-time public health policy making [15]. The knowledge about geo-epidemiological dynamics, including the patterns of disease transmission and the factors that influence the spread of diseases, is essential for policymaking to understand how diseases are likely to spread and how to best allocate resources to prevent or mitigate outbreaks. This knowledge can inform the development of policies related to public health, such as vaccination campaigns, quarantine measures, and disease surveillance systems, as well as policies related to travel and trade, which can impact the spread of disease across borders. By basing policy decisions on a thorough understanding of the underlying epidemiological dynamics, policymakers can make informed decisions that are better able to protect the public’s health and prevents the spread of disease.
Data and methods
Using openly available data, I mapped different COVID-19 waves in Europe for June 2020 to August 2021. The data covering the European countries and France are available at no fees [16, 17]. Incident cases were automatically reported per millions persons for Europe [16] and per 100,000 persons in France [17] to make possible comparison of geographical areas with each other.
To create the maps for 13 French provinces and 46 European countries, each epidemic wave started after the lowest number of infections between the previous wave to the subsequent next wave. I consider the European peak time (or the French peak time) when data showed the highest incident European (or French) cases per millions of persons (per 100,000 for France) or for each determined wave (see Supplemental Material, Tables S1 and S2). Information about the first wave were not included in the analyses due to it specific aspect with absence of real PCR test in all countries and the possible bias of non-well-reported incident cases at the beginning of the outbreak.
I then calculated four outcomes as follows:
-
The total cases between cases counts at the date of the European epidemic peak of the each studied wave and cases counts at the minimum of incident cases between the previous wave and the studied wave;
-
The rolling 7-day average for the date of the French or the European peak time of each studied wave;
-
The incidence of new cases for the French or the European peak time of each studied wave; and then,
-
The total new cases between the date of the French or the European peak time and the date of the minimum of infection counts between the studied wave and the one that follows.
Mixed linear regression models were performed on incident cases per 100,000 persons in France and incident cases per million persons in Europe to determine the interaction of time and location (as countries or French provinces) and to determine heterogeneity of the different waves.
For this analysis, incident French cases were reported by states divided by the population of each region and per 100,000 inhabitants, and I then calculated three outcomes as follows:
-
Incident cases per 100,000 persons between cases counts at the date of the French epidemic peak of the each studied wave and cases counts at the minimum of incident cases between the previous wave and the studied wave
-
Incident cases per 100,000 persons seven days before for the date of the French peak time of each studied wave.
-
Incident cases per 100,000 persons between the date of the French peak time and the date of the minimum of infection counts between the studied wave and the one that follows.
To create the maps and to perform analyses, I used SAS software (version 9.4; SAS Institute, Carry, NC).
Results
The maps of four outcomes for 46 European countries show no visual homogenous infection rates across countries for the three detected waves (Fig. 1A, D). On the day of the epidemic peaks for the waves (Supplementary Table S1) Europe maps show different infection rates between the countries on the day of the European peak. This may indicate that national epidemic peaks appeared at different times. The European peak may not be a good indicator for regional or global management of the epidemic. The spatial distribution of total cases between the nadir with minimum infection counts and the European peak timing for the second and third waves show that the fourth wave developed mainly in the Western countries of Europe (Fig. 1A; Supplementary Table S2). The European peak in the countries with the highest rates of infection occurred in the Eastern countries (Fig. 1C). The fourth wave, however, appears to be pronounced primarily in the Western countries, not those in Eastern Europe (Figures of the 4th wave). We also observed similar differences for the rolling 7-day average before the European peak time of each wave (Fig. 1B) and for the incidence of new cases on the day of the European epidemic peak (Fig. 1C).

Total count of new cases per million persons of COVID-19 patients across Europe for three waves (new cases were reported by states divided by the population of each state and per million inhabitants). A The total cases between cases counts at the date of the European epidemic peak of the each studied wave and cases counts at the minimum of incident cases between the previous wave and the studied wave. B The rolling 7-day average for the date of the European peak time of each studied wave. C The incidence of new cases for the European peak time of each studied wave. D The total new cases between the date of the European peak time and the date of the minimum of infection counts between the studied wave and the one that follows
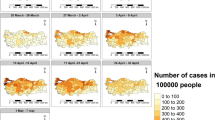
Maps of France at the province level show heterogeneous infection rates over time and across provinces for each three waves (Fig. 2). The maps help to show that the French regional epidemic peaks appear at different times. Thus, a national peak may not be a good indicator for national management of the epidemic. The fourth wave appears to be concentrated mainly in the Southeast rather than the Northwest, list in Supplementary table (Fig. 2).

Total count of new cases per 100,000 persons of COVID-19 patients across France during three waves (new cases were reported by states divided by the population of each region and per 100,000 inhabitants). A The total cases between cases counts at the date of the French epidemic peak of the each studied wave and cases counts at the minimum of incident cases between previous wave and the studied wave. B The rolling 7-day average for the date of the French peak time of each studied wave. C The incidence of new cases for the French peak time of each studied wave. D The total new cases between the date of the French peak time and the date of the minimum of infection counts between the studied wave and the one that follows
When considering incident cases per 100,000 persons and per day, significant interactions time-provinces were observed for the three analyzed waves in France (p for interaction < 0.001 for each wave), when considering analysis A (Fig. 3A) with the incident cases between the date of the French epidemic peak of the each studied wave and the minimum of incident cases between the previous wave and the studied wave; analysis B (p for interaction time-provinces < 0.001, Fig. 3B) when considering the incident cases seven days before the date of the French peak time of each studied wave; and analysis C (p for interaction time-provinces < 0.001, Fig. 3C) when considering the incident cases between the date of the French peak time and the date of the minimum of infection counts between the studied wave and the one that follows. Similar results were observed for all the waves in Europe (p for interaction < 0.001).

Incident cases per 100,000 persons of COVID-19 patients across France during three waves (new cases were reported by states divided by the population of each region and per 100,000 inhabitants). A Incident cases per 100,000 persons between cases counts at the date of the French epidemic peak of the each studied wave and cases counts at the minimum of incident cases between the previous wave and the studied wave. B Incident cases per 100,000 persons seven days before for the date of the French peak time of each studied wave. C Incident cases per 100,000 persons between the date of the French peak time and the date of the minimum of infection counts between the studied wave and the one that follows
Discussion
Numerous studies have investigated the prediction of epidemic trend of COVID-19 [18], but there are few reports of high-resolution, geo-epidemiological maps [19,20,21]. Showing epidemic spatial patterns provides insights about the geographic risks and social and economic determinants related to COVID-19 transmission and inform those planning how to respond to it. This study demonstrated varying geo-epidemiological dynamics in different areas within Europe and in France. It is likely that the presented maps demonstrated that the spread of COVID-19 has gradually shifted from a mostly imported case pattern to a local transmission pattern [22]. Greater transmission risks were likely to be in location with low-detection capacity, high transportation, or economic connections to the epicenter of the outbreak, but with few severely restricting travels, no social distancing, no school closures, and no lockdowns [23,24,25,26,27].
Limitations
This study shows several limitations, results were extrapolated from open available data which can include some errors in the reported data. Moreover, the different models did not consider the situation of each country regarding the different lockdowns or public policies and the time of their implementations which can bias the interpretation of the epidemic peak in Europe. Information about the first wave were not included in the analyses due to it specific aspect with the absence of real PCR test in all countries and the possible bias of non-well-reported incident cases at the beginning of the outbreak.
Conclusions
Geo-epidemiological heterogeneity of the COVID-19 pandemic occurred in regions of France and between the European countries. This observation may provide a basis for the implementation of geo-epidemiological analyses to improve public health policies.
Data availability
Data are open available for Europe at, https://github.com/CSSEGISandData/COVID-19 and for France, at https://www.data.gouv.fr/fr/datasets/synthese-des-indicateurs-de-suivi-de-lepidemie-covid-19/
References
Gaudart J, Landier J, Huiart L, Legendre E, Lehot L, Bendiane MK, et al. Factors associated with the spatial heterogeneity of the first wave of COVID-19 in France: a nationwide geo-epidemiological study. Lancet Public Health. 2021;6:e222–31.
Su D, Chen Y, He K, Zhang T, Tan M, Zhang Y, et al. Influence of socio-ecological factors on COVID-19 risk: a cross-sectional study based on 178 countries/regions worldwide. medRxiv. 2020;2:e198.
Shapira Y, Agmon-Levin N, Shoenfeld Y. Defining and analyzing geoepidemiology and human autoimmunity. J Autoimmun. 2010;34:J168-177.
Rivas AL, van Regenmortel MHV. COVID-19 related interdisciplinary methods: preventing errors and detecting research opportunities. Methods San Diego Calif. 2021;195:3–14.
Fasina FO, Mtui-Malamsha N, Mahiti GR, Sallu R, OleNeselle M, Rubegwa B, et al. Where and when to vaccinate? Interdisciplinary design and evaluation of the 2018 Tanzanian anti-rabies campaign. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. 2020;95:352–60.
Masiira B, Makumbi I, Matovu JKB, Ario AR, Nabukenya I, Kihembo C, et al. Long term trends and spatial distribution of animal bite injuries and deaths due to human rabies infection in Uganda, 2001–2015. PLoS ONE. 2018;13:e0198568.
Rivas AL, Febles JL, Smith SD, Hoogesteijn AL, Tegos GP, Fasina FO, et al. Early network properties of the COVID-19 pandemic: the Chinese scenario. Int J Infect Dis IJID Off Publ Int Soc Infect Dis. 2020;96:519–23.
Rivas AL, Chowell G, Schwager SJ, Fasina FO, Hoogesteijn AL, Smith SD, et al. Lessons from Nigeria: the role of roads in the geo-temporal progression of avian influenza (H5N1) virus. Epidemiol Infect. 2010;138:192–8.
Rivas AL, Fasina FO, Hoogesteyn AL, Konah SN, Febles JL, Perkins DJ, et al. Connecting network properties of rapidly disseminating epizoonotics. PLoS ONE. 2012;7:e39778.
Smith DL, Lucey B, Waller LA, Childs JE, Real LA. Predicting the spatial dynamics of rabies epidemics on heterogeneous landscapes. Proc Natl Acad Sci U S A. 2002;99:3668–72.
Rezaeian M, Dunn G, St Leger S, Appleby L. Geographical epidemiology, spatial analysis and geographical information systems: a multidisciplinary glossary. J Epidemiol Community Health. 2007;61:98–102.
Vallée A. Underestimation of the number of COVID-19 cases, an epidemiological threat. Epidemiol Infect. 2022;150:e191.
Srivastava A, Chowell G. Understanding spatial heterogeneity of COVID-19 pandemic using shape analysis of growth rate curves. J MedRxiv Prepr Serv Health Sci. 2020;42:90.
Simpson RB, Lauren BN, Schipper KH, McCann JC, Tarnas MC, Naumova EN. Critical periods, critical time points and day-of-the-week effects in COVID-19 surveillance data: an example in Middlesex County, Massachusetts, USA. Int J Environ Res Public Health. 2022;19:1321.
Srivast A, Chowell G. Modeling Study: characterizing the spatial heterogeneity of the COVID-19 Pandemic through shape analysis of epidemic curves. Res Sq, 2021. https://doi.org/10.21203/rs.3.rs-223226/v1
https://www.data.gouv.fr/fr/datasets/synthese-des-indicateurs-de-suivi-de-lepidemie-covid-19/.
Arutkin M, Faranda D, Alberti T, Vallée A. Delayed epidemic peak caused by infection and recovery rate fluctuations. Chaos Woodbury N. 2021;31:101107.
Vallée A. Heterogeneity of the COVID-19 pandemic in the United States of America: a geo-epidemiological perspective. Front Public Health. 2022;10:818989.
Darques R, Trottier J, Gaudin R, Ait-Mouheb N. Clustering and mapping the first COVID-19 outbreak in France. BMC Public Health. 2022;22:1279.
Kamel Boulos MN, Geraghty EM. Geographical tracking and mapping of coronavirus disease COVID-19/severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: how 21st century GIS technologies are supporting the global fight against outbreaks and epidemics. Int J Health Geogr. 2020;19:8.
Sigler T, Mahmuda S, Kimpton A, Loginova J, Wohland P, Charles-Edwards E, et al. The socio-spatial determinants of COVID-19 diffusion: the impact of globalisation, settlement characteristics and population. Glob Health. 2021;17:56.
Tirachini A, Cats O. COVID-19 and public transportation: current assessment, prospects, and research needs. J Public Transp. 2020;22:1–21.
Yang Y, Cao M, Cheng L, Zhai K, Zhao X, De Vos J. Exploring the relationship between the COVID-19 pandemic and changes in travel behaviour: a qualitative study. Transp Res Interdiscip Perspect. 2021;11:100450.
De Vos J. The effect of COVID-19 and subsequent social distancing on travel behavior. Transp Res Interdiscip Perspect. 2020;5:100121.
Dzisi EKJ, Dei OA. Adherence to social distancing and wearing of masks within public transportation during the COVID 19 pandemic. Transp Res Interdiscip Perspect. 2020;7:100191.
Ferguson N, Laydon D, Nedjati Gilani G, Imai N, Ainslie K, Baguelin M, et al. Report 9: impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. Imperial College London; 2020. https://doi.org/10.25561/77482
Funding
This research received no external funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares no conflict of interest.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Vallée, A. Geo-epidemiological approach of the COVID-19 pandemic in France and in Europe for public health policies. J Public Health Pol 44, 255–263 (2023). https://doi.org/10.1057/s41271-023-00402-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1057/s41271-023-00402-z