
Abstract
We investigated the impact of germline CYP2D6 genotyping done using the non-tumor specimen on endoxifen concentrations and/or clinical outcomes in breast cancer (BC) patients treated with tamoxifen in published studies. We evaluated published data from 13 001 patients in 29 studies. Mean±s.d. endoxifen concentrations were significantly lower in poor metabolizers (PM) versus extensive metabolizers (EM) (8.8±7.2 versus 22.3±11.8 ng ml−1; P<0.05). The PM status did not influence clinical outcomes in majority of the studies. However, only one study followed the Gaedigk activity scoring for phenotypic assignments, which predicted recurrence-free survival in CYP2D6 poor metabolizers. In two independent studies with 1676 patients, low endoxifen concentrations predicted poor BC-free survival. From our review of published data we found that standardization of CYP2D6 genotype-phenotype classification is needed in order to ensure effective evaluation of associations between CYP2D6 polymorphisms and endoxifen concentrations and BC outcomes. Universal implementation of this standardization classification system should be a priority among researchers and laboratories. Furthermore, additional clinical research is warranted to determine whether patients with CYP2D6 PM phenotypes or low endoxifen levels will have better clinical outcomes with increased tamoxifen dosing compared to standard dosing.
Similar content being viewed by others


Introduction
It is expected that 231 840 women will be diagnosed with invasive breast cancer (BC) in 2015–2016 in the United States.1 About 80% of all invasive BCs express hormone receptors (HR), which include estrogen receptors (ER) and progesterone receptors.2, 3 All patients with HR-positive BC are treated with various types of endocrine therapy, which includes selective estrogen receptor modulator (SERM).4 Tamoxifen is the most extensively used SERM, and is the most common agent used, especially, in premenopausal women for prevention and treatment of BC. Tamoxifen therapy reduces the risk of invasive and non-invasive BC in patients at high risk and also reduces recurrence in BC patients.5, 6, 7
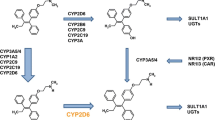
Tamoxifen selectively targets the ER signaling and further inhibits estrogen genomic activity.8 Tamoxifen is metabolized extensively in the liver via cytochrome (CYP) P450 to active metabolite, endoxifen, by two major pathways: N-demethylation and 4-hydroxylation. A major metabolic pathway is demethylation by CYP3A4/5 to N-desmethyltamoxifen, which is further oxidized by CYP2D6 to endoxifen (4-hydroxy-N-desmethyltamoxifen). This pathway contributes to 92% of tamoxifen metabolism.9 Another metabolic pathway includes hydroxylation by CYP2D6 to 4-hydroxytamoxifen (4HT), which is then further metabolized by CYP3A4 to the active metabolite, endoxifen. While not many function-altering variants in CYP3A4/5 metabolism have been reported, CYP2D6 is a highly polymorphic enzyme with over 100 variants reported commonly in many patients.10 Therefore, pharmacogenomics of CYP2D6 seems to be one of the more significant determinants of tamoxifen bio-activation to endoxifen and its overall potential impact on efficacy outcomes in BC patients.
Although many studies have evaluated the role of CYP2D6 polymorphisms on endoxifen concentrations as well as long-term clinical outcomes with tamoxifen, the results are conflicting.7 Retrospective analysis of two large prospectively conducted studies (ATAC and BIG 1-98) reported that CYP2D6 genotype did not impact clinical outcomes with tamoxifen.11, 12 However, these studies used the tumor DNA for the CYP2D6 genotyping. Several publications suggest that many BCs have gene deletions on chromosome 22 near the CYP2D6 locus (22q13), resulting in a loss of heterozygosity, contributing to a significant deviation of the genotype distribution from Hardy-Weinberg equilibrium.13, 14, 15, 16, 17 It is likely that this phenomenon may have skewed the accuracy of some of the studies accounting for specific CYP2D6 genetic variations in BC patients. To overcome this issue, we conducted a systematic analysis of published clinical studies that have utilized normal/healthy tissue for CYP2D6 analysis to describe the relationship between CYP2D6 genotype, endoxifen concentrations, and BC outcomes. We have found that CYP2D6 phenotype assigned based on the genotype in non-tumor tissues significantly impacts endoxifen concentrations, but its impact on BC outcomes is less clear. We also discuss here the clinical implications of these results and propose future directions for clinical research in this area.
Materials and methods
Search strategy
A systematic search of the literature via PUBMED was initially performed using the following expanded Medical Subject Headings (MESH) terms: ‘tamoxifen’, ‘CYP2D6', ‘breast cancer’, and ‘endoxifen’ or ‘recurrence’ with the search limit ‘title/abstract’. The search was conducted on 24 May, 2017 with no date restrictions. Additional reports were obtained from the references of the published papers and clinical trials related to the topic of the meta-analysis.
Selection criteria
The reports were selected after the abstracts were reviewed for the inclusion and exclusion criteria. Eligibility criteria for inclusion comprised of the following: full text articles, published in English, reporting either endoxifen concentrations for each phenotype and/or BC outcomes based on the analysis of CYP2D6 genotype, use of non-tumor specimens, in premenopausal or postmenopausal women, with high risk of BC or patients with BC who were treated with tamoxifen 20 mg by mouth daily for at least 4 weeks. Studies reporting BC outcomes based on endoxifen levels were also included. Exclusion criteria were studies reporting duplicate results, studies performed using formalin-fixed paraffin-embedded (FFPE) tumor tissues, studies described only as abstracts or correspondence, and those using non-traditional tamoxifen dosing. Both prospective and retrospective studies were included. Each study was critically evaluated for validity based on consistency, accuracy, and balance between the groups, if applicable.
Data collection
From each study, we recorded the following information: sample size (N), stage of the BC, menopausal stage (and % of patients in each category), age, CYP2D6 sample, CYP2D6 analysis tool, endoxifen sample, time points for the endoxifen sample, endoxifen analysis tool, endoxifen concentrations for each CYP2D6 phenotype classification, hot flash experience, concomitant medication usage and BC outcome (such as BC-specific survival (BCSS), recurrence-free survival (RFS), disease-free survival (DFS), progression-free survival (PFS), and/or overall survival (OS)). Since CYP2D6 phenotype was determined based on its genotype using different criteria in various publications, the definition of poor metabolizer (PM), intermediate metabolizer (IM), extensive metabolizer (EM) and ultra-rapid metabolizer (UM) was recorded separately in Supplementary Table 1. The activity score was calculated for the genotypes considered in each phenotypic category to compare various studies based on the PharmGKB website for CYP2D6 and tamoxifen (https://www.pharmgkb.org/guideline/PA166104966) and the criteria previously published.18 Gaedigk activity score definition for CYP2D6 was considered 0 for PM, 0.5 for IM, 1.0–2.0 for EM, and >2.0 for UM.18, 19 Endoxifen values were reported in ng ml−1. For consistent reporting, nM values were multiplied by 0.3735 to obtain ng ml−1 for endoxifen concentrations.
Data analysis
To assess the relationship between the CYP2D6 phenotype and endoxifen concentrations, only studies with documented endoxifen concentrations for any of the CYP2D6 phenotypes were included. Studies with endoxifen concentration reported as mean±standard deviation (s.d.) or 95% CI were included in the graphical representation. The difference in endoxifen concentrations between CYP2D6 phenotypes were evaluated using one-way analysis of variance (ANOVA) analysis, followed by Dunnette’s multiple comparison post hoc test. All the studies, even when the endoxifen values were reported as a median value, were tabulated and described. The association between CYP2D6 phenotypes and BC outcomes were summarized using descriptive statistics as reported in individual studies.
Results
Study characteristics and patient demographics
Total of 217 records were obtained from PUBMED search. Figure 1 describes the selection of articles for this study. We evaluated the data for 13 001 patients from a total of 29 studies.

Flow chart of literature review process. The flow chart describes numbers of studies that are included in our analysis and the reasons other studies are excluded.
Detailed information on all the studies included in this review is provided in Table 1. Among the 29 articles,20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48 18 were prospective studies including cohort studies,20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37 and three were case-control studies.38, 39, 40 The other eight articles were retrospective studies.41, 42, 43, 44, 45, 46, 47, 48 Eighteen studies included patients in the early stage BC and on tamoxifen adjuvant therapy.21, 23, 26, 27, 28, 29, 30, 31, 32, 34, 35, 37, 40, 42, 43, 45, 47, 48 Two of the articles evaluated patients on tamoxifen for prevention purposes;38, 46 whereas one study was in the recurrence/metastatic setting.41 Six studies included patients of all stages of cancer including metastatic stage.20, 24, 33, 36, 39, 44 Two studies did not report the stage of BC for the subjects enrolled in the study.22, 25 Overall, all studies included premenopausal or postmenopausal female patients with ER-positive BC at age of 18 or older. The activity scores calculated for each of the phenotypic categories as assigned by each of the studies are summarized in Table 1. Gaedigk activity score definition for CYP2D6 was considered 0 for PM, 0.5 for IM, 1.0–2.0 for EM, and >2.0 for UM.18, 19 Out of 29 studies, 28 did not follow this standard definition of activity score to assign various genotypes in each phenotypic category (Table 1). In these 28 studies, most had an overlap in the activity scores for different CYP2D6 phenotypes as calculated in Table 1. Only one study reported BC outcomes using this activity scoring classification system.24 Most studies reported if patients used any concomitant medications such as CYP2D6 inhibitors, since these may cause drug-drug interactions with tamoxifen therapy. However, detailed description in terms of their CYP2D6 inhibitory activity (strong, medium, weak) of these medications was not provided in most studies.
Association between CYP2D6 phenotypes and endoxifen concentrations
A total of 11 studies reported endoxifen concentrations based on CYP2D6 phenotypes. All these studies collected blood samples from subjects to determine CYP2D6 genotypes and characteristic phenotypes. Only the studies with mean values±s.d. reported were considered in Figure 2,23, 27, 28, 29, 30, 31, 41, 42 while the studies with median value reported are included in Table 2 separately.21, 25, 26 Mean endoxifen concentrations reported in 8 studies (N=2861) were 2.5-fold lower in subjects who had CYP2D6 PM phenotypes (8.8 ± 7.2 ng ml−1) compared to those with CYP2D6 EM phenotypes (22.3±11.8 ng ml−1; P⩽0.05, One-way ANOVA followed by Dunnett’s multiple comparison post hoc test). There were no significant differences between endoxifen concentrations in subjects who had CYP2D6 IM phenotypes (15.7±10.8 ng ml−1) or UM phenotypes (20.8±9.2 ng ml−1) compared to the subjects with EM phenotypes. In the three studies reporting median values with range, the endoxifen concentrations numerically increased from PM to IM to EM to UM (Table 2).

Endoxifen concentrations in patients with various CYP2D6 phenotypes. The mean±s.d. of endoxifen concentration (ng ml−1) is plotted as a bar graph for each CYP2D6 phenotype from 8 studies (N=2861). * indicates statistically significant difference (P<0.05, One-way ANOVA followed by Dunnette's multiple comparison test). Although different studies defined CYP2D6 phenotypes differently, we found that mean endoxifen concentrations were significantly lower in the poor metabolizer (PM) group versus the extensive metabolizer (EM) group. There were no significant differences between mean endoxifen concentrations in the intermediate metabolizer (IM) or ultra-rapid metabolizer (UM) groups versus the EM group.
Correlation between CYP2D6 phenotypes and BC outcomes
A total of 20 studies reported BC outcomes in patients who had available information regarding CYP2D6 phenotypes (Table 3). Eleven studies reported survival outcomes such as BCSS, RFS, DFS, or PFS,20, 24, 26, 30, 36, 37, 43, 44, 45, 46, 48 out of which 3 studies also reported OS.20, 35, 36 Seven additional studies reported BC recurrence or disease event.25, 33, 34, 35, 39, 43, 46 Whereas, BC mortality (BCM),22 time to progression (TTP),41 and recurrence-free time47were reported by one study each. Among the 20 studies, only nine studies reported significant associations between patients who had CYP2D6 PM phenotypes and a higher risk of BCM, higher recurrence rate, poorer RFS or OS, or faster TTP compared to those patients with CYP2D6 EM phenotypes.22, 24, 26, 33, 34, 37, 40, 41, 48 The remaining eleven studies found no significant associations between CYP2D6 phenotypes and BC outcomes.20, 30, 35, 36, 38, 39, 43, 44, 45, 46, 47 However, only one study24 out of the 20 we reviewed followed the Gaedigk activity scoring for CYP2D6 phenotypic assignments, which reported poor recurrence-free survival in CYP2D6 poor metabolizers.
Correlation between endoxifen concentrations and BC outcomes
Two studies reported BC outcomes in relationship to endoxifen concentrations. The study by Madlensky et al.,27 reported that among 1370 patients, those with endoxifen concentrations above 5.97 ng ml−1 (15.98 nm) had 30% lower risk of additional BC events (HR=0.70, 95% confidence interval: 0.52–0.94). Another study by Saladores et al.32 found that among 548 premenopausal hormone receptor-positive BC patients who were adherent to tamoxifen therapy, those with low (<14 nm or <5.2 ng ml−1) compared with high (>35 nm or >13.1 ng ml−1) endoxifen concentrations were associated with shorter distant relapse-free survival (univariate P=0.03; multivariate HR=1.94; 95% confidence interval: 1.04–4.14, P=0.064).
Ongoing clinical trials
We also reviewed current ongoing clinical trials to determine if any additional information was available regarding our topic of study. An on-line search was done on 9 April, 2017 using the clinical trials website (clinicaltrials.gov) of US National Institutes of Health. Among the 22 studies matched with the terms ‘tamoxifen,’ ‘breast cancer,’ and ‘CYP2D6,’ three were excluded due to termination or withdrawal of the study. Three studies were also excluded because CYP2D6 genotypes of BC patients were not analyzed. All of the 16 relevant ongoing studies being conducted in pre- or postmenopausal adult BC patients are summarized in Table 4.
Among the 16 studies, 6 studies are interventional studies, whereas 10 studies are observational. Among the six interventional studies, four studies are investigating the impact of increasing tamoxifen dose (from 20 to 40 mg per day) on its metabolism in patients with PM or IM CYP2D6 phenotypes (NCT01075802, NCT01192308, NCT00764322, NCT00963209). One study is investigating the incidence of invasive and non-invasive BC with 5 mg per day tamoxifen versus placebo in patients with ductal/lobular carcinoma-in situ (NCT01357772), and the other study is evaluating the safety and maximum tolerated dose (MTD) of Z-endoxifen (NCT01273168) in patients with metastatic BC. Among the 10 observational studies, the primary objective of 6 of these studies is to evaluate the effects of CYP2D6 polymorphisms and/or phenotype on tamoxifen metabolism (NCT00717015, 01220076,00900744) or disease/progression-free survival (NCT00973037, 01181518, 01124695). The frequency of CYP2D6 polymorphisms and phenotype and its association with outcomes is investigated in 2 additional studies (NCT01169792, 00830973). One study is investigating the effect of endoxifen concentrations on BC outcomes (NCT00815555), and another study is evaluating changes in tamoxifen metabolism when using concomitant administration of medications that are CYP2D6 inhibitors (NCT00667121). The latter two studies mentioned above are critical to determine the importance of using therapeutic drug monitoring for endoxifen concentrations to help guide appropriate tamoxifen dosing to ensure positive treatment outcomes. These studies may also be helpful to further define potential clinically relevant drug–drug interactions in patients using both tamoxifen and CYP2D6 inhibitors. However, all these studies are being conducted in relatively small number of patients, and additional larger clinical trials are necessary to better understand this clinically important issue.
Discussion
Our systematic analysis found that endoxifen concentrations were significantly lower in patients with PM phenotype for CYP2D6 compared to EM phenotype. The difference in the endoxifen concentrations in the patients with the CYP2D6 IM and UM phenotypes compared to EM phenotype were not statistically significant. The PM status did not impact clinical outcomes in majority of the studies. However, only one study followed the Gaedigk activity scoring for phenotypic assignments,24 which reported poor RFS in poor metabolizers. In two independent studies with 1,676 patients, low endoxifen concentrations predicted poor BC-free survival. Below, we discuss the strengths and limitations of our analysis, discuss the potential reasons for discrepancies in various studies, and suggest future directions of clinical research in this area.
One of the challenges in understanding the role of CYP2D6 is the source of tissue for its genotyping. Cancer in general, including BC, has significant chromosomal instability, accounting for loss of regions on various chromosomes. In the past, evaluation of FFPE tumor samples have led to misinterpretation of the data because of loss of heterozygosity in these samples and caused deviations from Hardy–Weinberg principles.17 Therefore, using tumor tissues for genotyping may not be the best method to obtain accurate results. While the bias caused by discordant genotyping has been debated,49 non-tumor tissues provide more suitable material for germline DNA analysis. In our study, only the studies assessing the germline rather than somatic mutations in CYP2D6 were included to avoid this concern.
Lack of consensus between various studies evaluated here stem from various definitions for CYP2D6 phenotype and differences in clinical characteristics. For example, some studies classified only CYP2D6 *4/*4 as PM; whereas, other studies included other genotypes such as CYP2D6 *3/*3, *3/*5, *6/*9, *4/*10, and *5/*41 in the PM category as well. As of now, there is no standardization of the CYP2D6 genotype to phenotype classification. Interestingly, only one study out of 20 reporting the relationship between CYP2D6 phenotype and BC outcomes followed the activity score guidelines adopted by Clinical Pharmacogenetics Implementation Consortium (CPIC) which was initially introduced by Gaedigk et al.18 Because most studies did not follow the Gaedigk activity score classification system, it is possible that discrepancies between studies can be accounted for by variable definitions used to determine CYP2D6 phenotypes. This information reflects a common, unmet clinical need to standardize the genotype–phenotype classification for CYP2D6 and ensure adequate education of researchers and laboratories conducting genetic testing so that proper assignment of CYP2D6 phenotypes is successfully implemented.
Another source of discrepancy could be the smaller sample size in most of the studies impacting the results, especially, considering the highly polymorphic nature of CYP2D6. Moreover, some studies tested many different alleles; whereas, others had only 2 (*1 and *4) for assignment of the phenotype. The testing of fewer alleles could also result in more patients with CYP2D6 genetic alterations being categorized in the EM group by default. In addition, all studies did not have a consensus on patient usage of concomitant medications. While some studies excluded the patients using CYP2D6 inhibitors or selective serotonin reuptake inhibitors (SSRIs), other studies included information regarding patient usage of these medications. Knowledge of concomitant medications that are strong CYP2D6 inhibitors is important since these can affect the metabolism of tamoxifen, as well as resulting endoxifen concentrations. For example, patients who might have a CYP2D6 EM phenotype and are concomitantly taking strong CYP2D6 inhibitors will essentially have a phenotype conversion to a CYP2D6 PM phenotype. Therefore, specific knowledge of drug–drug interactions and the degree of inhibition of concomitant medications is necessary to fully determine its overall impact on the appropriate use of tamoxifen therapy, its disposition, and related clinical outcomes.
Patient-specific factors may also influence tamoxifen metabolism; it is possible that these were not controlled for among the different studies. Because tamoxifen is a competitive antagonist for estrogen receptors, the levels of estrogen will impact the potency of tamoxifen, and hence would be relevant at least from the efficacy perspective. For example, one study found an association between reduced CYP2D6 activity and recurrence and breast cancer-specific mortality mostly in premenopausal women.34 Large studies in a specific group of patients (regards to age, menopausal status, treatment setting, stage, tumor type, grade and so on) may help us resolve this issue in a systematic manner. While DNA analysis method and endoxifen concentration assay may also be a potential source of variation, most of these methods have been validated and were concordant across various platforms in our review of the clinical studies. A clinical marker for tamoxifen metabolism is the presence of hot flashes. It is considered to be a better marker of tamoxifen treatment outcome. However, only 3 studies evaluated this toxicity based on genotyping, and the findings were not consistent in those studies, further suggesting the need for its evaluation in future studies.25, 31, 46
Since multiple patient- and tumor-specific factors determine the efficacy of tamoxifen in BC patients, large prospective studies are necessary to evaluate the role of CYP2D6 phenotype, endoxifen concentrations, and concomitant administration with strong CYP2D6 inhibitors on predicting BC outcomes to improve clinical management of BC patients. Because of the highly polymorphic nature of CYP2D6 that varies among different ethnicities, many variants exist to impact patients’ endoxifen concentrations. Therapeutic drug monitoring of endoxifen concentrations may serve well in guiding appropriate tamoxifen dosing or determining whether alternative therapies for BC should be chosen. Two independent studies showed the value of endoxifen concentration monitoring to predict treatment failure.27, 32 Clinical trials are needed to assess the efficacy of higher doses of tamoxifen in patients with low endoxifen steady state concentrations. Currently, there are ongoing or completed studies to evaluate the use of higher tamoxifen dosing in patients who have CYP2D6 PM phenotypes and their effects on endoxifen concentrations. The range of endoxifen concentrations observed in the PM category is wide with the mean (8.8 ng ml−1) higher than the concentration (~6 ng ml−1) below which poor clinical outcomes are observed. Furthermore, there is a big discrepancy regarding the effects of CYP2D6 genotyping on clinical outcomes. Therefore, we believe that using a combination approach including CYP2D6 genotyping with therapeutic drug monitoring of endoxifen concentrations is probably the most ideal strategy to ensure the best clinical outcomes for BC, and deserves further evaluation in future clinical studies.
Our systematic analysis suggests that CYP2D6 PM phenotype significantly predicts lower endoxifen concentrations in patients receiving a tamoxifen 20 mg once daily regimen. Meanwhile, the overall effects of different CYP2D6 phenotypes on BC outcomes are less clear. Future well-designed, controlled, larger clinical studies are warranted to determine if CYP2D6 genotyping and therapeutic drug monitoring of endoxifen concentrations can be used to improve treatment outcomes in BC patients. However, before these trials are initiated, standardization of CYP2D6 genotype–phenotype classification is needed in order to ensure effective evaluation of associations between CYP2D6 polymorphisms and endoxifen concentrations and BC outcomes. Before such data is available, we recommend that patients who have CYP2D6 PM phenotypes either be enrolled in appropriate clinical trials evaluating higher than normal dosing of tamoxifen with endoxifen concentration monitoring or be considered for alternative therapies such as aromatase inhibitors. Concomitant administration of strong CYP2D6 inhibitors should be avoided while patients are on tamoxifen. The importance of adequate adherence should also be discussed with all BC patients on tamoxifen regardless of their CYP2D6 genotype to increase disease-free survival.
References
Siegel RL, Miller KD, Jemal A . Cancer statistics, 2015. CA Cancer J Clin 2015; 65: 5–29.
Clark GM, Osborne CK, McGuire WL . Correlations between estrogen receptor, progesterone receptor, and patient characteristics in human breast cancer. J Clin Oncol 1984; 2: 1102–1109.
Osborne CK . Steroid hormone receptors in breast cancer management. Breast Cancer Res Treat 1998; 51: 227–238.
Lumachi F, Santeufemia DA, Basso SM . Current medical treatment of estrogen receptor-positive breast cancer. World J Biol Chem 2015; 6: 231–239.
Wolmark N, Dunn BK . The role of tamoxifen in breast cancer prevention: issues sparked by the NSABP Breast Cancer Prevention Trial (P-1). Ann N Y Acad Sci 2001; 949: 99–108.
Vogel VG . Follow-up of the breast cancer prevention trial and the future of breast cancer prevention efforts. Clin Cancer Res 2001; 7 (12 Suppl): 4413s–4418ss, discussion 1–2s.
Markopoulos C, Kykalos S, Mantas D . Impact of CYP2D*6 in the adjuvant treatment of breast cancer patients with tamoxifen. World J Clin Oncol 2014; 5: 374–381.
Walko CM, McLeod H . Use of CYP2D6 genotyping in practice: tamoxifen dose adjustment. Pharmacogenomics 2012; 13: 691–697.
Desta Z, Ward BA, Soukhova NV, Flockhart DA . Comprehensive evaluation of tamoxifen sequential biotransformation by the human cytochrome P450 system in vitro: prominent roles for CYP3A and CYP2D6. J Pharmacol Exp Ther 2004; 310: 1062–1075.
Kim J, Lim YR, Han S, Han JS, Chun YJ, Yun CH et al. Functional influence of human CYP2D6 allelic variations: P34S, E418K, S486T, and R296C. Arch Pharm Res 2013; 36: 1500–1506.
Breast International Group 1-98 Collaborative G, Thurlimann B, Keshaviah A, Coates AS, Mouridsen H, Mauriac L et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005; 353: 2747–2757.
Cuzick J, Sestak I, Baum M, Buzdar A, Howell A, Dowsett M et al. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol 2010; 11: 1135–1141.
Castells A, Gusella JF, Ramesh V, Rustgi AK . A region of deletion on chromosome 22q13 is common to human breast and colorectal cancers. Cancer Res 2000; 60: 2836–2839.
Hirano A, Emi M, Tsuneizumi M, Utada Y, Yoshimoto M, Kasumi F et al. Allelic losses of loci at 3p25.1, 8p22, 13q12, 17p13.3, and 22q13 correlate with postoperative recurrence in breast cancer. Clin Cancer Res 2001; 7: 876–882.
Loo LW, Ton C, Wang YW, Grove DI, Bouzek H, Vartanian N et al. Differential patterns of allelic loss in estrogen receptor-positive infiltrating lobular and ductal breast cancer. Genes Chromosomes Cancer 2008; 47: 1049–1066.
Nakamura Y, Ratain MJ, Cox NJ, McLeod HL, Kroetz DL, Flockhart DA . Re: CYP2D6 genotype and tamoxifen response in postmenopausal women with endocrine-responsive breast cancer: the Breast International Group 1-98 trial. J Natl Cancer Inst 2012; 104: 1264 author reply 6-8.
Goetz MP, Sun JX, Suman VJ, Silva GO, Perou CM, Nakamura Y et al. Loss of heterozygosity at the CYP2D6 locus in breast cancer: implications for germline pharmacogenetic studies. J Natl Cancer Inst 2014; 107: dju401.
Gaedigk A, Simon SD, Pearce RE, Bradford LD, Kennedy MJ, Leeder JS . The CYP2D6 activity score: translating genotype information into a qualitative measure of phenotype. Clin Pharmacol Ther 2008; 83: 234–242.
Crews KR, Gaedigk A, Dunnenberger HM, Leeder JS, Klein TE, Caudle KE et al. Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clin Pharmacol Ther 2014; 95: 376–382.
Abraham JE, Maranian MJ, Driver KE, Platte R, Kalmyrzaev B, Baynes C et al. CYP2D6 gene variants: association with breast cancer specific survival in a cohort of breast cancer patients from the United Kingdom treated with adjuvant tamoxifen. Breast Cancer Res 2010; 12: R64.
Barginear MF, Jaremko M, Peter I, Yu C, Kasai Y, Kemeny M et al. Increasing tamoxifen dose in breast cancer patients based on CYP2D6 genotypes and endoxifen levels: effect on active metabolite isomers and the antiestrogenic activity score. Clin Pharmacol Ther 2011; 90: 605–611.
Bijl MJ, van Schaik RH, Lammers LA, Hofman A, Vulto AG, van Gelder T et al. The CYP2D6*4 polymorphism affects breast cancer survival in tamoxifen users. Breast Cancer Res Treat 2009; 118: 125–130.
Borges S, Desta Z, Li L, Skaar TC, Ward BA, Nguyen A et al. Quantitative effect of CYP2D6 genotype and inhibitors on tamoxifen metabolism: implication for optimization of breast cancer treatment. Clin Pharmacol Ther 2006; 80: 61–74.
Damodaran SE, Pradhan SC, Umamaheswaran G, Kadambari D, Reddy KS, Adithan C . Genetic polymorphisms of CYP2D6 increase the risk for recurrence of breast cancer in patients receiving tamoxifen as an adjuvant therapy. Cancer Chemother Pharmacol 2012; 70: 75–81.
Irvin WJ Jr., Walko CM, Weck KE, Ibrahim JG, Chiu WK, Dees EC et al. Genotype-guided tamoxifen dosing increases active metabolite exposure in women with reduced CYP2D6 metabolism: a multicenter study. J Clin Oncol 2011; 29: 3232–3239.
Kiyotani K, Mushiroda T, Imamura CK, Hosono N, Tsunoda T, Kubo M et al. Significant effect of polymorphisms in CYP2D6 and ABCC2 on clinical outcomes of adjuvant tamoxifen therapy for breast cancer patients. J Clin Oncol 2010; 28: 1287–1293.
Madlensky L, Natarajan L, Tchu S, Pu M, Mortimer J, Flatt SW et al. Tamoxifen metabolite concentrations, CYP2D6 genotype, and breast cancer outcomes. Clin Pharmacol Ther 2011; 89: 718–725.
Murdter TE, Schroth W, Bacchus-Gerybadze L, Winter S, Heinkele G, Simon W et al. Activity levels of tamoxifen metabolites at the estrogen receptor and the impact of genetic polymorphisms of phase I and II enzymes on their concentration levels in plasma. Clin Pharmacol Ther 2011; 89: 708–717.
Opdam FL, Dezentje VO, den Hartigh J, Modak AS, Vree R, Batman E et al. The use of the 13C-dextromethorphan breath test for phenotyping CYP2D6 in breast cancer patients using tamoxifen: association with CYP2D6 genotype and serum endoxifen levels. Cancer Chemother Pharmacol 2013; 71: 593–601.
Park IH, Ro J, Park S, Lim HS, Lee KS, Kang HS et al. Lack of any association between functionally significant CYP2D6 polymorphisms and clinical outcomes in early breast cancer patients receiving adjuvant tamoxifen treatment. Breast Cancer Res Treat 2012; 131: 455–461.
Ruddy KJ, Desantis SD, Gelman RS, Wu AH, Punglia RS, Mayer EL et al. Personalized medicine in breast cancer: tamoxifen, endoxifen, and CYP2D6 in clinical practice. Breast Cancer Res Treat 2013; 141: 421–427.
Saladores P, Murdter T, Eccles D, Chowbay B, Zgheib NK, Winter S et al. Tamoxifen metabolism predicts drug concentrations and outcome in premenopausal patients with early breast cancer. Pharmacogenomics J 2015; 15: 84–94.
Teh LK, Mohamed NI, Salleh MZ, Rohaizak M, Shahrun NS, Saladina JJ et al. The risk of recurrence in breast cancer patients treated with tamoxifen: polymorphisms of CYP2D6 and ABCB1. AAPS J 2012; 14: 52–59.
Margolin S, Lindh JD, Thoren L, Xie H, Koukel L, Dahl ML et al. CYP2D6 and adjuvant tamoxifen: possible differences of outcome in pre- and post-menopausal patients. Pharmacogenomics 2013; 14: 613–622.
Markkula A, Hjertberg M, Rose C, Ingvar C, Jernstrom H . No association found between CYP2D6 genotype and early breast cancer events in tamoxifen-treated patients. Acta Oncol 2014; 53: 195–200.
Okishiro M, Taguchi T, Jin Kim S, Shimazu K, Tamaki Y, Noguchi S . Genetic polymorphisms of CYP2D6 10 and CYP2C19 2, 3 are not associated with prognosis, endometrial thickness, or bone mineral density in Japanese breast cancer patients treated with adjuvant tamoxifen. Cancer 2009; 115: 952–961.
Park HS, Choi JY, Lee MJ, Park S, Yeo CW, Lee SS et al. Association between genetic polymorphisms of CYP2D6 and outcomes in breast cancer patients with tamoxifen treatment. J Korean Med Sci 2011; 26: 1007–1013.
Goetz MP, Schaid DJ, Wickerham DL, Safgren S, Mushiroda T, Kubo M et al. Evaluation of CYP2D6 and efficacy of tamoxifen and raloxifene in women treated for breast cancer chemoprevention: results from the NSABP P1 and P2 clinical trials. Clin Cancer Res 2011; 17: 6944–6951.
Brooks JD, Teraoka SN, Malone KE, Haile RW, Bernstein L, Lynch CF et al. Variants in tamoxifen metabolizing genes: a case-control study of contralateral breast cancer risk in the WECARE study. Int J Mol Epidemiol Genet 2013; 4: 35–48.
Sirachainan E, Jaruhathai S, Trachu N, Panvichian R, Sirisinha T, Ativitavas T et al. CYP2D6 polymorphisms influence the efficacy of adjuvant tamoxifen in Thai breast cancer patients. Pharmgenomics Pers Med 2012; 5: 149–153.
Lim HS, Ju Lee H, Seok Lee K, Sook Lee E, Jang IJ, Ro J . Clinical implications of CYP2D6 genotypes predictive of tamoxifen pharmacokinetics in metastatic breast cancer. J Clin Oncol 2007; 25: 3837–3845.
Love RR, Desta Z, Flockhart D, Skaar T, Ogburn ET, Ramamoorthy A et al. CYP2D6 genotypes, endoxifen levels, and disease recurrence in 224 Filipino and Vietnamese women receiving adjuvant tamoxifen for operable breast cancer. Springerplus 2013; 2: 52.
Newman WG, Hadfield KD, Latif A, Roberts SA, Shenton A, McHague C et al. Impaired tamoxifen metabolism reduces survival in familial breast cancer patients. Clin Cancer Res 2008; 14: 5913–5918.
Nowell SA, Ahn J, Rae JM, Scheys JO, Trovato A, Sweeney C et al. Association of genetic variation in tamoxifen-metabolizing enzymes with overall survival and recurrence of disease in breast cancer patients. Breast Cancer Res Treat 2005; 91: 249–258.
Ramon y Cajal T, Altes A, Pare L, del Rio E, Alonso C, Barnadas A et al. Impact of CYP2D6 polymorphisms in tamoxifen adjuvant breast cancer treatment. Breast Cancer Res Treat 2010; 119: 33–38.
Sestak I, Kealy R, Nikoloff M, Fontecha M, Forbes JF, Howell A et al. Relationships between CYP2D6 phenotype, breast cancer and hot flushes in women at high risk of breast cancer receiving prophylactic tamoxifen: results from the IBIS-I trial. Br J Cancer 2012; 107: 230–233.
Mwinyi J, Vokinger K, Jetter A, Breitenstein U, Hiller C, Kullak-Ublick GA et al. Impact of variable CYP genotypes on breast cancer relapse in patients undergoing adjuvant tamoxifen therapy. Cancer Chemother Pharmacol 2014; 73: 1181–1188.
Sukasem C, Sirachainan E, Chamnanphon M, Pechatanan K, Sirisinha T, Ativitavas T et al. Impact of CYP2D6 polymorphisms on tamoxifen responses of women with breast cancer: a microarray-based study in Thailand. Asian Pac J Cancer Prev 2012; 13: 4549–4553.
Ahern TP, Hertz DL, Damkier P, Ejlertsen B, Hamilton-Dutoit SJ, Rae JM et al. Cytochrome P-450 2D6 (CYP2D6) genotype and breast cancer recurrence in tamoxifen-treated patients: evaluating the importance of loss of heterozygosity. Am J Epidemiol 2017; 185: 75–85.
Acknowledgements
This paper was presented at 2016 Hematology/Oncology Pharmacy Association (HOPA) Annual Conference in Atlanta, GA and at 2016 American College of Clinical Pharmacy (ACCP) Annual Conference in Hollywood, FL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the The Pharmacogenomics Journal website
Supplementary information
PowerPoint slides
Rights and permissions
About this article

Cite this article
Hwang, G., Bhat, R., Crutchley, R. et al. Impact of CYP2D6 polymorphisms on endoxifen concentrations and breast cancer outcomes. Pharmacogenomics J 18, 201–208 (2018). https://doi.org/10.1038/tpj.2017.36
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tpj.2017.36
- Springer Nature Limited
This article is cited by
-
Therapeutic Drug Monitoring of Endoxifen for Tamoxifen Precision Dosing: Feasible in Patients with Hormone-Sensitive Breast Cancer
Clinical Pharmacokinetics (2022)
-
Pharmacogenetics of tamoxifen therapy in Asian populations: from genetic polymorphism to clinical outcomes
European Journal of Clinical Pharmacology (2021)
-
Pharmacogenomics of breast cancer: highlighting CYP2D6 and tamoxifen
Journal of Cancer Research and Clinical Oncology (2020)
-
The Effect of Selenium on CYP450 Isoform Activity and Expression in Pigs
Biological Trace Element Research (2020)