
Abstract
Cisplatin remains to be primary chemotherapeutic drug for gastric cancer patients, especially for advanced stage ones. However, primary or acquired resistance often occurs with the mechanisms being not well understood, which results in relapse of the cancer and poor survival. Herein, we found that HER2 upregulation was associated with cisplatin resistance. We observed that cisplatin-resistant gastric cancer cells underwent a morphological change similar to epithelial-mesenchymal transition (EMT) which is mediated by HER2 overexpression. When specific monoclonal antibody Herceptin, small molecular targeted drug CP724714, or small interfering RNA against HER2 was applied, the EMT-like phenotypic change was dramatically reversed. More importantly, the IC50 and Resistance Index of resistant gastric cancer cells to cisplatin were also decreased by any of these treatments.We demonstrated that expression and amplification of HER2 positively correlated with expression of EMT-related transcription factor Snail in gastric cancer tissues. Furthermore, for the first time, we found that HER2/Snail double positive gastric cancer patients had poorer survival than single positive or double negative counterparts, which provided experimental evidence for the necessity of HER2/Snail double testing in gastric cancer. In conclusion, this study provides some clues of the association of cisplatin resistance with HER2 upregulation-induced EMT in gastric cancer cells.
Similar content being viewed by others


Introduction
Gastric cancer is one of the most common malignancies worldwide. Despite recent advances in diagnosis and treatment as well as declining incidence in some developed countries, it remains a major cause of cancer-related deaths in China1,2. Gastric cancer in early stages is curable by using endoscopic procedures. However, it is difficult to cure in most advanced-stage patients and the clinical treatment options have evolved little3. Until now, chemotherapy still remains mainstream treatment for gastric cancer patients with advanced stage4,5,6. Among them, many are resistant to chemotherapy agents, including cisplatin7,8,9. So, investigating the mechanisms underlying chemotherapy-induced resistance has clinical significance.
Epithelial-mesenchymal transition (EMT) is a process in which epithelial cells lose their polarity and cell-cell adhesion signatures and acquire the characteristics of mesenchymal cells, including spindle-cell shape, loss of polarity, intercellular separation and pseudopodia formation10,11,12. During EMT, the expression of some epithelial cell markers, such as E-cadherin, Claudin1 and zonula occluden-1 (ZO1), decreased, while the expression of mesenchymal cell markers, such as vimentin and fibronectin, increased. EMT-related transcription factors, like Snail, Slug, ZEB1, ZEB2 and Twist, are also upregurated. EMT is involved in both physiological and pathological processes. It not only participates in embryonic development processes10, but also plays a critical role in many aspects of cancer biological behaviors, such as migration and invasion, metastasis and the acquisition of stem cell-like properties12,13,14,15. EMT of Cancer cells also associates with resistance to chemotherapy16,17,18,19. Up-regulation of Twist was associated with resistance to paclitaxel in human nasopharyngeal, bladder, ovarian and prostate cancers16. In colorectal cancer, oxaliplatin-resistant cells can acquire the ability to migrate and invade with phenotypic changes resembling EMT17. In pancreatic and ovarian cancer, stable cell lines resistant to gemcitabine and paclitaxel established by continuous exposure can undergo EMT with increased expression of Snail and Twist18,19. However, there has no study investigating the role of EMT in mediating cisplatin resistance in gastric cancer.
HER2 (also known as ErbB2), a 185-kDa transmembrane tyrosine kinase (TK) receptor, is a member of the epidermal growth factor receptors (EGFRs) family. This family includes HER1 (also known as EGFR, ErbB1), HER2, HER3 (ErbB3) and HER4 (ErbB4). These receptors share similar molecular structure: an extracellular ligand-binding domain, a short transmembrane domain and an intracellular domain with TK activity (excepting HER3)20. Unlike HER1, HER3 and HER4, HER2 has no ligand20. Recent studies indicate a role of HER2 in the development of many types of human cancer, especially in breast cancer21,22. HER2 overexpression and/or amplification have been detected in 10–34% of invasive breast cancers and correlate with unfavorable patient outcome22. Targeted therapeutic drugs, including monoclonal antibody Herceptin and small molecule tyrosine kinase inhibitors targeting HER2, are playing more and more important roles in breast cancer treatment23,24. HER2 overexpression and/or amplification have also been observed in colon25, bladder26, ovarian27, endometrial28, lung29, uterine cervix30, head and neck31, esophageal32 and gastric carcinomas33. However, up to date, there is no study investigating the role of HER2 in mediating cisplatin-resistance in gastric cancer.
Based on the above knowledge, we hypothesized that HER2 and EMT may be involved in cisplatin resistance in gastric cancer. Herein, we found that HER2 is overexpressed in cisplatin-resistant gastric cancer cell models MGC803/DDP and AGS/DDP. Meanwhile, MGC803/DDP and AGS/DDP cells exhibited EMT-like morphological changes, compared with parental gastric cancer cell lines MGC803 and AGS. At molecular level, the alteration of expression patterns of EMT-related protein markers also implied this phenomenon. More interestingly, EMT in the cisplatin-resistant gastric cancer cells could be abrogated by monoclonal antibody Herceptin, small molecular targeted drug CP724714, or small interfering RNAs (siRNAs) against HER2. Furthermore, we demonstrated that amplification of HER2 or expression of HER2 positively correlated with the expression of EMT-related transcription factor Snail in 382 cases of gastric cancer and HER2/Snail double positive patients had poorer patient outcome compared with single positive or double negative group.
Results
Cisplatin-resistant gastric cancer cell models display higher motility
First of all, we tested cell proliferation rate of cisplatin-resistant gastric cancer cells MGC803/DDP and AGS/DDP. As shown in Fig. 1A, the proliferation rates of parental and cisplatin-resistant cells were similar. Then, we tested the IC50 and the Resistance Index (RI) of MGC803/DDP and AGS/DDP. As shown in Fig. 1B, IC50 of MGC803/DDP and AGS/DDP cells were 4.9 and 6.3 μg/ml respectively and the RI were 14.8 and 9.5 respectively. However, IC50 of MGC803 and AGS cells were 0.33 and 0.66 μg/ml respectively. Interestingly, we found that MGC803/DDP and AGS/DDP cells possess an increased motility compared with parental cells in the wound healing assay, as shown in Fig. 1C,D. Consistently, MGC803/DDP and AGS/DDP cells also showed enhanced migration through the micropore membranes into the lower chambers in the transwell chamber assay (Fig. 1E). The above results demonstrated that cisplatin-resistant gastric cancer cells displayed higher migratory capacity and motility compared with parental cells.

Cisplatin-resistant gastric cancer cell models display higher motility.
(A) Cell growth curve of cisplatin-resistant MGC803 and AGS cells, versus parental MGC803 and AGS cells. Values represented the mean ± SD from two independent experiments with triplicate samples. DDP, cisplatin. (B) IC50 and RI for DDP in drug resistant and parental gastric cancer cells. Values represented the mean ± SD from three independent experiments with triplicate samples. RI, resistance index. (C) Cisplatin-resistant gastric cancer cells exhibit higher wound healing ability. Photos were taken at 0 and 24 h after wounding. (D) Summary of wound healing assays. Results were presented as the mean ± SD of two independent experiments, **P < 0.01 compared with parental cells. (E) Cisplatin-resistant gastric cancer cells possess higher cell migratory capacity in vitro. The results were mean ± SD of three independent experiments with triplicate wells. **P < 0.01.
Cisplatin-resistant gastric cancer cells exhibit an EMT-like phenotypic change
EMT is of paramount importance in a plethora of cancer related events, including cancer metastasis and chemotherapy resistance14,16,17,18. But to the best of our knowledge, the association of EMT with cisplatin resistance in gastric cancer has not been reported. Herein, we found that MGC803/DDP and AGS/DDP cells exhibited a spindle-like fibroblastoid phenotypic change in contrast to parental cell lines MGC803 and AGS (Fig. 2A). FITC-conjugated phalloidin staining of F-actin also revealed that MGC803/DDP and AGS/DDP cells possessed EMT-like morphology compared with their parental cells (Fig. 2B). At molecular level, the expression patterns of EMT protein markers and EMT-related transcription factors were determined by western blot. MGC803/DDP and AGS/DDP cells showed reduced expression of epithelial cell marker ZO1. Meanwhile, the expression of E-cadherin was down-regulated in MGC803/DDP cells. Furthermore, the expression of EMT-related transcription factor Snail was increased in MGC803/DDP and AGS/DDP cells (Fig. 2C).

Cisplatin-resistant gastric cancer cells exhibit an EMT-like phenotypic change.
(A) Representative images of cellular morphology of cisplatin-resistant MGC803/DDP and AGS/DDP cell lines, plus parental MGC803 and AGS cells. (B) FITC-phalloidin staining of F-actin in cisplatin-resistant MGC803/DDP and AGS/DDP cell lines and parental MGC803 and AGS cells. (C) Epithelial marker E-cadherin, ZO1 and EMT-related transcription factor Snail were examined by Western blot.
HER2 is overexpressed and plays a pivotal role in mediating EMT in cisplatin-resistant gastric cancer cells
In the following study, we sought to explore the potential molecular mechanism which is responsible for the EMT-like phenotypic changes in cisplatin-resistant gastric cancer cells. Previous study revealed that HER2 overexpression and/or amplification is an unfavourable predictive factor34. So, we hypothesized that HER2 overexpression and/or amplification may be associated with cisplatin resistance in gastric cancer. As shown in Fig. 3A, HER2 expression was significantly upregulated in cisplatin-resistant gastric cancer cells, especially in MGC803/DDP cells. Next, we found that MGC803/DDP and AGS/DDP cells showed increased HER2 amplification compared with parental MGC803 and AGS cells through qPCR method, indicating that HER2 amplification played an important role in HER2 protein up-regulation (Fig. 3B).

HER2 is overexpressed and both Herceptin incubation and siRNAs against HER2 reversed the EMT in cisplatin-resistant gastric cancer cells.
(A) Western blot of HER2 in MGC803/DDP and AGS/DDP cell lines and parental MGC803 and AGS cells. GAPDH was used as loading control. (B) Relative amplification of HER2 in parental and cisplatin-resistant cells. Results were presented as the mean ± SD of two independent experiments, *P < 0.05 compared with parental cells. (C) Herceptin incubation abrogated EMT morphology in MGC803/DDP cells. Representative images of cellular morphology of MGC803/DDP cells, plus parental MGC803 cells treated with Herceptin for 24 h were shown. Hercep represents Herceptin. (D) Herceptin incubation reversed EMT morphology in MGC803/DDP cells. Representative images of FITC-phalloidin staining of F-actin after 100 μg/ml Herceptin treatment for 24 h were shown. (E) Effects of Herceptin on levels of ZO1 and Snail. (F) CP724714 treatment abolished EMT-like cell morphology. Cells were incubated with 10 μM CP724714 for 24 h. Representative images of cellular morphology of were captured. (G) CP724714 treatment abrogated EMT-like cell morphology. Cells were treated as in Fig. 4F, FITC-phalloidin staining of F-actin was performed and typical images were shown. (H) Effects of CP724714 on ZO1 and Snail. (I) CP724714 inhibited the increased cell migration in cisplatin-resistant gastric cancer cells. Representative images were presented here. (J) CP724714 inhibited the increased cell migration in cisplatin-resistant gastric cancer cells. Values represented the mean ± SD from three independent experiments with triplicate samples. *P < 0.01.
In order to investigate the role of HER2 in mediating EMT in cisplatin-resistant gastric cancer cells, we utilized multiple strategies, including monoclonal antibody Herceptin blocking method, siRNA technique and small molecular targeted therapeutic drug CP724714 treatment. Firstly, cell morphology analysis showed that the fibroblastic, spindle-shaped morphology of MGC803/DDP cells was reversed to the epithelial cell phenotype similar to that of parental counterparts after Herceptin treatment in a dose-dependent manner (Fig. 3C). Herceptin at the concentration of 100 μg/ml completely abrogated the EMT phenomenon observed in MGC803/DDP cells (Fig. 3C). Similar changes were observed by FITC-phalloidin staining for F-actin (Fig. 3D). At molecular level, ZO1 down-regulation and Snail up-regulation were also counteracted by Herceptin treatment in MGC803/DDP cells (Fig. 3E). Taken together, these results suggested that HER2 mediates EMT in cisplatin-resistant gastric cancer cells.
Next, a potent molecular targeted agent against HER2, CP724714, was utilized. CP724714 at the concentration of 10 μM was applied to MGC803/DDP cells for 24 h. As shown in Fig. 3F,G, the morphology of MGC803/DDP cells was also reversed to that of epithelial cells. Meanwhile, ZO1 down-regulation and Snail up-regulation were reversed by CP724714 in MGC803/DDP cells (Fig. 3H). CP724714 significantly lowered the cell migration of MGC803/DDP cells (Fig. 3I,J), suggesting that HER2 activity contributes to increased cell invasiveness in cisplatin-resistant gastric cancer cells.
Thirdly, we employed siRNA strategy. As shown in Fig. 4A, HER2 expressions were knocked down by three pairs of specific siRNAs. Cell morphology analysis and FITC-phalloidin staining assay showed that EMT of MGC803/DDP cells was completely reversed by these siRNAs (Fig. 4B,C). Snail up-regulation and ZO1 down-regulation were reversed by siRNAs in MGC803/DDP cells (Fig. 4D). Meanwhile, cell migration was inhibited by these siRNAs in MGC803/DDP cells (Fig. 4E,F).

SiRNAs against HER2 could abrogate the EMT phenotype and cell invasiveness in cisplatin-resistant gastric cancer cells.
(A) Validation of silencing efficiency of HER2. Cells were transiently transfected with 50 nM HER2-specific siRNAs #1-#3 or a control siRNA for 48 h. (B) Knock-down of HER2 abrogated EMT morphology. Cells were transiently transfected with 50 nM specific siRNAs targeting HER2 for 48 h, Representative images of cellular morphology were shown. (C) Knock-down of HER2 abolished EMT phenotype. Cells were treated as in Fig. 4B. FITC-phalloidin staining of F-actin were performed and representative images were shown. (D) Effects of HER2 knock-down on the levels of ZO1 and Snail. (E) Effects of HER2 knock-down on cell migration. Representative images of transwell cell migration assay were shown. (F) Summary of Fig. 4E. Values represented the mean ± SD from three independent experiments with triplicate samples. *P < 0.01.
Taken together, these data provided evidences that HER2 is required for EMT and cell invasiveness in cisplatin-resistant gastric cancer cells.
HER2 inhibition significantly reverses cisplatin resistance in MGC803/DDP cells
Firstly, we tested whether multiple HER2 inhibition strategies affect the proliferation of MGC803/DDP cells. After transfection with specific siRNA#3, treated with 100 μg/ml Herceptin, or treated with 10 μM CP724714, the proliferation rate remained similar (Fig. 5A). Next, we calculated the IC50 values and Resistance indexes of each panel. As shown in Fig. 5B, the sensitivity of MGC803/DDP cells towards cisplatin was dramatically increased (Fig. 5B). The IC50 values was decreased to 0.9, 0.6, or 0.5 respectively after siRNA against HER2, Herceptin, or CP724714 pre-treatment. These data suggested that HER2 is required for the maintenance of cisplatin resistance in gastric cancer cells. Meanwhile, it also provided potential therapeutic strategies for gastric cancer patients being unresponsive with cisplatin.

HER2 inhibition significantly reverses cisplatin resistance in MGC803/DDP cells.
(A) Cell growth curve of cisplatin-resistant MGC803 cells with different treatments. Values represented the mean ± SD from two independent experiments with triplicate samples. (B) Effects of different treatments on IC50 and RI. Values represented the mean ± SD from three independent experiments with triplicate samples.
HER2/Snail double positive gastric cancer patients have unfavorable outcome
To determine the association of HER2 overexpression and/or amplification with EMT in gastric cancer at tissue levels, we examined HER2 protein expression by immunohistochemistry (IHC) and DNA amplification by fluorescence in situ hybridization (FISH) in a cohort of 382 gastric cancer samples with a 5-year follow-up. Meanwhile, Snail protein expression was also tested by IHC in the same cohort. As shown in Fig. 6A, HER2 expression was positively correlated with Snail expression. In these cases, HER2 amplification was determined as a ratio of HER2 to that of chromosome 17 centromere signal. The typical results of the FISH test were presented in Fig. 6B.

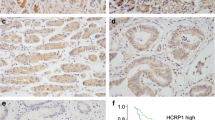
HER2/Snail double positive gastric cancer patients have unfavorable outcome.
(A) Representative immunohistochemical staining of HER2 and Snail by respective antibody in human gastric tissues. Original magnification, 100 × . (B) Representative FISH staining of HER2 by probe in human gastric tissues. Original magnification, 400 × . HER2 amplification was determined as a ratio of HER2 (red dots) and chromosome 17 centromere (green dots) signal counts. Ratios < 2 were determined as no amplification with FISH and those >2 as positive amplification with FISH. “a” represents no amplification; “b” represents positive amplification. (C) Chi-square analysis of the correlation of HER2 expression or amplification with Snail expression. (D) Kaplan-Meier Curve analysis of HER2 amplification with OS for patients with gastric cancer by the log-rank test. (E) Kaplan-Meier estimation of Snail overexpression with OS for patients with gastric cancer by the log-rank test. (F) Kaplan-Meier estimation of HER2/Snail double positive expression versus single positive or both negative counterparts with OS for patients with gastric cancer by the log-rank test.
In this cohort of gastric cancer patients, 19.9% (76/382) by IHC and 20.4% (78/382) by FISH were positive for HER2 (Table 1). 42.7% (109/382) by IHC were positive for Snail (Table 1). Although HER2 expression and/or amplification exhibited no link with patient’s gender, age, tumor size, or tumor differentiation, significant correlations with depth of invasion, lymph node metastasis, TNM staging, vascular invasion and metastasis were observed (Table 1). Snail expression obviously correlated with tumor size, differentiation, depth of invasion, lymph node metastasis, TNM staging, vascular invasion and metastasis (Table 1). Next, Chi-square statistical analysis was employed to evaluate the correlation of HER2 overexpression and/or amplification with Snail expression. The results showed that expression of Snail positively correlated with HER2 expression or HER2 amplification (Fig. 6C).
To analyze the correlation of HER2 expression/amplification and Snail expression with patients’ outcome, we performed patient survival analysis. The Kaplan-Meier plotting showed that gastric cancer patients with increased HER2 amplification had a poorer overall survival (OS) than those with HER2-negative counterparts (Fig. 6D). Gastric cancer patients with Snail-positive expression also had a poorer OS than those with Snail-negative expression (Fig. 6E). These two findings were consistent with previous reports by other labs34,35,36. Importantly, we found gastric cancer patients with HER2/Snail double positive amplification/expression had worst OS than those with single positive expression/amplification or both negative groups (Fig. 6F). These data indicated that combined testing of HER2 and Snail expression and/or amplification had a significantly prognostic value for determining the survival of gastric cancer patients.
Discussion
Gastric cancer remains the second leading cause of cancer mortality in the world37. Surgical resection is the primary option of treatment and can cure patients with early-stage cancer. However, many gastric cancer patients are diagnosed when the tumor is at an unresectable stage. For these persons, application of chemotherapeutic agents singly or in combination remains mainstream treatment. Cisplatin, as a first-line chemotherapeutic drug for gastric cancer, could trigger apoptosis by inducing DNA damage through crosslinking of the DNA38. However, cancer cells often develop multiple mechanisms to overcome cisplatin-induced DNA damage and apoptosis, leading to cisplatin resistance39,40. Therefore, investigation of the molecular mechanism conferring chemotherapy resistance is urgently needed.
Although HER2 plays a povital role in gastric cancer progression and prognosis34, the molecular mechanisms of HER2 amplification and/or overexpression in mediating gastric cancer-related biological behaviors is not yet fully understood. To our knowledge, this is the first study investigating the association of HER2 with cisplatin resistance in gastric cancer cells.
Herein, we found that HER2 protein is overexpressed in cisplatin-resistant gastric cancer cells compared to parental cells, likely due to HER2 gene amplification. Moreover, we found that these cells underwent an EMT-like morphological alteration. EMT is associated with cancer aggressiveness, invasive and metastatic potential and chemotherapeutic resistance14,15,16,17,18. In recent decade, the molecular mechanisms and signaling pathways mediating EMT were extensively studied, leading to the discovery of several pathways involved in the loss of epithelial cell polarity and the acquisition of mesenchymal phenotypic traits41,42,43. However, there is few study linking HER2 and EMT with cisplatin resistance in gastric cancer. In this study, we found that HER2 upregulation is responsible for EMT phenomenon and these events are associated with cisplatin resistance in gastric cancer cells. It was demonstrated that progression of carcinoma cells to metastatic tumor cells frequently involved EMT-like epithelial plasticity changes towards a migratory, fibroblastoid phenotype, particularly evident at the invasive front of human tumors44. Our current study suggests that EMT is not only a cause of cisplatin resistance in gastric cancer, it may also be a consequence of cisplatin resistance in gastric cancer which results in increased cancer metastasis and tumor relapse after cisplatin treatment for the unresponsive patients.
Herceptin is a monoclonal antibody which specifically targets HER2 protein by directly binding the extracellular domain of the receptor. Herceptin enhances survival rates in both primary and metastatic HER2-positive breast cancer patients45,46. The efficacy of Herceptin in breast cancer patients has led to its use in other HER2-positive cancer patients, including gastric cancer47,48,49. In this study, we found that gastric cancer patients with HER2 overexpression and/or amplification had a more unfavourable outcome. Kaplan Meier curve analysis demonstrated that Snail is another prognostic factor in gastric cancer progression, which is consistent with previous report36. Our study also suggested that combined testing of HER2 and Snail expression in gastric cancer would provide more useful information for patient prognosis, especially for those respond badly to cisplatin, however more efforts are required to validate this assumption. It is reported that HER2 is upregulated after onset of acquired resistance to cisplatin and fluorouracil combination chemotherapy in gastric cancer patients (P = 0.0065)50. The microarray data presented in this article implies that HER2 is upregulated in cisplatin-resistant gastric cancer samples. Furthermore, the mechanism of cisplatin resistance-induced HER2 overexpression in gastric cancer and the signaling pathway mediating HER2-upregulation-induced EMT in cisplatin-resistant gastric cancer cells also need to be elucidated in the future.
In conclusion, this study links HER2 overexpression-mediated EMT with cisplatin resistance in gastric cancer for the first time. Our study also suggests that targeting both HER2 and Snail would be a useful therapeutic strategy for the prevention of gastric cancer metastasis.
Methods
Cell culture
Human gastric cancer cell line MGC803 was kept in Peking University Cancer Hospital & Institute. Human gastric cancer cell line AGS was obtained from ATCC (American Type Culture Collection). MGC803 was from a 53-year-old Chinese male with poorly differentiated gastric mucinous adenocarcinoma51. AGS was from a 54-year-old Caucasian female with poorly differentiated gastric adenocarcinoma. The above two cell lines were cultured in RPMI-1640 medium supplemented with 10% fetal bovine serum (FBS) in 5% CO2 at 37 °C. The culture media and FBS were obtained from Invitrogen (Carlsbad, CA, US). Cisplatin was obtained from Sigma-Aldrich (St. Louis, MO, USA). The cisplatin-resistant MGC803/DDP cells were developed from the parental MGC803 cells that were subjected to gradient exposure to cisplatin as described in52. The cisplatin-resistant AGS/DDP cells were obtained by the same way.
Reagents and antibodies
FITC-phalloidin (P5282) was purchased from Sigma-Aldrich, dissolved in methanol, aliquoted and stored at –20 °C according to manufacturer’s instructions. EMT antibody sampler kit (9782) was purchased from Cell Signaling (Danvers, MA, US). Monoclonal antibody against HER2 (ZM-0065) was purchased from Zhongshan Golden Bridge Biologicals (Beijing, China). Polyclonal antibody against Snail (NBP2-27293SS) was purchased from Novus Biologicals (Littleton, CO, US). Polyclonal antibody against ZO-1 (ab59720) was purchased from Abcam (Cambridge, MA, US). CP724714 (S1167) was purchased from Selleck Chem (Shanghai, China). 3-(4,5-cimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) and dimethyl sulphoxide (DMSO) were purchased from Sigma-Aldrich.
Western blot
Cells were harvested with a plastic scraper and then washed twice with cold PBS. The cells were then homogenized in lysis buffer (25 mM Tris-HCl pH 7.4, 150 mM NaCl, 1 mM EDTA, 1% NP-40, 10% glycerol and 1x complete protease inhibitors). The proteins of the lysates were quantified with BCATM Protein Assay Kit (Thermo). 50 μg of total proteins were subjected to SDS-PAGE and Western blot as described in53.
Quantitative PCR (qPCR) analysis of HER2 amplification
qPCR was performed on an ABI7300 thermocycler (Life Technologies Corporation) by a previously described method54. Primers of HER2 and IGF1 (synthesized by Shanghai Sangon) were as follows: HER2 forward primer 5′-GAACTGGTGTATGCAGATTGC-3′, HER2 reverse primer 5′-AGCAAGAGTCCCCATCCTA-3′, IGF1 forward primer 5′-AGCTCGGCATAGTCTT-3′, IGF1 reverse primer 5′-CCAAGTGAGGGGTGTGA-3′. The standard amplification protocol consists of an initial denaturation step at 95 °C for 10 min, followed by 50 amplification cycles at 95 °C for 10 sec, 55 °C for 5 sec and 72 °C for 10 sec.
Cell Mobility Assay
Cell mobility was assessed using a wound healing assay. The parental and cisplatin-resistant gastric cancer cells were seeded into six-well plates and cultured to monolayers, which were then wounded using sterile pipette tips and any cellular debris was removed by washing with PBS. The wounded monolayers were then incubated in medium containing 10% FBS for 24 h. Photos were captured at 0 and 24 h after wounding.
Cell migration assay
Tissue culture-treated 6.5-mm Transwell chamber with 8.0-μm pore membranes (Corning, Corning, NY, US) was used in the cell migration assay. The assay was performed as described in55.
Immunofluorescence
Cells were grown on the coverslips and fixed with 4% fresh paraformaldehyde for 10 min at room temperature, followed by blocking with 5% bovine serum albumin (BSA) at room temperature for 1 h. Next, cells were stained with FITC-Phalloidin for 1 h at room temperature in dark. After washing, cells were counterstained with DAPI for 10 min and mounted on 50% glycerol/PBS. A Leica SP2 confocal microscope (Leica Microsystems, Dresden, Germany) was used to observe the distribution of F-actin.
SiRNA transfection
Cells were plated in 12-well plates and transfected with siRNA mate (GenePharma, Shanghai, China) according to the manufacturer’s protocol. The target sequences were as follows: HER2 #1 5′-ATCACAGGTTACCTATACA-3′, #2 5′-TGTCAGTATCCAGGCTTTGTA-3′, #3 5′-AAATTCCAGTGGCCATCAA-3′. Negative control siRNA sequence was 5′-ACACGAGAUAAUAUCGACUUG-3′. siRNAs were synthesized by GenePharma.
The MTT cell proliferation assay
1 × 104 cells were plated in 96-well plates before experiments. After HER2 siRNA transfection for 24 h, 100 μg/ml Herceptin pre-treatment for 2 h or 10 μM CP724714 pre-treatment for 2 h, different concentrations of cisplatin (0.1, 0.5, 2.5, 12.5 and 62.5 μg/ml) were applied for 72 h. Next, 10% MTT was added to the wells. After incubated at 37 °C for 4 h, the mixture reacted in culture media was centrifuged at 4000 rpm for 15 min. The precipitates were dissolved in DMSO. Absorbance was measured using a multiplate reader at the wavelength of 490 nm. Cell Proliferation Rate = Absorbance of drug treatment panel/Absorbance of control panel × 100%. Resistance Index = IC50 value of resistant cells/IC50 value of parental cells.
Specimen and immunohistochemistry (IHC)
The study with clinical samples was approved by the Medical Ethic Committee of Zhejiang Provincial People’s Hospital. One cohort of formalin fixed and paraffin embedded (FFPE) gastric cancer tissues were obtained from archives of the Department of Pathology, Zhejiang Provincial People’s Hospital, which had 382 cases collected during 1998-2004. Written Informed Consents were obtained from all patients prior to operation. Specimens were diagnosed histopathologically and staged according to the TNM-International Union against Cancer classification system. IHC was performed to detect HER2 and Snail. The degree of immunostaining was reviewed and scored independently by two pathologist (Z.Z. and G.R.) based on the intensity of staining: 0 (no staining), 1 (weak staining = light yellow), 2 (moderate staining = yellow brown) and 3 (strong staining = brown). Moderate and strong stainings were defined as positive, while no and weak stainings were defined as negative.
Fluorescence in situ hybridization (FISH)
FISH was performed on fixed-paraffin-embedded samples in the same cohort containing 382 gastric cancer cases. FISH experiments were performed according to the protocol given by the supplier (PathVysion kit, Vysis, Downers Grove, IL, US). The centromeric probe of chromosome 17 was included in FISH analyses in 382 cases. In these cases, HER2 amplification was determined as a ratio of HER2 and chromosome 17 centromere signal counts. Ratios ≤2 were determined as no amplification and those >2 were defined as positive amplification
Human rights statement and informed consent
The study with clinical samples was approved by the Medical Ethic Committee of Zhejiang Provincial People’s Hospital and was conducted in accordance with the Helsinki Declaration. Informed consent was obtained from all patients for being included in the study.
Statistical analysis
Data were presented as mean ± SD. The differences were analyzed by ANOVA using SPSS 22.0 software and P < 0.05 was considered statistically significant. IC50 values were calculated using Graphpad Prism software.
Additional Information
How to cite this article: Huang, D. et al. Cisplatin resistance in gastric cancer cells is associated with HER2 upregulation-induced epithelial-mesenchymal transition. Sci. Rep. 6, 20502; doi: 10.1038/srep20502 (2016).
References
Parkin, D. M., Pisani, P. & Ferlay, J. Estimates of the worldwide incidence of 25 major cancers in 1990. Int J Cancer 80, 827–841 (1999).
Hohenberger, P. & Gretschel, S. Gastric cancer. Lancet 362, 305–315 (2003).
Zhang, D. & Fan, D. New insights into the mechanisms of gastric cancer multidrug resistance and future perspectives. Future Oncol 6, 527–537 (2010).
Rosenberg, B., VanCamp, L., Trosko, J. E. & Mansour, V. H. Platinum compounds: a new class of potent antitumour agents. Nature 222, 385–386 (1969).
Kang, Y. K. et al. Capecitabine/Cisplatin Versus 5-Fluorouracil/Cisplatin as First-line Therapy in Patients with Advanced Gastric Cancer: A Randomised Phase III Non inferiority Trial. Ann Oncol 20, 666–673 (2009).
Yu, P. F. et al. Significance of multidrug resistance gene-associated proteins in the postoperative adjuvant chemotherapy for gastric carcinoma and the prognosis. Zhonghua Wei Chang Wai Ke Za Zhi 13, 289–293 (2010).
Scheffer, G. L. et al. The drug resistace-related protein LRP is the vault protein. Nature Med 1, 578–582 (1995).
Hu, W. Q., Peng, C. W. & Li, Y. The expression and significance of P-glycoprotein, lung resistance protein and multi-drug-resistance-associated protein in gastric cancer. Exp Clin Cancer Res 28, 144 (2009).
Gianni, L. Anthracycline resistance: the problem and its current definition. Semin Oncol 24, 10–17 (1997).
Hay, E. D. An overview of epithelio-mesenchymal transformation. Acta Anat 154, 8–20 (1995).
Kalluri, R. & Weinberg, R. A. The basics of epithelial-mesenchymal transition. J Clin Invest 119, 1420–1428 (2009).
Thiery, J. P., Acloque, H., Huang, R. Y. & Nieto, M. A. Epithelial-mesenchymal transitions in development and disease. Cell 139, 871–890 (2009).
López-Novoa, J. M. & Nieto, M. A. Inflammation and EMT: an alliance towards organ fibrosis and cancer progression. EMBO Mol Med 1, 303–314 (2009).
Keshamouni, V. G. & Schiemann, W. P. EMT in Tumor Metastasis: A Method to the Madness. Future Oncol 8, 1109–1111 (2009).
Scheel, C. & Weinberg, R. A. Cancer stem cells and epithelial mesenchymal transition: concepts and molecular links. Semin Cancer Biol 22, 396–403 (2012).
Wang, X. et al. Identification of a novel function of TWIST, a bHLH protein, in the development of acquired taxol resistance in human cancer cells. Oncogene 23, 474–482 (2004).
Yang, A. D. et al. Chronic oxaliplatin resistance induces epithelial-to-mesenchymal transition in colorectal cancer cell lines. Clin Cancer Res 12, 4147–4153 (2006).
Kajiyama, H. et al. Chemoresistance to paclitaxel induces epithelial-mesenchymal transition and enhances metastatic potential for epithelial ovarian carcinoma cells. Int J Oncol 31, 277–283 (2007).
Shah, A. N. et al. Development and characterization of gemcitabine-resistant pancreatic tumor cells. Ann Surg Oncol 14, 3629–3637 (2007).
Mendelsohn, J. & Baselga, J. The EGF receptor family as targets for cancer therapy. Oncogene 19, 6550–6565 (2000).
Slamon, D. J. et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science 244, 707–712 (1989).
Kaptain, S., Tan, L. K. & Chen, B. Her–2/neu and breast cancer. Diagn Mol Pathol 10, 139–152 (2001).
Nahta, R. Molecular mechanisms of trastuzumab-based treatment in HER2-overexpressing breast cancer. ISRN Oncol 2012, 428062 (2012). doi: 10.5402/2012/428062.
Goldenberg, M. M. Trastuzumab, a recombinant DNA-derived humanized monoclonal antibody, a novel agent for the treatment of metastatic breast cancer. Clin Ther 21, 309–318 (1999).
Schuell, B., Gruenberger, T., Scheithauer, W., Zielinski, C. H. & Wrba, F. HER 2/neu protein expression in colorectal cancer. BMC Cancer 8, 123 (2006).
Eltze, E. et al. Cox-2 and Her2/neu co-expression in invasive bladder cancer. Int J Oncol 26, 1525–1531 (2005).
McKenzie, S. J. et al. Serum levels of HER-2 neu (C-erbB-correlate with overexpression of p185neu in human ovarian cancer. Cancer 71, 3942–3946 (1993).
Hetzel, D. J. et al. HER-2/neu expression: a major prognostic factor in endometrial cancer. Gynecol Oncol 47, 179–185 (1992).
Hirashima, N., Takahashi, W., Yoshii, S., Yamane, T. & Ooi, A. Protein overexpression and gene amplificationof c-erbB-2 in pulmonary carcinomas: a comparative immunohistochemical and fluorescence in situ hybridization study. Mod Pathol 14, 556–662 (2001).
Mitra, A. B., Murty, V. V., Pratap, M., Sodhani, P. & Chaganti, R. S. ERBB2 (HER2/neu) oncogene is frequently amplified in squamous cell carcinoma of the uterine cervix. Cancer Res 54, 637–639 (1994).
Beckhardt, R. N. et al. HER-2/neu oncogene characterization in head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg 121, 1265–1270 (1995).
Reichelt, U. et al. Frequent homogenous HER-2 amplification in primary and metastatic adenocarcinomas of the esophagus. Mod Path 20, 120–129 (2007).
Lemoine, N. R. et al. Amplification and overexpression of the EGF receptor and c-erbB-2 proto-oncogenes in human stomach cancer. Br J Cancer 64, 79–83 (1991).
Gravalos, C. & Jimeno, A. HER2 in gastric cancer: a new prognostic factor and a novel therapeutic target. Ann Oncol 19, 1523–1529 (2008).
Boku, N. Her2-positive gastric cancer. Gastric Cancer 17, 1–12 (2014).
Shin, N. R. et al. Overexpression of Snail is associated with lymph node metastasis and poor prognosis in patients with gastric cancer. BMC Cancer 12, 521 (2012).
Ferlay, J. et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127, 2893–2917 (2010).
Tanner, M. et al. Topoisomerase Ilalpha gene amplification predicts favorable treatment response to tailored and dose-escalated anthracycline-based adjuvant chemotherapy in HER-2/neu-amplified breast cancer. J Clin Oncol 24, 2428–2436 (2006).
Cho, H. J. et al. VEGF-C mediates RhoGDI2-induced gastric cancer cell metastasis and cisplatin resistance. Int J Cancer 135, 1553–1563 (2014).
Cho, H. J. et al. RhoGDI2 confers gastric cancer cells resistance against cisplatin-induced apoptosis by upregulation of Bcl-2 expression. Cancer Lett 311, 48–56 (2011).
Thiery, J. P. & Sleeman, J. P. Complex networks orchestrate epithelial-mesenchymal transitions. Nat Rev Mol Cell Biol 7, 131–142 (2006).
Huber, M. A. et al. NF-kappaB is essential for epithelial-mesenchymal transition and metastasis in a model of breast cancer progression. J Clin Invest 114, 569–581 (2004).
Lamouille, S., Xu, J. & Derynck, R. Molecular mechanisms of epithelial–mesenchymal transition. Nat Rev Mol Cell Biol 15, 178–196 (2014).
Yang, J. & Weinberg, R. A. Epithelial-mesenchymal transition: At the crossroads of development and tumor metastasis. Dev Cell 14, 818–829 (2008).
Vogel, C. L. et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol 20, 719–726 (2002).
Romond, E. H. et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 353, 1673–1684 (2005).
Bang, Y. J. et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 376, 687–697 (2010).
Fujimoto-Ouchi, K. et al. Antitumor activity of trastuzumab in combination with chemotherapy in human gastric cancer xenograft models. Cancer Chemother Pharmacol 59, 795–805 (2007).
Yu, G. Z., Chen, Y. & Wang, J. J. Overexpression of Grb2/HER2 signaling in Chinese gastric cancer: their relationship withclinicopathological parameters and prognostic significance. J Cancer Res Clin Oncol 135, 1331–1339 (2009).
Kim, H. K. et al. A Gene Expression Signature of Acquired Chemoresistance to Cisplatin and Fluorouracil Combination Chemotherapy in Gastric Cancer Patients. PLoS ONE 6, e16694 doi: 10.1371/journal.pone.0016694 (2011).
Wang, Z. H. et al. Establishment and preliminary observation on biological characteristics of human gastric Mucinous adenocarcinoma cell line MGC803. Acta Biologiae Experimentalis Sinica 16, 257–262 (1983).
Huang, H. et al. Establishment of drug resistant cell line of MGC803 and analysis of differential secretome. Beijing Da Xue Xue Bao 46, 183–189 (2014).
Duan, H., Qu, L. & Shou, C. Mycoplasma hyorhinis induces epithelial-mesenchymal transition in gastric cancer cell MGC803 via TLR4-NF-κB signaling. Cancer Lett 354, 447–454 (2014).
Hillig, T. et al. Assessing HER2 amplification by IHC, FISH and real-time polymerase chain reaction analysis (real-time PCR) following LCM in formalin-fixed paraffin embedded tissue from 40 women with ovarian cancer. APMIS 120, 1000–1007 (2012).
Duan, H. Y. et al. Mycoplasma hyorhinis infection promotes NF-κB-dependent migration of gastric cancer cells. Cancer Res 74, 5782–5794 (2014).
Acknowledgements
The authors thank Dr. Zhihua Tian (Peking University Cancer Hospital and Institute) for providing critical technical assistance. This work was supported by Zhejiang Provincial Department of Science and Technology Research Foundation 2008C33040 and National Basic Research Program of China (2015CB553906). The authors declare that sponsor had no involvement in the study design, in the collection, analysis and interpretation of data, in the writing of the manuscript, or in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
Conception and design: D.H., H.D. and Z.Z. Development of methodology: D.H., H.D. and H.H. Acquisition of data (provided animals, acquired and managed patients, provided facilities, etc.): H.D., G.R. and Z.Z. Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational analysis): D.H., H.D., H.H., X.T., Y.H., L.Q., G.R., C.S. and Z.Z. Writing, review, and/or revision of the manuscript: D.H., H.D., X.T., L.Q., C.S. and Z.Z. Administrative, technical, or material support (i.e., reporting or organizing data, constructing databases): H.H., L.Q., G.R. and C.S. Study supervision: L.Q., C.S. and Z.Z.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Huang, D., Duan, H., Huang, H. et al. Cisplatin resistance in gastric cancer cells is associated with HER2 upregulation-induced epithelial-mesenchymal transition. Sci Rep 6, 20502 (2016). https://doi.org/10.1038/srep20502
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep20502
- Springer Nature Limited
This article is cited by
-
The role of m6A methylation in therapy resistance in cancer
Molecular Cancer (2023)
-
Mechanism of cisplatin resistance in gastric cancer and associated microRNAs
Cancer Chemotherapy and Pharmacology (2023)
-
Targeting mitochondria as a therapeutic anti-gastric cancer approach
Apoptosis (2022)
-
High expression of NEK2 promotes gastric cancer progression via activating AKT signaling
Journal of Physiology and Biochemistry (2021)
-
Simultaneously target of normal and stem cells-like gastric cancer cells via cisplatin and anti-CD133 CAR-T combination therapy
Cancer Immunology, Immunotherapy (2021)